





Permanent contraception involves making a person incapable of reproduction.
Topic Resources


Disrupting the tubes that carry sperm or the egg ends the ability to reproduce.
This form of contraception should always be considered permanent, although the procedures can sometimes be reversed.
Vasectomy is a short procedure for men, done in the doctor’s office.
The procedure for women (often called tubal sterilization) is more complicated and may be done using a thin tube inserted through a small incision in the abdomen or done through a larger incision in the abdomen.
In the United States, about one third of all married couples who use family planning methods, particularly if the woman is over 30, choose permanent contraception. For men, the procedure is vasectomy. For women, permanent contraception procedures can be done using a thin tube inserted through a small incision in the abdomen (laparoscopy) or through an incision in the abdomen (minilaparotomy—see below). Permanent contraception for women is often called tubal sterilization, which also refers to a specific procedure, the so-called tying the tubes.
Sterilization procedures are very effective. The percentages of women who become pregnant after 1 year are
For vasectomy: 0.15%
For procedures involving the fallopian tubes: 0.6%
One year after their partner has a vasectomy, fewer than 0.2% of women become pregnant. About 1.1% of women become pregnant during the 5 years after their partner has had a vasectomy.
This form of contraception should always be considered permanent. However, if couples change their minds, an operation that reconnects or opens the appropriate tubes (called reanastomosis) can be done to try to restore fertility. Its success depends in part on which procedure was used. Reanastomosis is less likely to be effective in men than in women. For couples, pregnancy rates are about 26% after reanastomosis in men.
For women, the likelihood of reversing a permanent contraception procedure depends on the following:
Which procedure was used
How old the woman is
How much of the tube remains
How much scarring has occurred
What fertility test results in the woman and her partner are
If reanastomosis is unsuccessful, conception may be possible with in vitro (test tube) fertilization.
Vasectomy
Vasectomy is used to provide permanent contraception for men. It involves cutting and sealing the vasa deferentia (the tubes that carry sperm from the testes). A vasectomy, which is done by a urologist in the office, takes about 20 minutes and requires only a local anesthetic. Through a small incision on each side of the scrotum, a section of each vas deferens is removed and the open ends of the tubes are sealed off.
After a vasectomy, backup method of contraception should be used until sterility is confirmed. Usually, men do not become sterile until they have had about 20 ejaculations after the operation because many sperm are stored in the seminal vesicles. Sterility is confirmed when a laboratory test shows that semen from two ejaculations, usually obtained 3 months after the procedure, is free of sperm.


