



Allergic reactions (hypersensitivity reactions) are inappropriate responses of the immune system to a normally harmless substance.

 Filter")




Usually, allergies cause sneezing, watery and itchy eyes, a runny nose, itchy skin, and rash.
Some allergic reactions, called anaphylactic reactions, are life threatening.
Symptoms suggest the diagnosis, and skin testing can help identify the substance that triggers the allergy but does not predict the severity of a future reaction.
Avoiding the trigger is best, but if it is impossible, allergy shots, when given long before the exposure occurs, can sometimes desensitize the person.
People who have had or are at risk of having severe allergic reactions should always carry a self-injecting syringe of epinephrine and antihistamine pills.People who have had or are at risk of having severe allergic reactions should always carry a self-injecting syringe of epinephrine and antihistamine pills.
Severe reactions require emergency treatment in an emergency care facility.
Normally, the immune system—which includes antibodies, white blood cells, mast cells, complement proteins, and other substances—defends the body against foreign substances (called antigens). However, in susceptible people, the immune system can overreact when exposed to certain substances (allergens) in the environment, foods, or medications, which are harmless in most people. The result is an allergic reaction. (Allergens are molecules that the immune system can identify and that can stimulate a response by the immune system.) Some people are allergic to only one substance. Others are allergic to many.
Allergens may cause an allergic reaction when they land on the skin or in the eye or are inhaled, eaten, or injected. An allergic reaction can occur in several ways:
Triggered by substances present only during certain seasons, such as tree, grass, or ragweed pollens (seasonal allergy, including hay fever)
Triggered by taking a medication (drug allergy)
Triggered by eating certain foods (food allergy)
Triggered by breathing in dust, animal dander, or molds (year-round allergy)
Triggered by touching certain substances (such as latex)
Triggered by insect bites or stings (as occurs in anaphylactic reactions and angioedema)
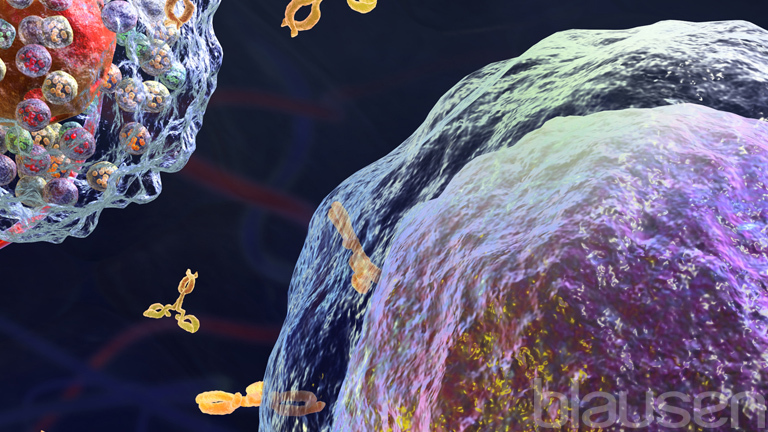
In many allergic reactions, the immune system, when first exposed to an allergen, produces a type of antibody called immunoglobulin E (IgE). IgE binds to a type of white blood cell called basophils in the bloodstream and to a similar type of cell called mast cells in the tissues. The first exposure may make people sensitive to the allergen (called sensitization) but does not cause symptoms. When sensitized people subsequently encounter the allergen, the basophils and mast cells with IgE on their surface release substances (such as histamine, prostaglandins, and leukotrienes) that cause swelling or inflammation in the surrounding tissues. Such substances begin a cascade of reactions that continue to irritate and harm tissues. These reactions range from mild to severe.
Some people have an inherited tendency to produce a lot of IgE (a condition called atopy) and may overreact to some antigens that cause hay fever, asthma, skin problems, or a food allergy.
