



Oral inflammation and ulcers, known as stomatitis, may be mild and localized or severe and widespread. They are invariably painful.


")

")
")



(See also Evaluation of the Dental Patient and Gingivitis.)
Stomatitis may involve swelling and redness of the oral mucosa or discrete, painful ulcers (single or multiple). Less commonly, whitish lesions form. Rarely, the mouth appears normal despite significant symptoms (burning mouth syndrome). Symptoms hinder eating, sometimes leading to dehydration and undernutrition. Secondary infection occasionally occurs, especially in patients with immunocompromise. Some conditions are recurrent.
Etiology of Stomatitis
Stomatitis may be caused by local infection, systemic disease, a physical or chemical irritant, or an allergic reaction (see the table Some Causes of Stomatitis); many cases are idiopathic. Because the normal flow of saliva protects the mucosa against many insults, xerostomia predisposes the mouth to stomatitis of any cause.


CLINICA CLAROS/SCIENCE PHOTO LIBRARY

SCIENCE SOURCE/SCIENCE PHOTO LIBRARY


© Springer Science+Business Media


Image provided by Jonathan A. Ship, DMD.
The most common causes include
Recurrent aphthous stomatitis (RAS)—also called recurrent aphthous ulcers (RAU)
Viral infections, particularly herpes simplex and herpes zoster
Other infectious agents (Candida albicans and bacteria)
Trauma
Tobacco or irritating foods or chemicals
Chemotherapy and radiation therapy
Systemic disorders
Some Causes of Stomatitis
Category | Examples |
|---|---|
Bacterial infections | Actinomycosis* Acute necrotizing ulcerative gingivitis Syphilis, primary or secondary Tuberculosis* |
Fungal infections | Blastomycosis* Candidal infections (most common) Coccidioidomycosis* Cryptococcosis* Mucormycosis* (more common in people with diabetes) |
Viral infections | Herpes simplex infection, primary (mostly in young children) Herpes simplex infection, secondary (cold sores on the lips or palate) Varicella zoster, primary (chickenpox) Varicella zoster reactivation (shingles)* Others (eg, infection by coxsackievirus, cytomegalovirus, Epstein-Barr virus, or HIV; condyloma acuminata; influenza; rubeola) |
Systemic disorders | Cyclic neutropenia* Pemphigoid, pemphigus vulgaris Thrombotic thrombocytopenic purpura* Vitamin B deficiency (pellagra) Vitamin C deficiency (scurvy) |
Drugs | Antibiotics* Antiseizure medications* Barbiturates* Chemotherapeutic agents Gold* Iodides* Nonsteroidal anti-inflammatory drugs (NSAIDs)* |
Physical irritation | Dentures that fit poorly Broken or jagged teeth Habitual cheek or lip biting |
Irritants, and allergens | Acidic foods Nickel or palladium (in dental appliances) Dyes, acid fumes, heavy metals, or metal or mineral dusts (via occupational exposure) Tobacco (nicotinic stomatitis, particularly pipe smoker’s palate [hyperkeratotic palate with red dots at the openings of minor salivary glands]) Type IV hypersensitivity reaction (eg, to ingredients in toothpaste such as sodium lauryl sulfate, mouthwash, candy, gum, dyes, or lipstick) Aspirin, when applied topicallyAspirin, when applied topically |
Other | Recurrent aphthous stomatitis (most commonly, minor aphthae) Head and neck radiation |
* Rare. | |
Evaluation of Stomatitis
History
History of present illness should ascertain the duration of symptoms and whether the patient ever had them previously. Presence and severity of pain should be noted. The relation of symptoms to food, drugs, oral hygiene materials (eg, toothpaste, mouth rinses), and other substances (particularly occupational exposure to chemicals, metals, fumes, or dust) is sought.
