









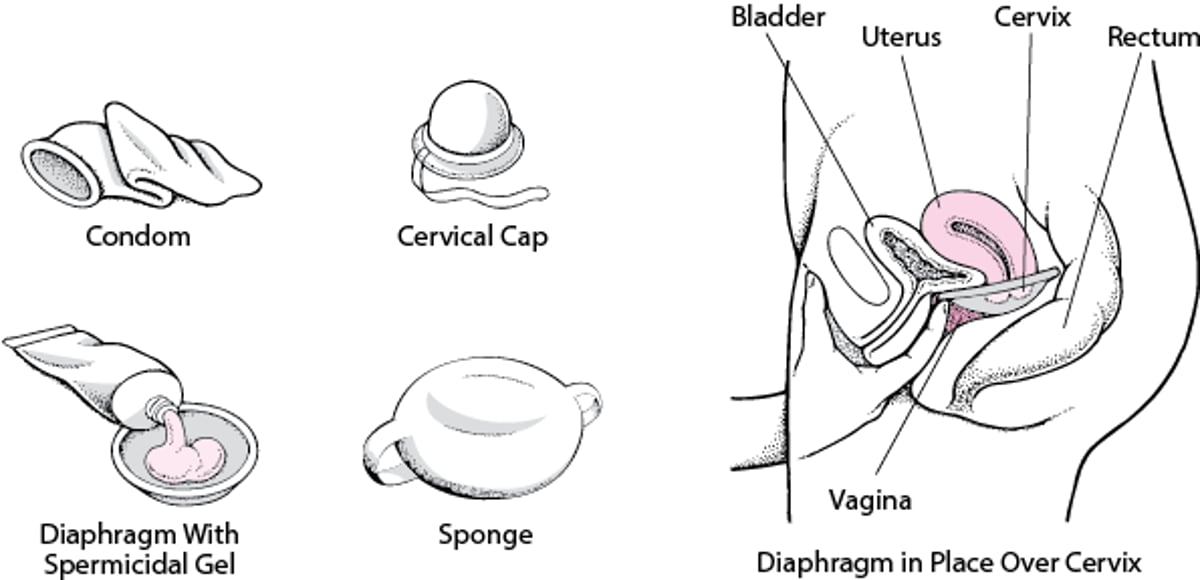
Barrier contraceptives physically block the sperm’s access to a woman’s uterus. They include condoms, diaphragms, cervical caps, contraceptive gels, contraceptive sponges, and spermicides (foams, creams, and suppositories). These contraceptives should be used by the woman or her partner each time they have sexual intercourse.
Blocking Access: Barrier Contraceptives
Barrier contraceptives prevent sperm from entering a woman’s uterus. They include the condom, diaphragm, cervical cap, and contraceptive sponge. Some condoms contain spermicides. Spermicides should be used with condoms and other barrier contraceptives that do not already contain them. |

Condoms
Condoms made of latex are the only contraceptives that provide protection against all common sexually transmitted infections (STIs), including those due to bacteria (such as gonorrhea and syphilis) and those due to viruses (such as HPV—human papillomavirus—and HIV—human immunodeficiency virus). Condoms made of a synthetic material such as polyurethane, polyisoprene, or silicon rubber provide some protection, but they are thinner and more likely to tear. Condoms made of lambskin do not protect against viral infections such as HIV infection.
A new condom should be used each time a person has sexual intercourse, and the condom should be discarded if its integrity is in doubt.
During the first year external (male) condoms are used, the chance of pregnancy is about 2% with perfect use (when instructions are followed exactly) and about 18% with typical use (the way most people use them). The chance of pregnancy with internal (female) condoms during the first year is 5% with perfect use and 21% with typical use.
A spermicide, which may be included in the condom’s lubricant or inserted separately into the vagina, may increase the effectiveness of condoms. Spermicide should be reapplied each time a condom is used.
Did You Know...
