


Breast milk is the ideal food for newborns and infants. Although babies may be fed breast milk or formula, the World Health Organization (WHO) and American Academy of Pediatrics (AAP) recommend exclusive breastfeeding if possible for about 6 months, with introduction of solid foods thereafter. Other organizations suggest parents introduce solid foods between 4 months and 6 months of age while continuing breastfeeding. Signs that a baby is ready for solid foods include good head and neck control, ability to sit upright when supported, interest in food, opening their mouth when offered food on a spoon, and swallowing food rather than pushing it back out. Most babies start to show these signs by 6 months of age. Introducing solid foods before 4 months of age is not recommended. Introducing peanut- and egg-containing foods before 12 months of age is encouraged because there is evidence that this may prevent the development of allergy to these foods.
After children reach 1 year of age, breastfeeding may continue, depending on the preferences of the mother. However, after age 1 year, breastfeeding should complement a full diet of solid foods and other fluids.
Sometimes breastfeeding is not possible (for example, if the mother is taking certain medications while breastfeeding), and many healthy babies have been raised on formula.
(See also Overview of Feeding of Newborns and Infants and Overview of the Postdelivery (Postpartum) Period.)
Benefits of Breastfeeding
Breastfeeding is good for the mother and the baby. Breast milk
Provides the baby with the necessary nutrients in the most easily digestible and absorbable form
Contains antibodies and white blood cells that protect the baby against infection
The first milk the mother produces is a thin yellow fluid called colostrum. Colostrum is particularly rich in calories, protein, white blood cells, and antibodies.
The breast milk that is produced after colostrum helps maintain the correct pH of the stool and the proper balance of normal intestinal bacteria, thus protecting the baby against bacterial diarrhea. Because of the protective qualities of breast milk, many types of infections occur less often in babies who are breastfed rather than formula-fed. Breastfeeding also seems to protect against the development of certain chronic problems, such as allergies, diabetes, obesity, and Crohn disease. Most commercial formulas are now supplemented with certain fatty acids (arachidonic acid [ARA] and docosahexaenoic acid [DHA]) to more closely resemble breast milk and perhaps promote optimal neurologic development in formula-fed babies.
Breastfeeding offers many advantages to the mother as well, such as
Helping her to bond and feel close to her baby in a way that bottle-feeding cannot
Allowing her to recover more quickly after delivery
Providing her with some long-term health benefits
Long-term health benefits of breastfeeding include decreased risk of obesity, osteoporosis, ovarian cancer, and some breast cancers.
If the mother follows a healthy, varied diet, normal-term infants who are breastfed do not need vitamin or mineral supplements, except for vitamin D and sometimes fluoride. Infants who are fed only breast milk are at risk of If the mother follows a healthy, varied diet, normal-term infants who are breastfed do not need vitamin or mineral supplements, except for vitamin D and sometimes fluoride. Infants who are fed only breast milk are at risk ofvitamin D deficiencyvitamin D deficiency after 2 months of age, particularly if they are premature, have dark skin, or have limited exposure to sunlight (for example, infants who live in northern climates). These infants are given vitamin D supplements beginning at 2 months of age. After 6 months of age, infants in homes where the water does not have adequate fluoride (supplemental or natural) should be given fluoride drops. Parents can obtain information about the fluoride content of their water from a local dentist or health department.after 2 months of age, particularly if they are premature, have dark skin, or have limited exposure to sunlight (for example, infants who live in northern climates). These infants are given vitamin D supplements beginning at 2 months of age. After 6 months of age, infants in homes where the water does not have adequate fluoride (supplemental or natural) should be given fluoride drops. Parents can obtain information about the fluoride content of their water from a local dentist or health department.
Infants who are under 6 months of age should not be given additional plain water. Plain water is unnecessary and it also may cause the level of sodium in their blood to become too low (a disorder called hyponatremia).