Review of systems seeks symptoms of possible causes, including chronic diarrhea and weakness (inflammatory bowel disease, celiac disease); genital lesions (Behçet disease, syphilis); eye irritation (Behçet disease); and weight loss, malaise, and fever (nonspecific chronic illness).
Past medical history should ascertain known conditions that cause oral lesions, including herpes simplex, Behçet disease, inflammatory bowel disease, and risk factors for oral lesions, including immunocompromised state (eg, cancer, diabetes, organ transplant, use of immunosuppressants, HIV infection). Whether chemotherapy or radiation therapy has ever been used to manage cancer needs to be determined. Medication history should note all recent medications used. History of tobacco use should be noted. Social history should include sexual contact, particularly oral sex, unprotected sex, and sex with multiple partners.
Physical examination
Vital signs are reviewed for fever. The patient’s general appearance is noted for lethargy, discomfort, or other signs of significant systemic illness.
The mouth is inspected for the location and nature of any lesions.
The skin and other mucosal surfaces (including the genitals) are inspected for any lesions, rash, petechiae, or desquamation. Any bullous lesions may be tested for the Nikolsky sign (upper layers of epidermis move laterally with gentle lateral pressure or rubbing of skin adjacent to a blister).
Red flags
The following findings are of particular concern:
Fever
Cutaneous bullae
Ocular inflammation
Immunocompromise (Nikolsky sign)
Interpretation of findings
Occasionally, causes are obvious in the history (eg, cytotoxic chemotherapy; significant occupational exposure to chemicals, fumes, or dust). Recurrent episodes of oral lesions occur with recurrent aphthous stomatitis (RAS), herpes simplex, and Behçet disease. History of diabetes, HIV infection or other immunocompromise, or recent antibiotic use should increase suspicion of Candida infection. Recent medication use (particularly sulfa medications, other antibiotics, and antiseizure medications) should increase suspicion of Stevens-Johnson syndrome (SJS).
Some causes typically have extraoral, noncutaneous findings, some of which suggest a cause. Recurrent gastrointestinal symptoms suggest inflammatory bowel disease or celiac disease. Ocular symptoms can occur with Behçet disease and SJS. Genital lesions may occur with Behçet disease and primary syphilis.
Some causes usually also have extraoral, cutaneous findings.
Cutaneous bullae suggest SJS, pemphigus vulgaris, or bullous pemphigoid. Prodrome of malaise, fever, conjunctivitis, and generalized macular target lesions suggests SJS. Pemphigus vulgaris starts with oral lesions, then progresses to flaccid cutaneous bullae. Bullous pemphigoid has tense bullae on normal-appearing skin. The Nikolsky sign is usually positive in SJS and pemphigus vulgaris.
Cutaneous vesicles are typical with chickenpox or herpes zoster (see Herpesviruses). Unilateral lesions in a band along a dermatome suggest herpes zoster. Diffuse, scattered vesicular and pustular lesions in different stages suggest chickenpox.
Kawasaki disease usually has a macular rash, desquamation of hands and feet, and conjunctivitis, but lesions can be present at different times; it occurs in children, usually those < 5 years. Oral findings include erythema of the lips and oral mucosa.
Other cutaneous lesions may implicate erythema multiforme, hand-foot-and-mouth disease (resulting from coxsackievirus), or secondary syphilis.
Some causes have isolated oral findings, including RAS, most viral infections, acute necrotizing ulcerative gingivitis (ANUG), primary syphilis, gonorrhea, and Candida.


Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
Location of oral lesions may help identify the cause. Interdental ulcers occur with primary herpes simplex or acute necrotizing ulcerative gingivitis. Lesions on keratinized surfaces suggest herpes simplex or physical injury. Physical injury typically has an irregular appearance and occurs near projections of teeth, dental appliances, or where biting or an errant toothbrush can injure the mucosa. An aspirin burn next to a tooth and pizza burn on the palate are common.
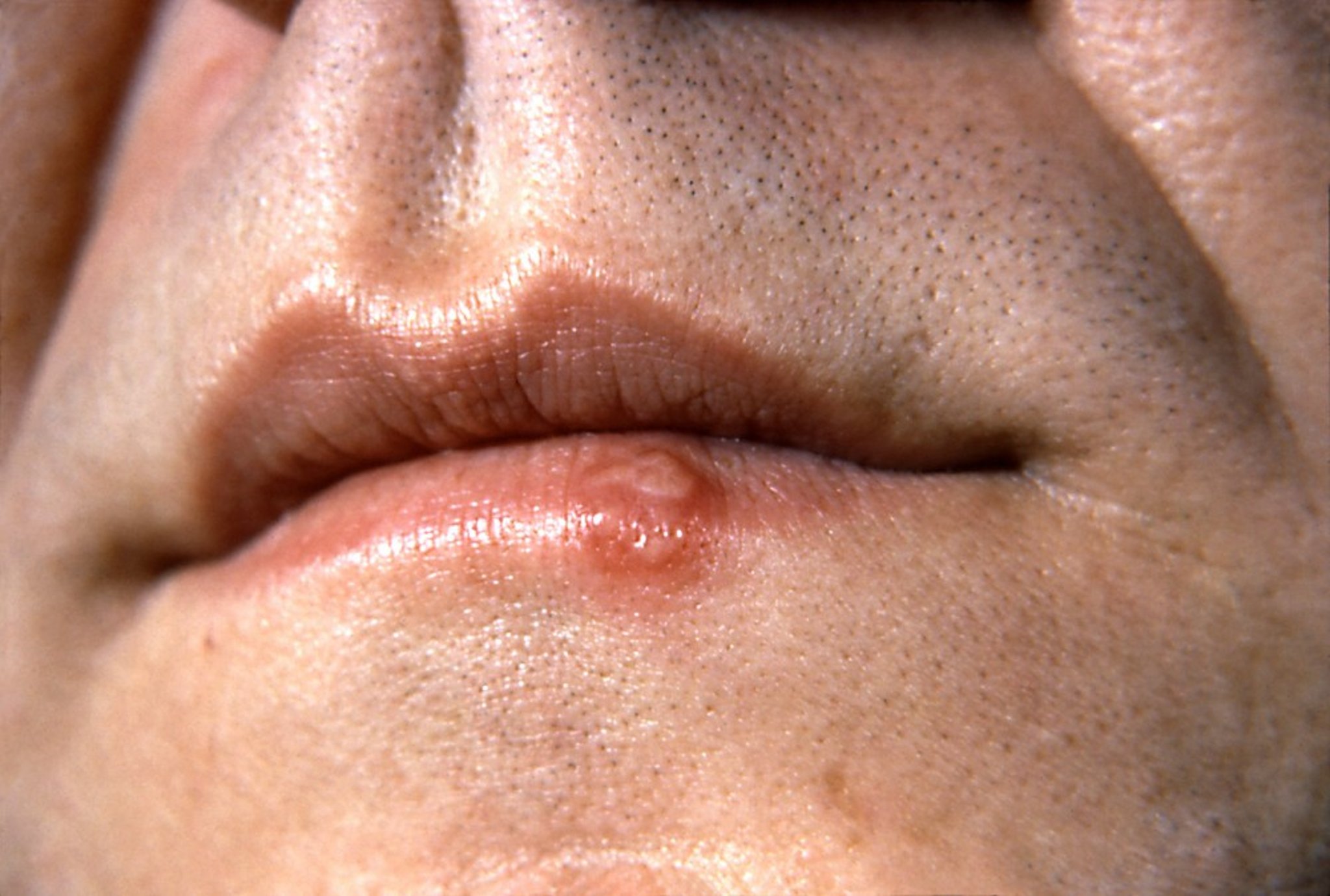
Primary herpes simplex infection causes multiple vesicular lesions on the intraoral mucosa on both keratinized and nonkeratinized surfaces and always includes the gingiva. These lesions rapidly ulcerate. Clinical manifestation occurs most often in children. Subsequent reactivations (secondary herpes simplex, cold sore) usually appear starting in puberty on the lip at the vermilion border and, rarely, on the hard palate.
Acute necrotizing ulcerative gingivitis causes severe inflammation and punched-out ulcers on the dental papillae and marginal gingivae. A severe variant called noma (gangrenous stomatitis) can cause full-thickness tissue destruction (sometimes involving the lips or cheek), typically in a patient with frailty or undernutrition. It begins as a gingival, buccal, or palatal (midline lethal granuloma) ulcer that becomes necrotic and spreads rapidly. Tissue sloughing may occur.