|
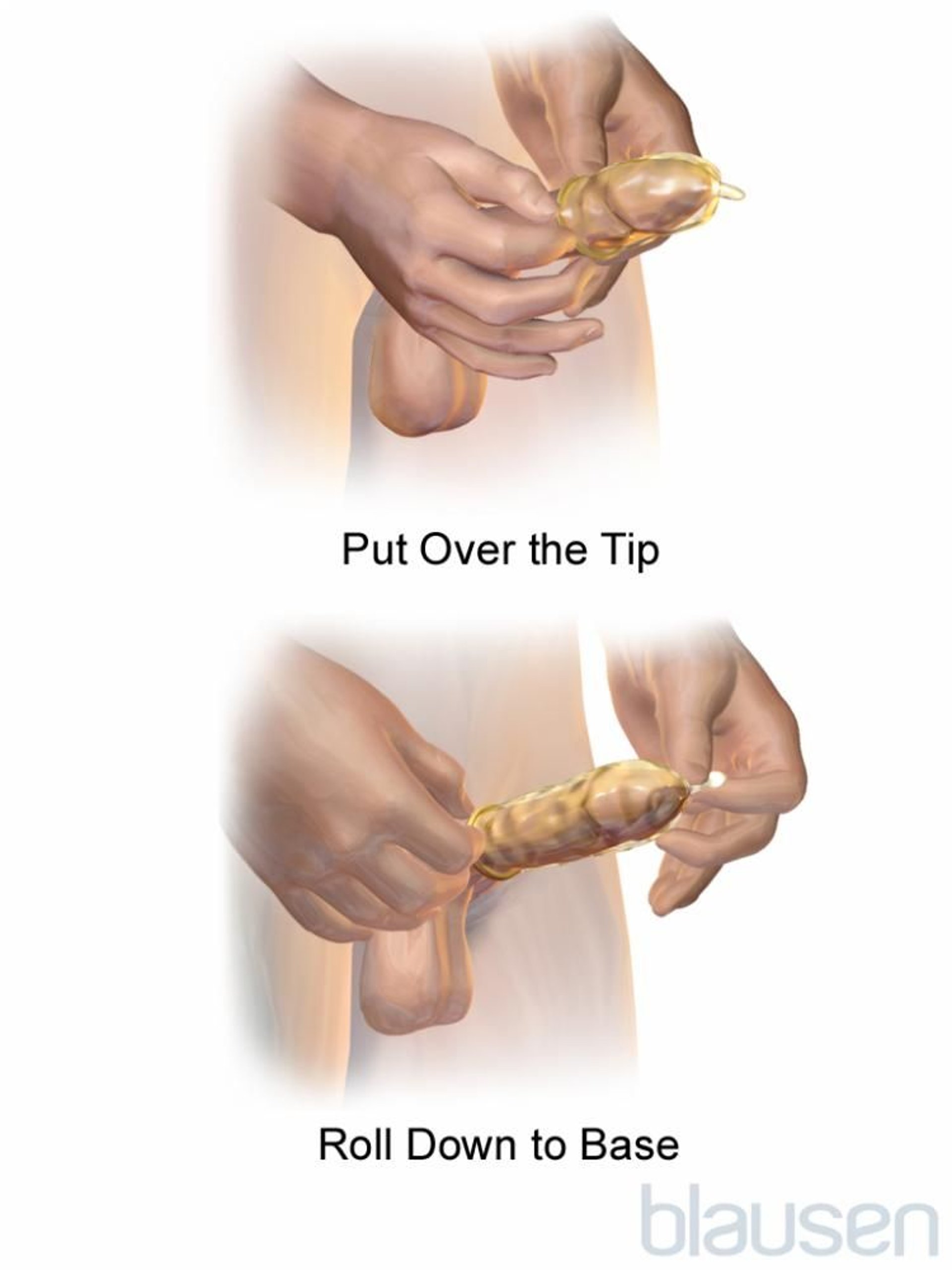
External (male) condoms are thin protective sheaths that cover the penis.
Condoms must be used correctly to be effective. Condoms should be applied before penetration. Correct use of an external (placed over the penis) involves the following:
Use a new condom for each episode of sexual intercourse.
Use the correct size condom.
Carefully handle the condom to avoid damaging it with fingernails, teeth, or other sharp objects.
Put the condom on after the penis is erect and before any genital contact with the partner.
Determine which way the condom is rolled by placing it on the index finger and gently trying to unroll it, but only a little bit. If it resists, turn it over, and try the other way. Then reroll it.
Place the rolled condom over the tip of the erect penis.
Leave 1/2 inch at the tip of the condom to collect semen.
With one hand, squeeze trapped air out of the tip of the condom.
If uncircumcised, pull the foreskin back before unrolling the condom.
With the other hand, roll the condom over the penis to its base and smooth out any air bubbles.
Make sure that lubrication is adequate during intercourse.
With latex condoms, use only water-based lubricants. Oil-based lubricants (such as petroleum jelly, shortening, mineral oil, massage oils, body lotions, and cooking oil) can weaken latex and cause the condom to break.
Hold the condom firmly against the base of the penis during withdrawal to prevent the condom from spilling semen.
External condoms should be positioned so that the tip extends almost 1/2 inch (about 1 centimeter) beyond the penis to provide a space to collect semen. Some condoms have a reservoir at the tip for this purpose. Immediately after ejaculation, the penis should be withdrawn while the condom’s rim is held firmly against the base of the penis to prevent the condom from slipping off and spilling semen.