Breastfeeding Procedure
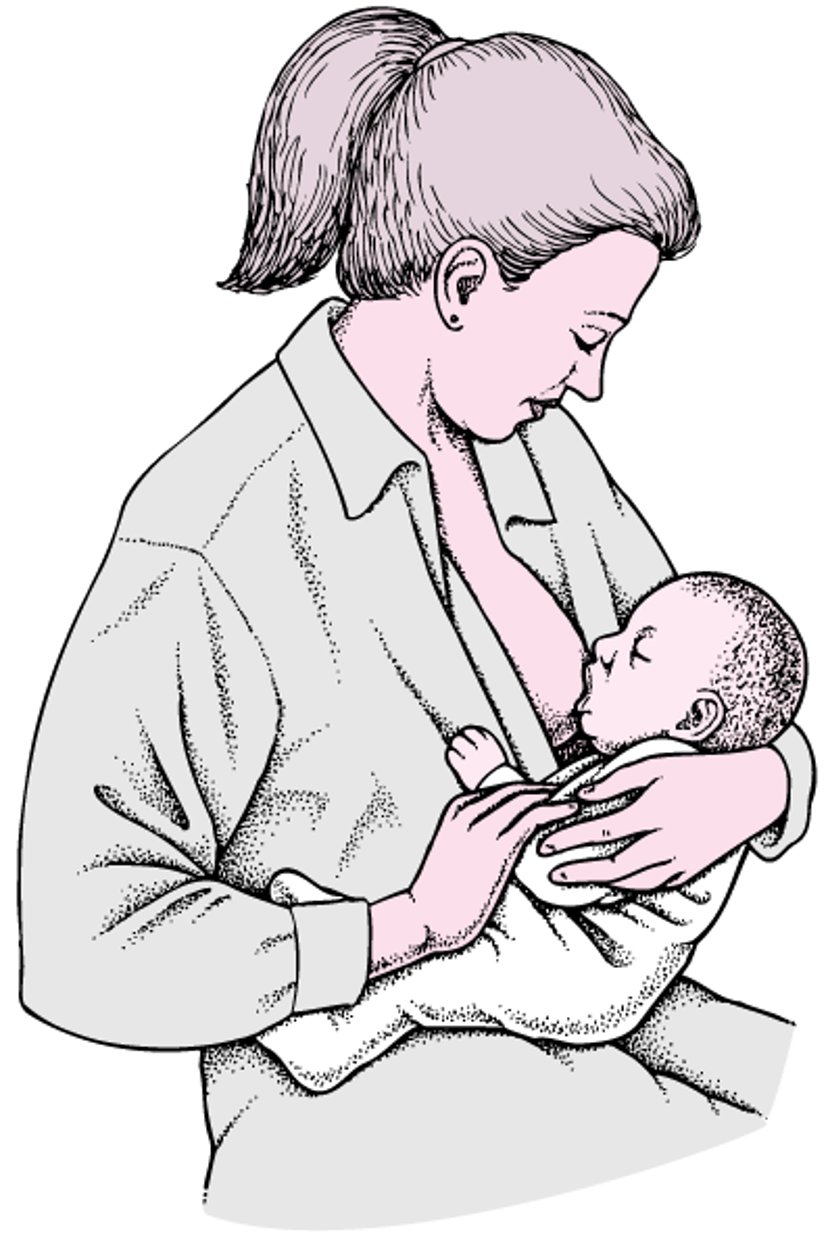
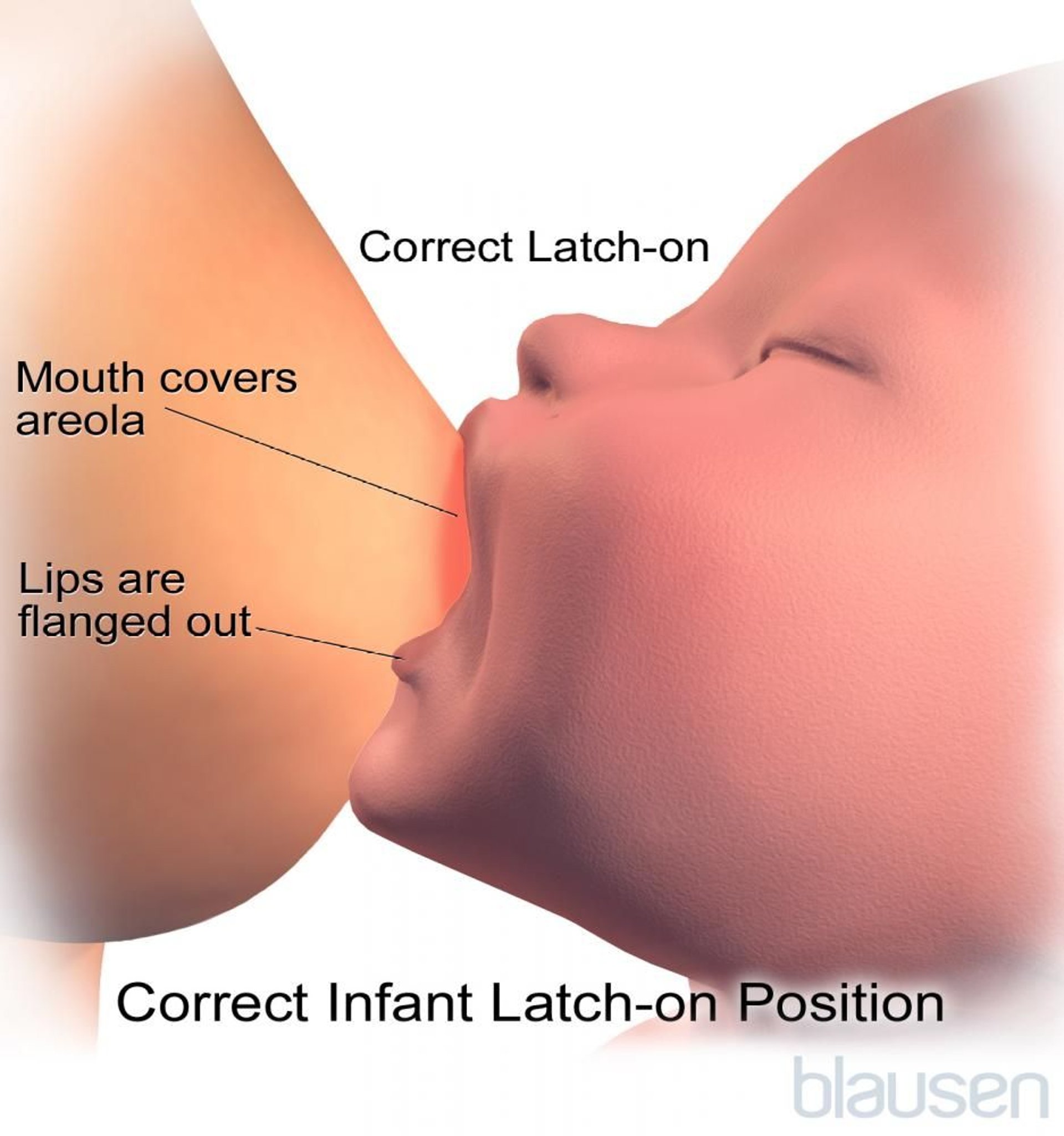
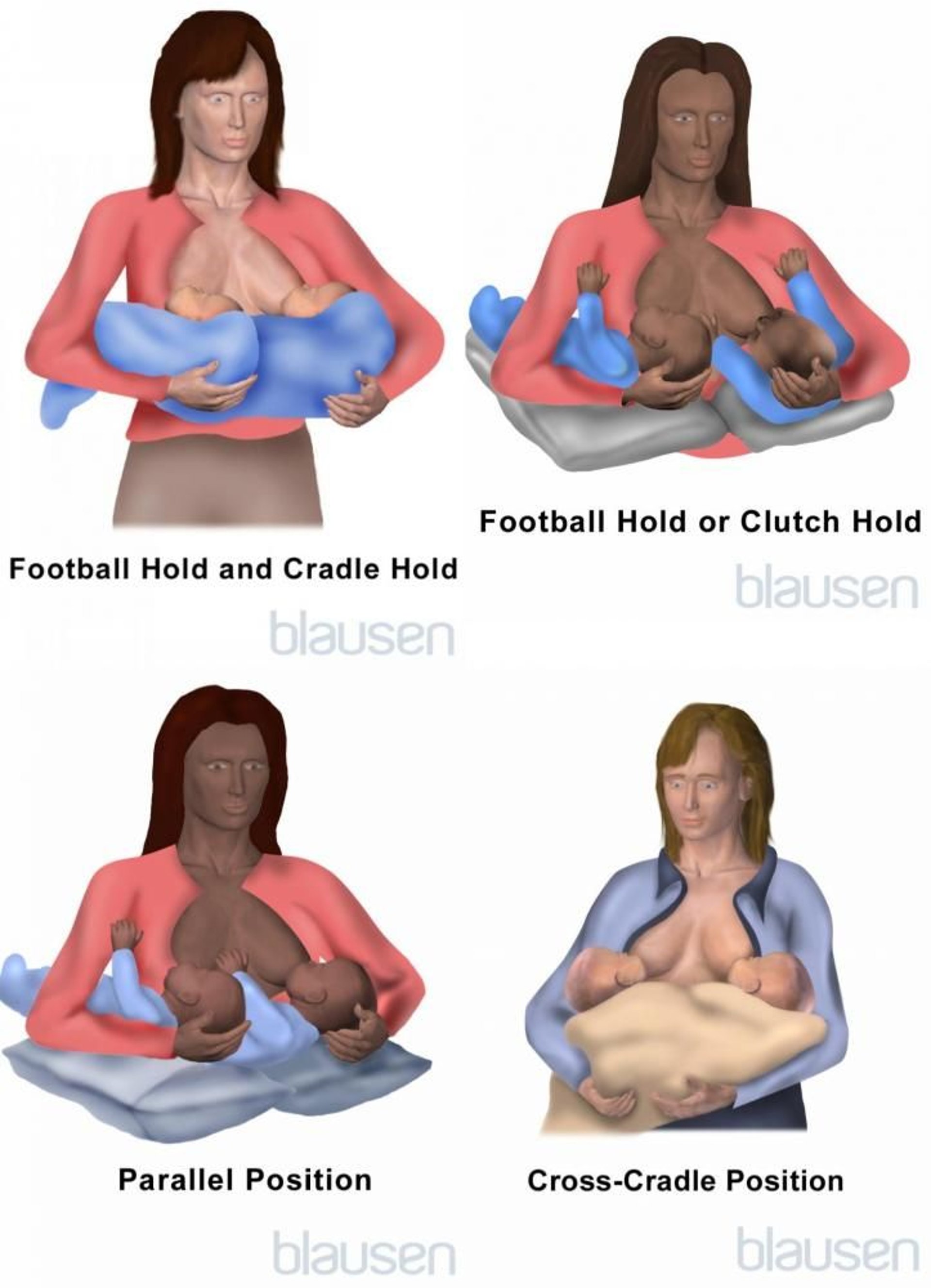
To begin breastfeeding, the mother settles into a comfortable, relaxed position, either seated or lying almost flat. The mother should be able to comfortably turn from one side to the other to offer each breast. The baby faces the mother. The mother supports her breast with her thumb and index finger on top and other fingers below and brushes her nipple against the middle of the baby's lower lip, which stimulates the baby's mouth to open (the rooting reflex) and grasp the breast. As the mother eases the nipple and areola into the baby's mouth, she makes sure the nipple is centered, which helps keep the nipple from becoming sore. Before removing the baby from the breast, the mother breaks the suction by inserting her finger into the baby's mouth and gently pressing the baby's chin down. Sore nipples result from poor positioning and are easier to prevent than to cure.
Positioning a Baby to Breastfeed