Isolated oral gonorrhea very rarely causes burning ulcers and erythema of the gingiva and tongue, as well as the more common pharyngitis. Primary syphilis chancres may appear in the mouth. Tertiary syphilis may cause oral gummas or a generalized glossitis and mucosal atrophy. A common sign of HIV becoming AIDS is hairy leukoplakia (vertical white lines on the lateral border of the tongue).

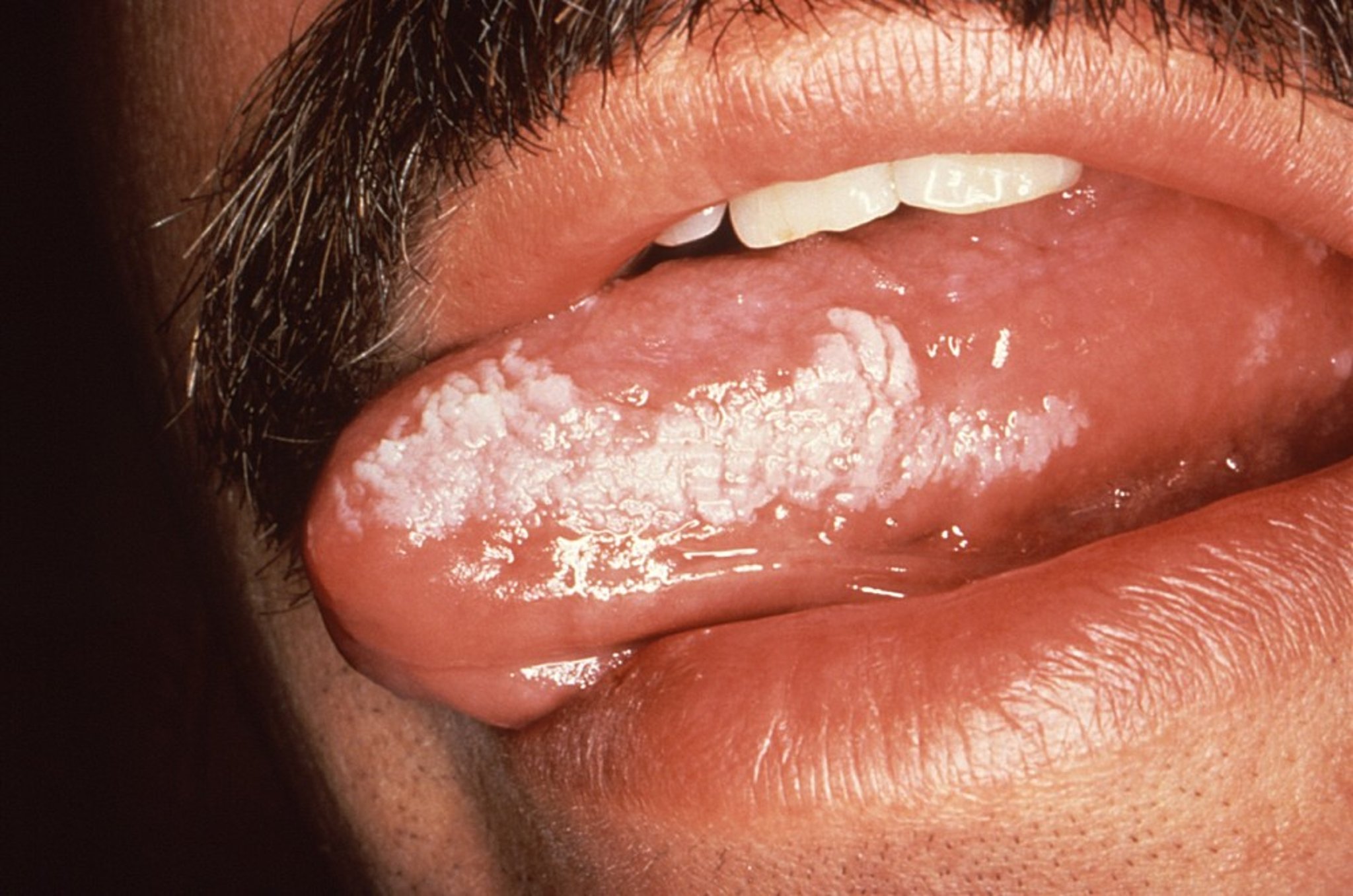
Image courtesy of J.S. Greenspan, BDS, University of California, San Francisco and Sol Silverman, Jr., DDS via the Public Health Image Library of the Centers for Disease Control and Prevention.
C. albicans and related species, which are normal oral flora, can overgrow in people who have taken antibiotics or corticosteroids or who have immunocompromise, such as patients with AIDS. C. albicans can cause whitish, cheesy plaques that leave erosions when wiped off. Sometimes only flat, erythematous areas appear (erosive form of Candida).
Testing
Bacterial and viral culture
Laboratory tests
Biopsy
Patients with acute stomatitis and no symptoms, signs, or risk factors for systemic illness probably require no testing.
If stomatitis is recurrent, viral and bacterial cultures, complete blood count, serum iron, ferritin, vitamin B12, folate, zinc, and endomysial antibody (for celiac disease) are done. Biopsy at the periphery of normal and abnormal tissue can be done for persistent lesions that do not have an obvious etiology.
Systematically eliminating foods from the diet can be useful, as can changing brands of toothpaste, chewing gum, or mouthwash.
Treatment of Stomatitis
Cause treated
Oral hygiene
Topical agents and rinses
Chemical or physical cautery
Specific disorders are treated, and any causative substances or medications are avoided. Mouth rinses that contain ethanol can cause or worsen stomatitis and should not be used.Specific disorders are treated, and any causative substances or medications are avoided. Mouth rinses that contain ethanol can cause or worsen stomatitis and should not be used.
Meticulous oral hygiene (using a soft toothbrush and salt-water rinses) may help prevent secondary infection. A soft diet that does not include acidic or salty foods is followed.
Topical measures
Numerous topical treatments, alone or in combination, are used to ease symptoms. These treatments include
Anesthetics
Protective coatings
Corticosteroids
Physical measures (eg, cautery)