Latex Allergy
Latex is a fluid that comes from the rubber tree. It is used to make rubber products, including some rubber gloves, condoms, and medical equipment such as catheters, breathing tubes, enema tips, and dental dams. Latex can cause the immune system to produce antibodies to IgE, which can lead to allergic reactions, including hives, rashes, and even severe and potentially life-threatening allergic reactions called anaphylactic reactions. However, the dry, irritated skin that many people develop after wearing latex gloves is usually the result of irritation and not an allergic reaction to latex. People may be at risk of becoming sensitive to latex if they
For unknown reasons, people who are allergic to latex are often allergic to bananas and sometimes other foods such as kiwi, papaya, avocados, chestnuts, potatoes, tomatoes, and apricots. Doctors may suspect latex allergy based on symptoms and the person's description of when symptoms occur, especially if the person is a health care professional. Blood or skin tests are sometimes done to confirm the diagnosis. People who are allergic to latex should avoid it. For example, health care professionals can use gloves and other products that are latex-free. Most health care institutions provide them. |

Causes of Allergic Reactions
Genetic and environmental factors work together to contribute to the development of allergies.
Genes are thought to be involved because specific mutations are common among people with allergies and because allergies tend to run in families.
Environmental factors also increase the risk of developing allergies. These factors include the following:
Repeated exposure to foreign substances (allergens)
Diet
Pollutants (such as tobacco smoke and exhaust fumes)
On the other hand, exposure to various antigens, such as bacteria and viruses and foods (including peanuts), during childhood may strengthen the immune system. Such exposure may help the immune system learn how to respond to allergens in a way that is not harmful and thus help prevent allergies from developing. An environment that limits a child's exposure to bacteria and viruses—commonly thought of as a good thing—may make allergies more likely to develop. Exposure to microorganisms is limited in families with fewer children and cleaner indoor environments and by the early use of antibiotics.
Microorganisms live in the digestive tract, in the respiratory tract, and on the skin, but which microorganisms are present varies from person to person. Which ones are present appears to affect whether and which allergies develop.
Allergens that most commonly trigger allergic reactions include
House dust mite droppings
Animal dander
Pollens (of trees, grasses, and weeds)
Molds
Insect venom
Household chemicals, such as cleaning products and fragrances
House dust mites live in the dust that builds up in carpets, bedding, soft furnishings, and soft toys.
Symptoms of Allergic Reactions
Most allergic reactions are mild, consisting of watery and itchy eyes, a runny nose, itchy skin, and some sneezing. Rashes (including hives) are common and often itch.
Hives, also called urticaria, are small, red, slightly elevated areas of swelling (wheals) that often have a pale center. Swelling may occur in larger areas under the skin (called angioedema). Swelling is caused by fluids leaking from blood vessels. Depending on which areas of the body are affected, angioedema may be serious, particularly when it occurs in the throat or airways.
Allergies may trigger attacks of asthma.
Certain allergic reactions, called anaphylactic reactions, can be life threatening. The airways can narrow (constrict), causing wheezing, and the lining of the throat and airways may swell, interfering with breathing. Blood vessels can widen (dilate), causing a dangerous fall in blood pressure.


Photo provided by Thomas Habif, MD.
Diagnosis of Allergic Reactions
A doctor's evaluation
Sometimes blood tests
Often skin tests and the allergen-specific serum IgE test
Doctors first determine whether a reaction is allergic. They may ask
Whether the person has close relatives with allergies because a reaction is more likely to be allergic in such cases
How often reactions occur and how long they last
How old the person was when the reactions started
Whether anything (such as exercise or exposure to pollen, animals, or dust) triggers the reaction
Whether any treatments have been tried and, if so, how the person responded
To help determine whether a reaction is allergic, doctors sometimes do blood tests to detect a type of white blood cell called eosinophils. Eosinophils, although present in everyone, are usually produced in greater numbers when an allergic reaction occurs. However, the usefulness of this test is limited because other eosinophilic disorders can cause the number of eosinophils to increase, and a normal number does not exclude the presence of an allergy.
If it seems likely that a person's symptoms are caused by an allergy, the main goal is to identify the specific allergen. Often, the person and doctor can identify the allergen, or at least the type of allergen, based on when the allergy started and when and how often the reaction occurs (for example, during certain seasons or after eating certain foods).