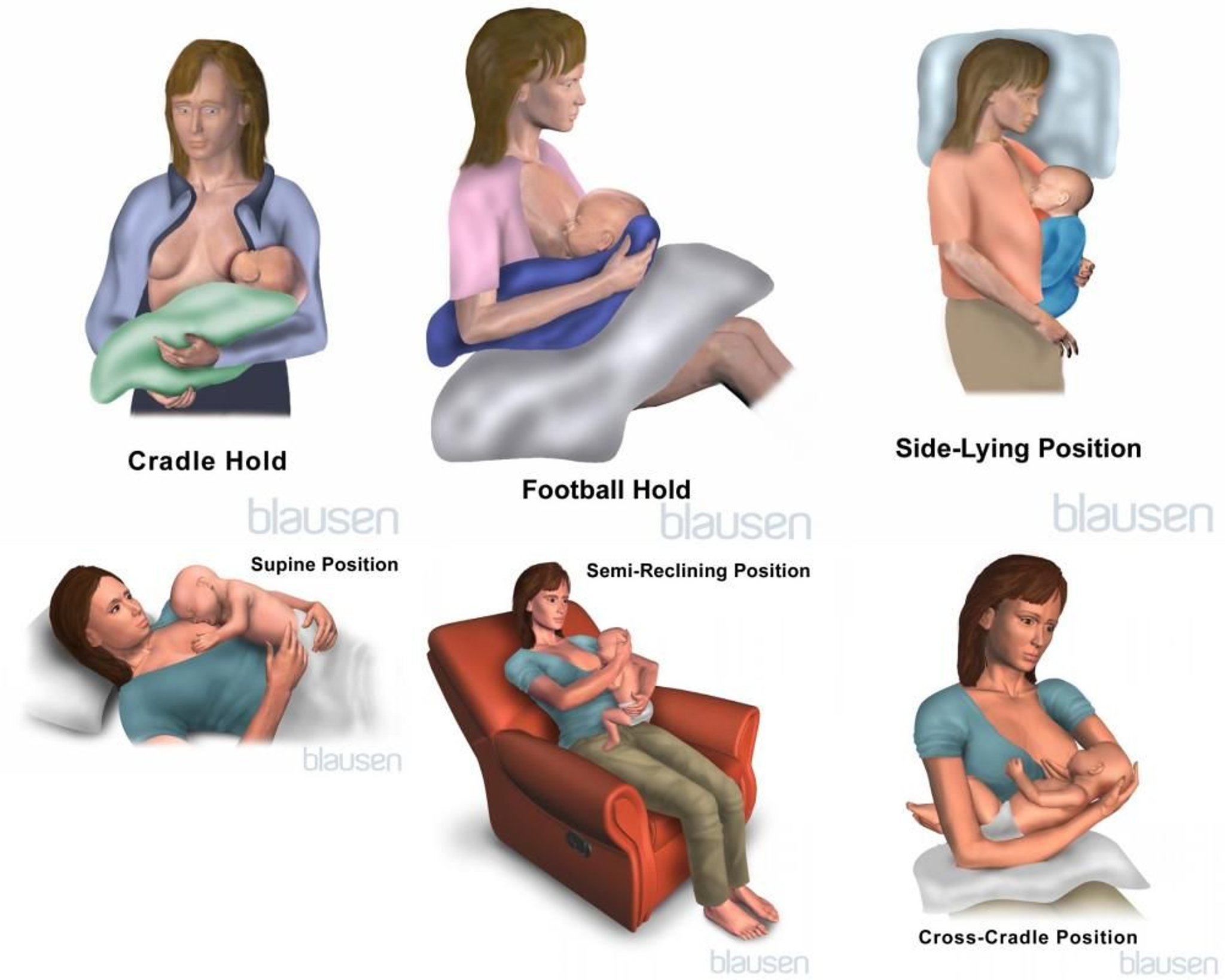
The mother settles into a comfortable, relaxed position. She may sit or lie almost flat, and she may hold the baby in several different positions. A mother should find the position that works best for her and her baby. She may wish to alternate among different positions. A common position is holding the baby on the lap so that the baby is facing the mother, stomach to stomach. The mother supports the baby's neck and head with her left arm when the baby is feeding on the left breast and with her right arm when the baby is feeding on the right breast. The baby is brought to the level of the breast, not the breast to the baby. Support for the mother and the baby is important. Pillows can be placed behind the mother's back or under her arm. Placing her feet on a footstool or coffee table may help keep her from leaning over the baby. Leaning over may strain her back and result in a poor latch. A pillow or folded blanket may be placed under the baby for added support. |