To reduce discomfort that may interfere with eating and drinking, the following may be effective:
Lidocaine rinse Lidocaine rinse
Sucralfate plus aluminum-magnesium antacid rinseSucralfate plus aluminum-magnesium antacid rinse
A 2-minute rinse is done with 15 mL 2% viscous lidocaine every 3 hours as needed; patient expectorates when done (no rinsing with water and no swallowing unless the pharynx is involved). A soothing coating may be prepared with sucralfate (1-g pill dissolved in 15 mL water) plus 30 mL of aluminum-magnesium liquid antacid; the patient should rinse with or without swallowing. Many institutions and pharmacies have their own variation of this formulation (magic mouthwash), which sometimes also contains an antihistamine.A 2-minute rinse is done with 15 mL 2% viscous lidocaine every 3 hours as needed; patient expectorates when done (no rinsing with water and no swallowing unless the pharynx is involved). A soothing coating may be prepared with sucralfate (1-g pill dissolved in 15 mL water) plus 30 mL of aluminum-magnesium liquid antacid; the patient should rinse with or without swallowing. Many institutions and pharmacies have their own variation of this formulation (magic mouthwash), which sometimes also contains an antihistamine.
If the physician is certain the inflammation is not caused by an infectious organism, the patient can
Rinse and expectorate after meals with dexamethasone elixir 0.5 mg/5 mL (1 tsp)Rinse and expectorate after meals with dexamethasone elixir 0.5 mg/5 mL (1 tsp)
Apply a paste of 0.1% triamcinolone in an oral emollientApply a paste of 0.1% triamcinolone in an oral emollient
Wipe amlexanox over the ulcerated area with the tip of a finger
Chemical or physical cautery can ease the pain of localized lesions. Silver nitrate sticks are not as effective as low-power (2- to 3-watt), defocused, pulsed-mode carbon dioxide laser treatments, after which pain relief is immediate and lesions tend not to recur locally.Chemical or physical cautery can ease the pain of localized lesions. Silver nitrate sticks are not as effective as low-power (2- to 3-watt), defocused, pulsed-mode carbon dioxide laser treatments, after which pain relief is immediate and lesions tend not to recur locally.
Key Points
Isolated stomatitis in patients with no other symptoms and signs or risk factors for systemic illness is usually caused by a viral infection or recurrent aphthous stomatitis (RAS).
Extraoral symptoms, rash, or both suggest more immediate need for diagnosis.