Skin tests and a blood test called the allergen-specific serum IgE test can also help doctors detect the specific allergen. However, these tests may not detect all allergies, and they sometimes indicate that people are allergic to an allergen when they are not (called a false-positive result).
Skin testing
Skin tests are the most useful way to identify specific allergens. An allergen applied to or injected into the skin should cause a skin reaction in people who are allergic to it. There are 2 types of skin tests:
Skin prick test
Intradermal test
To help ensure that the results of these skin test are reliable, doctors give 2 control solutions in addition to the test solution (which contains the suspected allergen). The control substances are
A drop of a histamine solution, which should trigger an allergic reaction in anyone, is given. If there is no skin reaction, it may be because the immune system is not working normally or because people have allergy medications in their system. People who do not react to histamine probably will not react to the test solution that contains the allergen. Thus, people may appear to have no allergy to the allergen when they do (a false-negative result).
A drop of diluting solution that contains no allergens and thus should not trigger an allergic reaction is given. If people react to the diluting solution, they probably have sensitive skin, and probably will also react to the test solution that contains the allergen, even if they are not allergic to it (a false-positive result).
Usually, doctors give several test solutions. These are dilute solutions, each with one specific antigen. Commonly used antigens include pollens (of trees, grasses, or weeds), molds, dust mites, animal dander, insect venom, foods, and some antibiotics. Doctors choose the antigens for this test based on which substances they suspect to be the cause.
Usually, a skin prick test is done first. A drop of each of the control and test solutions is placed on the person’s skin, which is then pricked with a needle through the drop. The skin prick test can identify most allergens.
If no allergen is identified, an intradermal test may be done. For this test, a tiny amount of each of the control and test solutions is injected into the person’s skin through a needle. This type of skin test is more sensitive and more likely to detect a reaction to an allergen.
If the person is allergic to one or more of the allergens in the test solution, the person has a wheal and flare reaction, indicated by the following:
A slightly elevated swelling that is pale or matches the person's skin tone—the wheal—appears at the pinprick site within 15 to 20 minutes.
The resulting wheal is about 1/8 to 2/10 inch (about 0.3 to 0.5 centimeters) larger in diameter than the wheal caused by the diluting solution.
The wheal is surrounded by a well-defined red area (which may be hard to identify on dark skin)—the flare.
Before skin tests are done, people are asked to stop taking medications that may suppress a reaction in a person who actually has an allergy to allergens in the test solution. These medications include
Antihistamines
Certain antidepressants called tricyclic antidepressants (such as amitriptyline)Certain antidepressants called tricyclic antidepressants (such as amitriptyline)
Omalizumab (a monoclonal antibody manufactured to block IgE)Omalizumab (a monoclonal antibody manufactured to block IgE)
Monoamine oxidase inhibitors (such as selegiline)Monoamine oxidase inhibitors (such as selegiline)
Some doctors also do not test people who are taking beta-blockers because if such people have an allergic reaction in response to the test, the consequences are more likely to be serious. In addition, beta-blockers may interfere with the medications used to treat serious allergic reactions.
Allergen-specific serum IgE tests

The allergen-specific serum IgE test, a blood test, is used when skin tests cannot be used—for example, when a rash is widespread. This test determines whether IgE in the person's blood binds to the specific allergen used for the test. If binding occurs, the person has an allergy to that allergen.
Provocative testing
For provocative testing people are directly exposed to a small amount of the suspected allergen. This test is usually done when people must document their allergic reaction—for example, for a disability claim. It is sometimes used to diagnose a food allergy. If doctors suspect an exercise-induced allergy, they may ask the person to exercise. If doctors suspect an allergy triggered by cold, they may place an ice cube on the person's skin to see if a rash develops.