Initially, the baby should feed for several minutes at each breast. The resulting reflex in the mother called the let-down reflex triggers milk production. The production of milk depends on sufficient suckling time, so feeding times should be long enough for milk production to be fully established. During the first few weeks, the baby should be encouraged to nurse on both breasts with each feeding. However, some babies fall asleep while feeding at the first breast. Burping the infant and switching to the other breast helps keep the infant awake. The breast used last should be used first for the next feeding.

For a first baby, full milk production is usually established in 72 to 96 hours. For subsequent babies, milk production is established earlier. No more than 6 hours should elapse between feeding sessions during the first few days in order to stimulate breast milk production. Feeding should be on demand (the baby's, that is) rather than by the clock. Similarly, the length of each breastfeeding session should be adjusted to meet the baby's needs. Babies should be nursed on demand, which is typically 8 to 12 times in a 24-hour period, but this guideline varies widely.

Mothers who work may breastfeed while at home and have the baby drink pumped breast milk from a bottle during the hours they are away. Pumped breast milk should be immediately refrigerated if it is to be used within 2 days and should be immediately frozen if it is to be used after 2 days. Refrigerated milk that is not used within 4 days should be thrown away because the risk of contamination by bacteria is high. Frozen milk should be thawed by placing it in warm water. Breast milk should not be heated in a microwave.
Complications of Breastfeeding for the Baby
The main complication caused by breastfeeding is
Because mothers cannot tell exactly how much milk a baby takes, mothers should take the baby to the doctor 3 to 5 days after delivery so that the doctor can find out how breastfeeding is going, weigh the baby, and answer any questions. A doctor may need to see the baby earlier if the baby was discharged within 24 hours or is not feeding well, or if the parents have a particular concern.