The internal (female) condom is a pouch with an inner and an outer ring. The inner ring is inserted as far as it can go into the vagina (or anus), and the outer ring remains outside. Then, the penis is carefully guided through the outer ring into the pouch. If the penis slips out of the pouch or the outer ring is pushed inside, the condom can be removed and reinserted without risking pregnancy as long as semen has not been released (ejaculated). After sexual intercourse and before the condom is removed, the outer ring should be squeezed together and twisted to prevent semen from being spilled. Then the condom should be removed from the vagina carefully. If semen is spilled, sperm could enter the vagina, resulting in pregnancy. The female condom should be inserted no more than 8 hours before sexual intercourse.


Diaphragm
The diaphragm, a dome-shaped rubber cup with a flexible rim, is inserted into the vagina and positioned over the cervix. A diaphragm prevents sperm from entering the uterus.
Some diaphragms come in various sizes and must be fitted by a health care professional, who also teaches the woman how to insert it. If a woman has gained or lost more than 10 pounds, has had a diaphragm for more than a year, or has had a baby or an abortion, she must be refitted for a diaphragm because the vagina’s size and shape may have changed.
A new type of diaphragm is considered to be one size fits most women. It is made of silicone. Older diaphragms are made of latex. The silicone diaphragm is softer and more durable than the older diaphragms.
A diaphragm should cover the entire cervix without causing discomfort. Neither the woman nor her partner should notice its presence. A spermicidal cream or gel (which kills sperm) should always be used with a diaphragm. The cream or gel is placed on the inside of the cup (nearest to the cervix) in case the diaphragm is displaced during intercourse.
The diaphragm is inserted up to 2 hours before intercourse and should remain in place for at least 6 and probably 8 hours but no more than 24 hours. If intercourse is repeated while the diaphragm is in place, additional spermicidal cream or gel should be inserted into the vagina to continue protection.
Diaphragms can be washed and reused. A woman should inspect the diaphragm regularly for tears.
During the first year of latex diaphragm use, the percentage of women who become pregnant is approximately 6% with perfect use and about 12% with typical use (the way most people use it).
Cervical Cap
The cervical cap, a hat-shaped silicone cup, is inserted into the vagina and positioned over the cervix. A cervical cap prevents sperm from entering the cervix. Cervical caps resemble diaphragms but are smaller and more rigid.
Only one cervical cap is available in the United States. It comes in three sizes. Health care professionals determine what size a woman needs based on whether she has been pregnant before and whether the baby was delivered vaginally or by cesarean. Health care professionals must write a prescription for the cervical cap, but it does not need to be fitted for the woman.
A spermicidal cream or gel should always be used with a cervical cap. The cap is inserted 15 minutes to 40 hours before sexual intercourse and left in place at least 6 hours after intercourse and not more than 48 hours. A strap is attached to the cervical cap for easy removal. The cervical cap can be washed and reused for 1 year.
During the first year, the percentage of women who become pregnant with typical use is about 8% in women who have not had a baby. However, women who have had children are more likely to become pregnant when using a cervical cap than women who have not had children. Childbirth changes the cervix, making a secure fit with a cap less likely.
Contraceptive Gel
Contraceptive gel changes the acidity (pH) of the vaginal pH. This change incapacitates sperm and thus prevents fertilization of the egg.
The percentage of women who become pregnant is 7% with perfect use and 14% with typical use. Because the effectiveness of contraceptive gel is limited, it is best used with another barrier contraceptive, such as a condom or diaphragm.
Vaginal gel should be placed in the vagina no more than 1 hour before sexual intercourse and reapplied before each time intercourse occurs.
Vaginal gel does not reliably protect against sexually transmitted infections.
Contraceptive Sponge
A contraceptive sponge is a round, pillow-shaped polyurethane sponge about 1 1/2 in (4 cm) in diameter. The sponge is wet with water, folded, and inserted deep into the vagina, where it blocks sperm from entering the uterus. The sponge also contains a spermicide. It is available over the counter and does not need to be fitted by a health care professional.
The sponge can be inserted into the vagina by the woman up to 24 hours before sexual intercourse and provides protection through that period of time, regardless of how frequently intercourse is repeated. The sponge must be left in place for at least 6 hours after the last episode of intercourse. It should not be left in place for more than 30 hours. Usually, neither partner is aware of its presence once it is inserted.
The sponge is less effective than the diaphragm. Pregnancy rates with typical use are 12% for women who have not had children and 24% for women who have.
Problems related to use are uncommon. They include allergic reactions, vaginal dryness or irritation, and difficulty removing the sponge.
Spermicides
Spermicides are preparations that kill sperm on contact. They are available as vaginal foams, creams, gels, and suppositories and are placed in the vagina before a couple has sexual intercourse. These contraceptives provide a chemical barrier to sperm by trapping and damaging sperm. Thus, they prevent sperm from fertilizing an egg.