Prevention of Allergic Reactions
Environmental measures
Avoiding or removing an allergen, if possible, is the best approach. Avoiding an allergen may involve the following:
Avoid certain medications (discuss with your doctor before stopping a medication)
Keeping pets out of the house or limiting them to certain rooms
Using high-efficiency particulate air (HEPA) vacuums and filters
Not eating a particular food
For people with severe seasonal allergies, possibly moving to an area that does not have the allergen
Removing or replacing items that collect dust, such as upholstered furniture, carpets, and knickknacks
Covering mattresses and pillows with finely woven fabrics that cannot be penetrated by dust mites and allergen particles
Using synthetic-fiber pillows and impermeable mattress covers
Frequently washing bed sheets, pillowcases, and blankets in hot water
Frequently cleaning the house, including dusting, vacuuming, and wet-mopping
Using air conditioners and dehumidifiers in basements and other damp rooms
Exterminating cockroaches

People with allergies should avoid or minimize exposure to certain other irritants that can make allergic symptoms worse or cause breathing problems. These irritants include the following:
Cigarette smoke
Strong odors
Irritating fumes
Air pollution
Cold temperatures
High humidity
Allergen immunotherapy (desensitization)
Allergen immunotherapy, usually allergy shots (injections), can be given to desensitize people to the allergen when some allergens, especially airborne allergens, cannot be avoided and the drugs used to treat allergic reactions are ineffective.
With allergen immunotherapy, allergic reactions can be prevented or reduced in number and/or severity. However, allergen immunotherapy is not always effective. Some people and some allergies tend to respond better than others.
Immunotherapy is used most often for allergies to
Pollens
House dust mites
Molds
Venom of stinging insects
When people are allergic to unavoidable allergens, such as insect venom, immunotherapy helps prevent anaphylactic reactions. Sometimes it is used for allergies to animal dander, but such treatment is unlikely to be useful. Immunotherapy for peanut allergy is available, and immunotherapy for other food allergies is being studied.
Immunotherapy is not used when the allergen, such as penicillin and other medications, can be avoided. However, if people need to take a medication that they are allergic to, immunotherapy, closely monitored by a doctor, can be done to desensitize them.
In immunotherapy, tiny amounts of the allergen are either injected under the skin or given by mouth, depending on the specific allergen. The first dose is so small that even an allergic person does not react to it. However, the small dose starts to get the person's immune system used to the allergen. Then the dose is gradually increased. Each increase is so small that the immune system still does not react. The dose is increased until the person is not reacting to the same amount of allergen that once caused symptoms. This dose is the person's maintenance dose. A gradual increase is necessary because exposure to too much allergen too soon can cause an allergic reaction. Injections are usually given once or twice a week until the maintenance dose is reached. Then injections are usually given every 2 to 4 weeks. The procedure is most effective when maintenance injections are continued throughout the year, even for seasonal allergies.
Because immunotherapy injections occasionally cause dangerous allergic reactions, people remain in the doctor’s office for at least 30 minutes afterward. If they have mild reactions to the immunotherapy (such as sneezing, coughing, flushing, tingling sensations, itching, chest tightness, wheezing, and hives), a medication—usually an antihistamine, such as diphenhydramine or loratadine—may help. For more severe reactions, epinephrine (adrenaline) is injected.Because immunotherapy injections occasionally cause dangerous allergic reactions, people remain in the doctor’s office for at least 30 minutes afterward. If they have mild reactions to the immunotherapy (such as sneezing, coughing, flushing, tingling sensations, itching, chest tightness, wheezing, and hives), a medication—usually an antihistamine, such as diphenhydramine or loratadine—may help. For more severe reactions, epinephrine (adrenaline) is injected.
Alternatively, doses of the allergen may be placed under the tongue (sublingual) and held there for a few minutes, then swallowed. The dose may be gradually increased, as for injections. The sublingual dose may be given every day or up to 3 times a week. Extracts for grass pollen, ragweed, or house dust mite, placed under the tongue, can be used to help prevent hay fever (allergic rhinitis).
Immunotherapy for peanut allergy may also be given by mouth (see Food Allergy, Prevention). The person receives the first several doses of the allergen over the course of a single day while in a doctor's office or clinic. The person then takes the allergen at home. Each time the dose is increased, the first dose of the higher dosage is given under a doctor's supervision.
