



")



(See also Overview of Inflammatory Bowel Disease.)
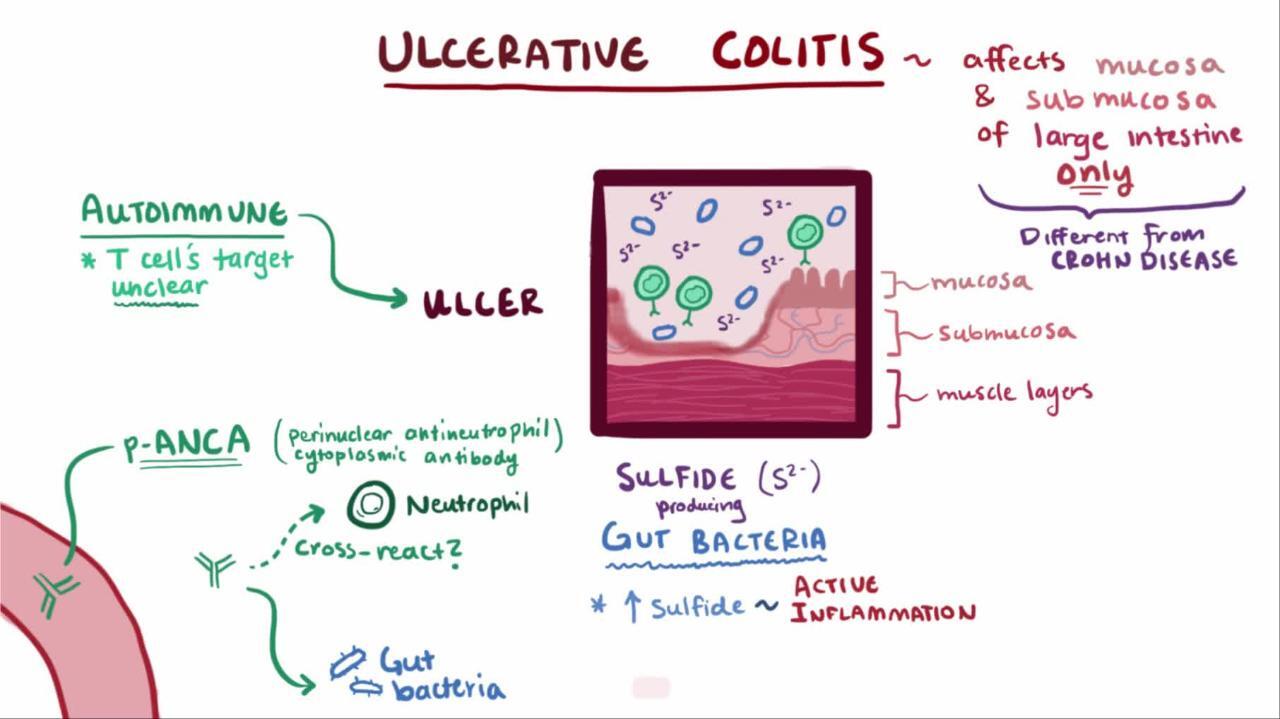
Pathophysiology of Ulcerative Colitis
Ulcerative colitis usually begins in the rectum. It may remain localized to the rectum (ulcerative proctitis) or extend proximally, sometimes involving the entire colon. Rarely, it involves most of the large bowel at once.
The inflammation caused by ulcerative colitis affects the mucosa and submucosa, and there is a sharp border between normal and affected tissue. Only in severe disease is the muscularis involved. Early in the disease, the mucous membrane is erythematous, finely granular, and friable, with loss of the normal vascular pattern and often with scattered hemorrhagic areas. Large mucosal ulcers with copious purulent exudate characterize severe disease. Islands of relatively normal or hyperplastic inflammatory mucosa (pseudopolyps) project above areas of ulcerated mucosa. Fistulas and abscesses do not occur.





Toxic colitis
Toxic colitis or fulminant colitis occurs when transmural extension of ulceration results in localized ileus and peritonitis. Within hours to days, the colon loses muscular tone and begins to dilate.
The terms toxic megacolon and toxic dilation are discouraged because the toxic inflammatory state and its complications can occur without frank megacolon (defined as transverse colon > 6 cm diameter during an exacerbation).
Toxic colitis is a medical emergency that usually occurs spontaneously in the course of very severe colitis but is sometimes precipitated by opioid or anticholinergic antidiarrheal drugs. Colonic perforation may occur, which increases mortality significantly.