Most types of spermicides are equally effective. If women who use spermicides as instructed (perfect use), about 19% of them become pregnant during the first year of use. With contraceptive gel, about 7% of women become pregnant if they use gels as instructed and about 14% become pregnant if they use it the way most people use it (typical use).
Because their effectiveness is limited, spermicides are best used with another barrier contraceptive, such as a condom or diaphragm.
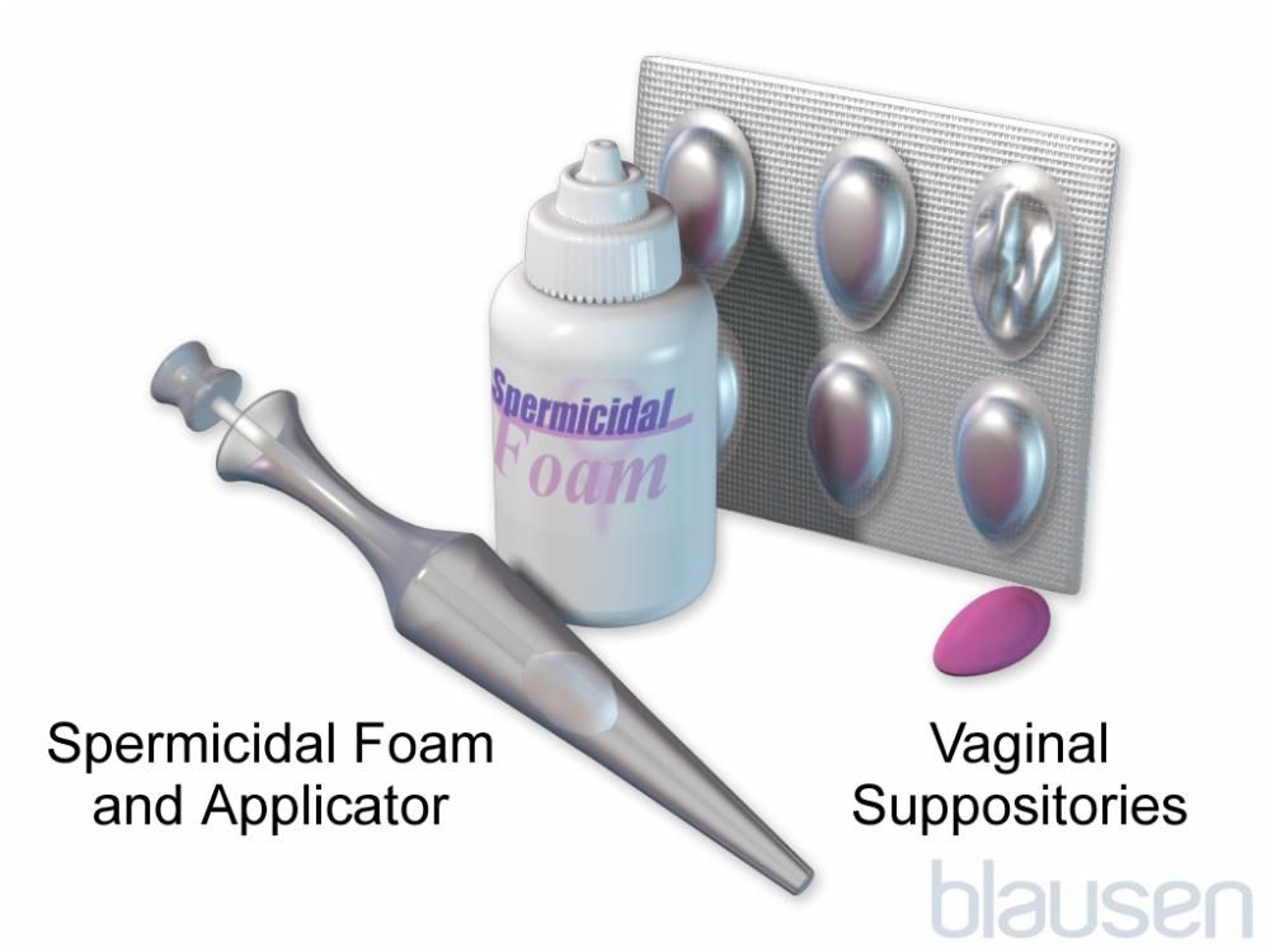
Spermicides should be placed in the vagina at least 10 to 30 minutes and usually no more than 1 hour before sexual intercourse. They should be reapplied each time a couple has intercourse.
Using spermicides several times a day may irritate the vagina and damage the tissues lining it. As a result, the microorganisms that cause sexually transmitted infections (including HIV) can more easily enter the body and cause disease. Spermicides do not protect against sexually transmitted infections.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
CDC: Condom Effectiveness: This web site provides information about the correct use of male and female condoms and dental dams, prevention of sexually transmitted infections with the male condom, and links to additional resources.