Allergen immunotherapy may take 3 years to complete. People who develop allergies again may need another longer course (sometimes 5 years or more) of immunotherapy.
Treatment of Allergic Reactions
Avoidance of the allergen
Antihistamines
Mast cell stabilizers
Corticosteroids
For severe allergic reactions, emergency treatment, including epinephrine injectionsFor severe allergic reactions, emergency treatment, including epinephrine injections
Avoiding the allergen is the best way to treat as well as prevent allergies.
If mild symptoms occur, antihistamines are often all that is needed. If they are ineffective, other medications, such as mast cell stabilizers and corticosteroids, may help. Nonsteroidal anti-inflammatory drugs (NSAIDs) are not useful, except in eye drops used to treat allergic conjunctivitis.
Severe symptoms, such as those involving the airways (including anaphylactic reactions), require emergency treatment, including epinephrine injections.), require emergency treatment, including epinephrine injections.
Antihistamines
The medications most commonly used to relieve the symptoms of allergies are antihistamines. Antihistamines block the effects of histamine (which triggers symptoms). They do not stop the body from producing histamine.
Taking antihistamines partially relieves the runny nose, watery eyes, and itching and reduces the swelling due to hives or mild angioedema. But antihistamines do not ease breathing when airways are constricted. Some antihistamines (such as azelastine) are also Taking antihistamines partially relieves the runny nose, watery eyes, and itching and reduces the swelling due to hives or mild angioedema. But antihistamines do not ease breathing when airways are constricted. Some antihistamines (such as azelastine) are alsomast cell stabilizers.
Antihistamines are available as
Tablets, capsules, or liquid solutions to be taken by mouth
Nasal sprays
Eye drops
Lotions or creams
Which antihistamine is used depends on the type of allergic reaction. Some antihistamines are available without a prescription (over-the-counter, or OTC), and some require a prescription.
Products that contain an antihistamine and a decongestant (such as pseudoephedrine) are also available OTC and are useful when both an antihistamine and a nasal decongestant are needed. They can be taken by adults and children aged 12 years and older. Antihistamine-decongestant products should not be given to children under 12 years old. In addition, some people, such as those who are taking monoamine oxidase inhibitors (a type of antidepressant), cannot take these products. People with high blood pressure should not take a decongestant unless a doctor recommends it and monitors its use.Products that contain an antihistamine and a decongestant (such as pseudoephedrine) are also available OTC and are useful when both an antihistamine and a nasal decongestant are needed. They can be taken by adults and children aged 12 years and older. Antihistamine-decongestant products should not be given to children under 12 years old. In addition, some people, such as those who are taking monoamine oxidase inhibitors (a type of antidepressant), cannot take these products. People with high blood pressure should not take a decongestant unless a doctor recommends it and monitors its use.
The antihistamines diphenhydramine and doxepin, available in lotion, cream, gel, and spray forms, can be applied to the skin to relieve itching. People, particularly children, should not take antihistamines by mouth while using antihistamines applied to the skin because these medications can cause extreme drowsiness.The antihistamines diphenhydramine and doxepin, available in lotion, cream, gel, and spray forms, can be applied to the skin to relieve itching. People, particularly children, should not take antihistamines by mouth while using antihistamines applied to the skin because these medications can cause extreme drowsiness.
Side effects of antihistamines include anticholinergic effects, such as drowsiness, dry mouth, blurred vision, constipation, difficulty with urination, confusion, and light-headedness (particularly after a person stands up), as well as drowsiness.
Some antihistamines are more likely to cause drowsiness (sedation) than others. People should not take these antihistamines if they are going to drive, operate heavy equipment, or do other activities that require alertness. Antihistamines that cause drowsiness should not be given to children under 2 years old because they may have serious or life-threatening side effects. These antihistamines are also a particular problem for older adults and for people with glaucoma, benign prostatic hyperplasia, constipation, or dementia because of the medications’ anticholinergic effects. People with cardiovascular disease should consult their doctor before taking antihistamines, even OTC ones.