Symptoms and Signs of Ulcerative Colitis
Patients typically have
Attacks of bloody diarrhea of varied intensity and duration interspersed with asymptomatic intervals
Usually an attack begins insidiously, with increased urgency to defecate, mild lower abdominal cramps, and blood and mucus in the stools. Some cases develop after an infection (eg, amebiasis, bacillary dysentery).
When ulceration is confined to the rectosigmoid, the stool may be normal or hard and dry, but rectal discharges of mucus loaded with red and white blood cells accompany or occur between bowel movements. Systemic symptoms are absent or mild.
If ulceration extends proximally, stools become looser and the patient may have > 10 bowel movements per day, often with severe cramps and distressing rectal tenesmus, without respite at night. The stools may be watery or contain mucus and frequently consist almost entirely of blood and pus.
Toxic or fulminant colitis manifests initially with sudden violent diarrhea, fever to 40° C (104° F), abdominal pain, signs of peritonitis (eg, rebound tenderness), and profound toxemia.
Systemic symptoms and signs, more common with extensive ulcerative colitis, include malaise, fever, anemia, anorexia, and weight loss. Extraintestinal manifestations of inflammatory bowel disease (IBD), particularly joint and skin complications, are most common when systemic symptoms are present.
Diagnosis of Ulcerative Colitis
Stool cultures and microscopy (to exclude infectious causes)
Sigmoidoscopy with biopsy
Initial presentation
Diagnosis of ulcerative colitis is suggested by typical symptoms and signs, particularly when accompanied by extraintestinal manifestations or a history of previous similar attacks. Ulcerative colitis should be distinguished from Crohn disease (see table Differentiating Crohn Disease and Ulcerative Colitis) but more importantly from other causes of acute colitis (eg, infection; in older patients, ischemia).
In all patients, stool cultures for enteric pathogens should be done, and Entamoeba histolytica should be excluded by examination of fresh stool specimens. When amebiasis is suspected because of epidemiologic or travel history, serologic titers and biopsies should be done. History of prior antibiotic use or recent hospitalization should prompt stool assay for Clostridioides difficile (formerly Clostridium difficile) toxin. Patients at risk should be tested for HIV, gonorrhea, herpesvirus, chlamydia, and amebiasis. Opportunistic infections (eg, cytomegalovirus, Mycobacterium avium-intracellulare) or Kaposi sarcoma must also be considered in immunosuppressed patients. In women using oral contraceptives, contraceptive-induced colitis is possible; it usually resolves spontaneously after hormone therapy is stopped. Stool testing for lactoferrin and fecal calprotectin can be beneficial in differentiating IBD from functional diarrhea.
Sigmoidoscopy should be done; it allows visual confirmation of colitis and permits direct sampling of stool or mucus for culture and microscopic evaluation, as well as biopsy of affected areas. Although visual inspection and biopsies may be nondiagnostic, because there is much overlap in appearance among different types of colitis, acute, self-limited, infectious colitis can usually be distinguished histologically from chronic idiopathic ulcerative colitis or Crohn colitis. Severe perianal disease, rectal sparing, absence of bleeding, and asymmetric or segmental involvement of the colon indicate Crohn disease rather than ulcerative colitis. Colonoscopy is usually unnecessary initially but should be done electively if inflammation has extended proximal to the reach of the sigmoidoscope.
Laboratory tests should be done to screen for anemia, hypoalbuminemia, and electrolyte abnormalities. Liver tests should be done; elevated alkaline phosphatase and gamma-glutamyl transpeptidase levels suggest possible primary sclerosing cholangitis. Perinuclear antineutrophil cytoplasmic antibodies are relatively specific (60 to 70%) for ulcerative colitis. Anti–Saccharomyces cerevisiae antibodies are relatively specific for Crohn disease. However, these tests do not reliably separate the 2 diseases and are not recommended for routine diagnosis. Other possible laboratory abnormalities include leukocytosis, thrombocytosis, and elevated acute-phase reactants (eg, erythrocyte sedimentation rate, C-reactive protein).
X-rays are not diagnostic but occasionally show abnormalities. Plain x-rays of the abdomen may show mucosal edema, loss of haustration, and absence of formed stool in the diseased bowel; however, the yield is low and they are not recommended routinely. Barium enema shows similar changes, albeit more clearly, and may also show ulcerations, but the enema should not be done during an acute presentation. A shortened, rigid colon with an atrophic or pseudopolypoid mucosa is often seen after several years of illness. X-ray findings of thumbprinting and segmental distribution are more suggestive of intestinal ischemia or possibly Crohn colitis rather than of ulcerative colitis.