Doctors use frequency of feeding, number of urine and stool diapers, and weight gain to tell whether milk production is adequate. Parents can get a rough idea of whether their baby is getting enough milk by counting diapers. By 5 days of age, wetting fewer than 6 diapers a day and/or having fewer than 4 bowel movements a day may mean the baby is not getting enough milk. Babies who are hungry and feed every hour or two but who do not gain weight appropriately for their age and size are probably not getting enough milk. Babies who do not get enough milk may become dehydrated and develop hyperbilirubinemia. Babies who are small or premature or who have a mother who is ill or had a delivery that was difficult or required surgery are at risk of underfeeding.

Complications of Breastfeeding for the Mother
(See also Overview of the Postdelivery (Postpartum) Period.)
Common complications caused by breastfeeding include breast engorgement, sore nipples, plugged milk ducts, mastitis, and anxiety.
Breast engorgement is painful overfilling of the breasts with milk. Engorgement occurs during the early stages of milk production (lactation). For ways to relieve symptoms, see Breast engorgement.
For sore nipples, the infant's position during breastfeeding should be checked. Sometimes the infant draws in a lip and sucks it, which irritates the nipple. For ways to prevent and relieve sore nipples, see Breastfeeding.
Plugged milk ducts occur when the breasts do not get completely drained of milk on a regular basis. They cause mildly tender lumps that can be felt in the breasts of lactating women. Continued breastfeeding is the best way to unplug the duct. Although it may be painful to nurse on the affected side, frequent breastfeeding is necessary to completely empty the breast. Warm compresses and massage of the affected area before breastfeeding may help. Women may also vary their breastfeeding positions because different areas of the breast empty better depending on the infant's position at the breast. A good nursing bra is helpful because regular bras with underwires or constricting straps can compress milk ducts.
Mastitis is a breast infection that can occur in women who are breastfeeding, particularly if there is engorgement or a plugged milk duct. Bacteria can enter the breast through cracked or damaged nipples and cause an infection. The infected area is tender, warm, and red, and the woman may have fever, chills, and flu-like aching. Women whose symptoms are severe or do not go away in 12 to 24 hours are given antibiotics that are safe for breastfeeding infants. If pain is significant, women may take acetaminophen for relief. Women should continue breastfeeding during treatment.is a breast infection that can occur in women who are breastfeeding, particularly if there is engorgement or a plugged milk duct. Bacteria can enter the breast through cracked or damaged nipples and cause an infection. The infected area is tender, warm, and red, and the woman may have fever, chills, and flu-like aching. Women whose symptoms are severe or do not go away in 12 to 24 hours are given antibiotics that are safe for breastfeeding infants. If pain is significant, women may take acetaminophen for relief. Women should continue breastfeeding during treatment.
Anxiety, frustration, and feelings of inadequacy may result from a mother's lack of experience with breastfeeding, difficulties holding the infant and getting the infant to latch on and suck, fatigue, difficulty telling whether the infant is getting enough milk, and other physical changes that occur after giving birth. These factors and emotions are the most common reasons mothers stop breastfeeding. Mothers can consult with their pediatrician or a lactation specialist to discuss their feelings and possibly prevent stopping breastfeeding early.
Taking Medications While Breastfeeding
Mothers who are breastfeeding should avoid taking medications if possible. When medications are necessary, mothers should avoid certain ones and take only those that are known to be safe (see Medication Use During Pregnancy).
Weaning
When to stop breastfeeding (wean the infant) depends on the needs and desires of both mother and baby, but preferably not until the infant is at least 12 months old. Gradual weaning over weeks or months during the time solid food is introduced is most common. Some mothers and infants stop abruptly without problems, but others continue breastfeeding 1 or 2 times a day for 18 to 24 months or longer. There is no correct or easier schedule.
Mothers initially replace one to three breastfeeding sessions a day with a bottle or cup of water or diluted fruit juice (water or fruit juice should not be used when weaning infants younger than 6 months old), expressed breast milk, formula, or whole milk if the baby is older than 12 months. Learning to drink from a cup is an important developmental milestone, and weaning to a cup can be completed by age 10 months. Babies who are weaned to a sippy cup instead of a bottle do not go through a second weaning process from bottle to cup.
Some feedings, particularly those at mealtimes, should be replaced with solid food. Mothers gradually replace more and more breastfeedings, although many infants continue one or two breastfeedings daily until the age of 18 to 24 months or longer. When breastfeeding continues longer, the child should also be eating solid foods and drinking from a cup.