Not everyone reacts the same way to antihistamines. For example, people of Asian descent seem to be less susceptible to the sedative effects of diphenhydramine than are people of Western European origin. Also, antihistamines cause the opposite (paradoxical) reaction in some people, making them feel nervous, restless, and agitated.Not everyone reacts the same way to antihistamines. For example, people of Asian descent seem to be less susceptible to the sedative effects of diphenhydramine than are people of Western European origin. Also, antihistamines cause the opposite (paradoxical) reaction in some people, making them feel nervous, restless, and agitated.
Some Antihistamines
Medication | Degree of Anticholinergic Effects* | Degree of Drowsiness† |
|---|---|---|
Nonprescription (over-the-counter) | ||
BrompheniramineBrompheniramine | Moderate | Some |
CetirizineCetirizine | Few to none | Little to none in most people and moderate in some people |
ChlorpheniramineChlorpheniramine | Moderate | Some |
ClemastineClemastine | Strong | Moderate |
DesloratadineDesloratadine | Few to none | Little to none |
DiphenhydramineDiphenhydramine | Strong | Extreme |
FexofenadineFexofenadine | Few to none | Little to none |
LoratadineLoratadine | Few to none | Little to none |
Prescription | ||
Acrivastine‡ | Few to none | Little to none |
Azelastine§Azelastine§ | Few to none | Some |
CyproheptadineCyproheptadine | Moderate | Some |
DexchlorpheniramineDexchlorpheniramine | Moderate | Some |
HydroxyzineHydroxyzine | Moderate | Extreme |
LevocetirizineLevocetirizine | Few to none | Little to none |
Mizolastine | Few to none | Little to none |
PromethazinePromethazine | Strong | Extreme |
* Anticholinergic effects include dry mouth, blurred vision, constipation, difficulty with urination, confusion, and light-headedness (particularly after a person stands up). Older adults are particularly susceptible to these effects. | ||
† The degree of drowsiness varies, depending on the dose, other active ingredients in the formulation (as in formulations that contain a decongestant plus an antihistamine), and the person. | ||
‡ Acrivastine is available only in combination with pseudoephedrine (a decongestant). The combination is taken by mouth. Such combination medications are not used in children under 12 years old.‡ Acrivastine is available only in combination with pseudoephedrine (a decongestant). The combination is taken by mouth. Such combination medications are not used in children under 12 years old. | ||
§ Azelastine is also a mast cell stabilizer.§ Azelastine is also a mast cell stabilizer. | ||
Mast cell stabilizers
Mast cell stabilizers block mast cells from releasing histamines and other substances that cause swelling and inflammation.
Mast cell stabilizers are taken when antihistamines and other medications are not effective or have bothersome side effects. These medications may help control allergy symptoms.
These medications include azelastine, cromolyn, lodoxamide, ketotifen, nedocromil, olopatadine, and pemirolast. Azelastine, ketotifen, olopatadine, and pemirolast are also antihistamines.These medications include azelastine, cromolyn, lodoxamide, ketotifen, nedocromil, olopatadine, and pemirolast. Azelastine, ketotifen, olopatadine, and pemirolast are also antihistamines.
CromolynCromolyn is available by prescription as follows:
For use with an inhaler or nebulizer (which delivers the medication in aerosol form to the lungs)
As eye drops
As a liquid to be taken by mouth
Cromolyn is available without a prescription as a nasal spray to treat allergic rhinitis. Cromolyn usually affects only the areas where it is applied, such as the back of the throat, lungs, eyes, or nose. When taken by mouth, cromolyn can relieve the digestive symptoms of Cromolyn is available without a prescription as a nasal spray to treat allergic rhinitis. Cromolyn usually affects only the areas where it is applied, such as the back of the throat, lungs, eyes, or nose. When taken by mouth, cromolyn can relieve the digestive symptoms ofmastocytosis, but it is not readily absorbed into the bloodstream and thus has little effect on other bodywide allergic symptoms.
Corticosteroids
When antihistamines and mast cell stabilizers cannot control allergic symptoms, a corticosteroid may help.