Recurrent symptoms
Patients with known disease and a recurrence of typical symptoms should be examined, but extensive testing is not always required. Depending on duration and severity of symptoms, sigmoidoscopy or colonoscopy may be done and a complete blood count obtained. Cultures, ova and parasite examination, and C. difficile toxin assay should be done when there are atypical features to the relapse or when there is an exacerbation after prolonged remission, during a contagious outbreak, after antibiotic exposure, or whenever the clinician is suspicious.
Acute severe attacks
Patients require prompt hospitalization during severe flare-ups. Flat and upright abdominal x-rays should be taken; they may show megacolon or intraluminal gas accumulated over a long, continuous, paralyzed segment of colon—a result of lost muscle tone. Barium enema should be avoided because of the risk of perforation, but a careful sigmoidoscopy is typically advisable to assess severity and rule out infection. Complete blood count, platelet count, erythrocyte sedimentation rate, C-reactive protein, electrolytes, and albumin should be obtained; prothrombin time, partial thromboplastin time, and blood type and cross-match are also indicated in cases of severe bleeding.Patients require prompt hospitalization during severe flare-ups. Flat and upright abdominal x-rays should be taken; they may show megacolon or intraluminal gas accumulated over a long, continuous, paralyzed segment of colon—a result of lost muscle tone. Barium enema should be avoided because of the risk of perforation, but a careful sigmoidoscopy is typically advisable to assess severity and rule out infection. Complete blood count, platelet count, erythrocyte sedimentation rate, C-reactive protein, electrolytes, and albumin should be obtained; prothrombin time, partial thromboplastin time, and blood type and cross-match are also indicated in cases of severe bleeding.
The patient must be watched closely for progressive peritonitis or perforation. Percussion over the liver is important because loss of hepatic dullness may be the first clinical sign of free perforation, especially in a patient whose peritoneal signs are suppressed by high-dose corticosteroids. Abdominal x-rays are taken every 1 or 2 days to follow the course of colonic distention and to detect free or intramural air; CT is more sensitive in detecting extraluminal air or pericolic abscess.
Pearls & Pitfalls
|
Treatment of Ulcerative Colitis
Dietary management and loperamide (except in acute severe attacks) for symptom reliefDietary management and loperamide (except in acute severe attacks) for symptom relief
5-Aminosalicylic acid (5-ASA)
Corticosteroids and other drugs depending on symptoms and severity
Antimetabolites, biologic agents, a Janus kinase inhibitor, or sphingosine 1-phosphate (S1P) receptor modulator
Sometimes surgery
Details of specific medications and dosages are discussed in Medications for Inflammatory Bowel Disease. (See also the American College of Gastroenterology's 2019 guidelines for management of ulcerative colitis in adults.)
General management
Avoiding raw fruits and vegetables limits trauma to the inflamed colonic mucosa and may lessen symptoms. A milk-free diet may help but need not be continued if no benefit is noted. Loperamide 2 mg orally 2 to 4 times a day is indicated for relatively mild diarrhea; higher oral doses (4 mg in the morning and 2 mg after each bowel movement) may be required for more intense diarrhea. Antidiarrheal drugs must be used with extreme caution in severe cases because they may precipitate toxic dilation. All patients with inflammatory bowel disease should be advised to take appropriate amounts of calcium and vitamin D.Avoiding raw fruits and vegetables limits trauma to the inflamed colonic mucosa and may lessen symptoms. A milk-free diet may help but need not be continued if no benefit is noted. Loperamide 2 mg orally 2 to 4 times a day is indicated for relatively mild diarrhea; higher oral doses (4 mg in the morning and 2 mg after each bowel movement) may be required for more intense diarrhea. Antidiarrheal drugs must be used with extreme caution in severe cases because they may precipitate toxic dilation. All patients with inflammatory bowel disease should be advised to take appropriate amounts of calcium and vitamin D.
Routine health maintenance measures (eg, immunizations, cancer screening) should be emphasized.