Complications of vasectomy include
A blood clot in the scrotum (in 5% or fewer)
An inflammatory response to sperm leakage
Spontaneous reanastomosis (in fewer than 1%)
In spontaneous reanastomosis, the disrupted tubes become reconnected or unblocked on their own, thus restoring fertility. If reanastomosis occurs, it usually does so shortly after the procedure.
Sexual activity, with contraception until sterility is confirmed, may resume as soon after the procedure as men wish, but ejaculation should be avoided for the first few days because it can cause pain.
Did You Know...
|
Tubal Sterilization
Permanent contraception for women involves a surgical procedure to disrupt the fallopian tubes, which carry the egg from the ovaries to the uterus. Or the fallopian tubes may be completely removed.
If the fallopian tubes are completely removed, pregnancy is not possible. After procedures that do not involve removing the fallopian tubes, about 2% of women become pregnant during the first 10 years after a permanent contraception procedure is done. About one third of these pregnancies are mislocated (ectopic) pregnancies that develop in the fallopian tubes.
Permanent contraception may be planned in advance and done as elective surgery, or it can be done during cesarean delivery or 1 to 2 days after vaginal delivery.
Surgical removal of the uterus (hysterectomy) also results in sterility. This procedure is usually done to treat a disorder rather than as a contraception procedure.
Permanent contraception by laparoscopy
Laparoscopic tubal sterilization is commonly done. This procedure is done in an operating room. After women are given a general anesthetic, doctors make small incisions just below the navel. Doctors then insert a thin viewing tube (laparoscope) through an incision and work through the laparoscope to remove, disrupt, and/or seal off the fallopian tubes by doing one of the following:
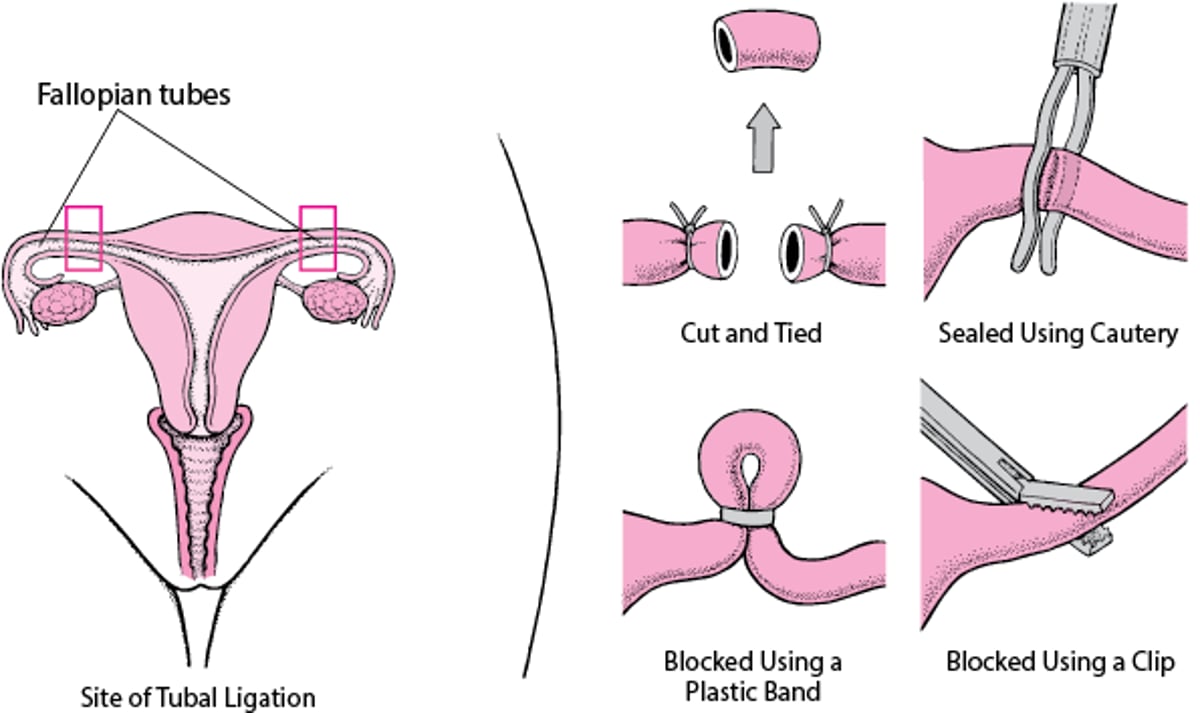
Using electrocautery (a device that produces an electrical current to cut through tissue) to completely remove the tubes or to seal off about 1 inch of each tube
Applying devices, such as plastic bands or metal clips, to block the tubes or pinch and hold them closed
After this procedure, the woman usually goes home the same day. Up to 6% of women have minor complications, such as a skin infection or pain at the incision site or constipation. Fewer than 1% have major complications, such as bleeding or punctures of the bladder or intestine.
Tubal Sterilization
Both fallopian tubes (which carry the egg from the ovaries to the uterus) are cut, sealed, or blocked so that sperm cannot reach the egg to fertilize it. |

Minilaparotomy
Minilaparotomy is sometimes used instead of tubal sterilization by laparoscopy, usually when women want to permanent contraception soon after they have had a baby.
A general, regional, or local anesthetic is used. Women do not have to stay in the hospital any longer than they would after having a baby. Doctors make a small incision (about 1 to 3 inches) in the abdomen. Then, they usually remove a section of each fallopian tube. Compared with laparoscopy, minilaparotomy causes more pain, and recovery takes a little longer.
Permanent contraception by hysteroscopy
As of December 31, 2018, the special device required for this procedure is no longer available in the United States.
For this procedure, no incisions are necessary. A local anesthetic is used, with or without medications to make the woman drowsy (sedatives).
Doctors insert a flexible viewing tube (hysteroscope) through the vagina and uterus and into the fallopian tubes. Coils (microinserts) are then inserted into the fallopian tubes to block them. The coil irritates tissue in the tubes, causing scar tissue to form. The scar tissue blocks the tubes. Scar tissue takes up to 3 months to form, so women must use another method of contraception until doctors confirm that the tubes are blocked. Women can usually go home the same day as the procedure.
About 3 months later, doctors confirm that the tubes are blocked by taking x-rays after a radiopaque dye is injected through the vagina into the uterus and fallopian tubes (called hysterosalpingography). If the dye does not come out the end of the fallopian tubes, doctors can confirm that the tubes are blocked.
Usually, this type of sterilization cannot be reversed.
Unintended pregnancy rates are similar whether hysteroscopy or laparoscopy is used for permanent contraception. However, after hysteroscopy, women are more likely to require a second operation.
Possible problems
Procedures that provide permanent contraception in women cause few problems. Problems include
Death: 1 to 2/100,000 women
Bleeding (hemorrhage) or an injury to the intestines: About 0.5% of women
Failure to block the tubes, pain, and other complications: Up to about 5% of women
A mislocated (ectopic) pregnancy: About 30% of pregnancies that occur after tubal sterilization
If women have ongoing pain or vaginal bleeding, the microinserts may have to be removed, Typically, the microinserts are removed by hysteroscopy, but laparoscopy may be required if part of the microinsert is outside the fallopian tube.