Corticosteroids can be taken as a nasal spray to treat nasal symptoms or through an inhaler, usually to treat asthma.
Doctors prescribe a corticosteroid (such as prednisone) to be taken by mouth only when symptoms are very severe or widespread and all other treatments are ineffective. If taken by mouth at high doses and for a long time (for example, for more than 3 to 4 weeks), Doctors prescribe a corticosteroid (such as prednisone) to be taken by mouth only when symptoms are very severe or widespread and all other treatments are ineffective. If taken by mouth at high doses and for a long time (for example, for more than 3 to 4 weeks),corticosteroids can have many, sometimes serious side effects. Therefore, corticosteroids taken by mouth are used for as short a time as possible.
Creams and ointments that contain corticosteroids can help relieve the itching associated with allergic rashes. One corticosteroid, hydrocortisone, is available OTC.Creams and ointments that contain corticosteroids can help relieve the itching associated with allergic rashes. One corticosteroid, hydrocortisone, is available OTC.
Other medications
Leukotriene inhibitors, such as montelukast, are anti-inflammatory medications used to treat the following:such as montelukast, are anti-inflammatory medications used to treat the following:
Mild persistent asthma
Seasonal allergic rhinitis
They inhibit leukotrienes, which are released by some white blood cells and mast cells when they are exposed to an allergen. Leukotrienes contribute to inflammation and cause airways to constrict. Montelukast is used only when other treatments are ineffective.They inhibit leukotrienes, which are released by some white blood cells and mast cells when they are exposed to an allergen. Leukotrienes contribute to inflammation and cause airways to constrict. Montelukast is used only when other treatments are ineffective.
OmalizumabOmalizumab is a monoclonal antibody (which is a manufactured [synthetic] antibody designed to interact with a specific substance). Omalizumab binds to immunoglobulin E (IgE), an antibody that is produced in large amounts during an allergic reaction, and prevents IgE from binding to mast cells and basophils and triggering an allergic reaction. Omalizumab may be used to treat persistent or severe asthma when other treatments are ineffective. If hives recur frequently and other treatments are ineffective, it may be helpful. When it is used, the dose of a corticosteroid can be reduced. It is given by injection under the skin (subcutaneously).
Emergency treatment
Severe allergic reactions, such as an anaphylactic reaction, require prompt emergency treatment.
People who have had or are at risk of having severe allergic reactions should always carry a self-injecting syringe of epinephrine which should be used as quickly as possible if a severe reaction occurs. Antihistamine pills may also help, but People who have had or are at risk of having severe allergic reactions should always carry a self-injecting syringe of epinephrine which should be used as quickly as possible if a severe reaction occurs. Antihistamine pills may also help, butepinephrine should be injected before taking antihistamine pills. Usually, epinephrine stops the reaction, at least temporarily. Nonetheless, people who have had a severe allergic reaction should be transported to an emergency care facility. There, they can be closely monitored, and treatment can be repeated or adjusted as needed.
If an anaphylactic reaction occurs, the airways can become swollen and narrowed, making breathing difficult. The doctor may have to insert a tube through the nose or mouth into the windpipe (trachea) to help with breathing. Sometimes the trachea becomes too swollen and narrowed for the tube to pass through into the trachea. In such cases, the doctor may have to insert a tube directly into the trachea through an incision in the front of the neck (tracheostomy) to make breathing possible.
Treatment of allergies during pregnancy and breastfeeding
Whenever possible, pregnant women with allergies should control their symptoms by avoiding allergens. If symptoms are severe, pregnant women should use an antihistamine nasal spray. They should take antihistamines by mouth (oral antihistamines) only if antihistamine nasal sprays do not provide adequate relief.
Women who are breastfeeding should also try to avoid antihistamines. But if antihistamines are necessary, doctors prefer to use antihistamines that are less likely to cause drowsiness, and they prefer antihistamine nasal sprays to oral antihistamines. If oral antihistamines are essential for controlling symptoms, they should be taken immediately after feeding the baby.