Mild left-sided disease
Patients with mild to moderate ulcerative proctitis or proctosigmoiditis that does not extend proximally beyond the sigmoid colon are treated with 5-ASA (mesalamine) by enema once a day or twice a day depending on severity. Suppositories are effective for more distal disease and are usually preferred by patients. Corticosteroid and budesonide enemas are slightly less effective but should be used if 5-ASA is unsuccessful or not tolerated. Once remission is achieved, dosage is slowly tapered to maintenance levels. Oral 5-ASA drugs theoretically have some incremental benefit in lessening the probability of proximal spread of disease.(mesalamine) by enema once a day or twice a day depending on severity. Suppositories are effective for more distal disease and are usually preferred by patients. Corticosteroid and budesonide enemas are slightly less effective but should be used if 5-ASA is unsuccessful or not tolerated. Once remission is achieved, dosage is slowly tapered to maintenance levels. Oral 5-ASA drugs theoretically have some incremental benefit in lessening the probability of proximal spread of disease.
Moderate or extensive disease
Patients with inflammation proximal to the sigmoid colon or left-sided disease unresponsive to topical agents should receive a biologic agent (infliximab, adalimumab, golimumab, ustekinumab, vedolizumab) with or without an immunomodulator medication (azathioprine or 6-mercaptopurine). Sometimes, high-dose (infliximab, adalimumab, golimumab, ustekinumab, vedolizumab) with or without an immunomodulator medication (azathioprine or 6-mercaptopurine). Sometimes, high-dosecorticosteroids are added for inducing remission in patients with moderate to severe ulcerative colitis. A combination of immunomodulator and anti-TNF therapy is sometimes helpful. Finally, in some patients, a trial of the Janus kinase inhibitor (tofacitinib or upadacitinib), or a trial of sphingosine 1-phosphate receptor modulator ozanimod can be considered.is sometimes helpful. Finally, in some patients, a trial of the Janus kinase inhibitor (tofacitinib or upadacitinib), or a trial of sphingosine 1-phosphate receptor modulator ozanimod can be considered.
Severe disease
Patients with > 10 bloody bowel movements per day, tachycardia, high fever, or severe abdominal pain require hospitalization to receive biologic agent and/or high-dose IV corticosteroids. IV fluids and blood transfusion are given as needed for dehydration and anemia. The patient must be observed closely for the development of toxic colitis. Parenteral hyperalimentation is sometimes used for nutritional support but is of no value as primary therapy; patients who can tolerate food should eat.
Patients who do not respond to biologic agents and/or corticosteroids within 3 to 7 days should be considered for IV cyclosporine or for surgery. Patients who do respond to a corticosteroid regimen are switched within a week or so to prednisone 40 mg orally once a day, which may be gradually reduced at home based on clinical response. Patients who are started on IV cyclosporine and respond to therapy are switched to oral cyclosporine and concomitant azathioprine or 6-mercaptopurine. Oral cyclosporine is continued for about 3 to 4 months, during which time corticosteroids are tapered and cyclosporine levels are closely monitored. Some clinicians recommend or for surgery. Patients who do respond to a corticosteroid regimen are switched within a week or so to prednisone 40 mg orally once a day, which may be gradually reduced at home based on clinical response. Patients who are started on IV cyclosporine and respond to therapy are switched to oral cyclosporine and concomitant azathioprine or 6-mercaptopurine. Oral cyclosporine is continued for about 3 to 4 months, during which time corticosteroids are tapered and cyclosporine levels are closely monitored. Some clinicians recommendprophylaxis against Pneumocystis jirovecii pneumonia during the interval of overlapping treatment with corticosteroids, cyclosporine, and an antimetabolite. Tacrolimus, an immunosuppressant also used in transplant patients, seems as effective as cyclosporine and may be considered for use in patients with severe or refractory ulcerative colitis who do not require hospitalization. The trough blood levels should be kept between 10 to 15 ng/mL (12 to 25 nmol/L).pneumonia during the interval of overlapping treatment with corticosteroids, cyclosporine, and an antimetabolite. Tacrolimus, an immunosuppressant also used in transplant patients, seems as effective as cyclosporine and may be considered for use in patients with severe or refractory ulcerative colitis who do not require hospitalization. The trough blood levels should be kept between 10 to 15 ng/mL (12 to 25 nmol/L).
Fulminant colitis
If fulminant or toxic colitis is suspected, the patient should
Stop all antidiarrheal medications
Take nothing by mouth and have inserted a long intestinal tube attached to intermittent suction
Receive aggressive IV fluid and electrolyte therapy with 0.9% sodium chloride, and potassium chloride and blood as neededReceive aggressive IV fluid and electrolyte therapy with 0.9% sodium chloride, and potassium chloride and blood as needed
Receive high-dose IV corticosteroids or cyclosporineReceive high-dose IV corticosteroids or cyclosporine
Receive antibiotics (eg, metronidazole 500 mg IV every 8 hours and ciprofloxacin 500 mg IV every 12 hours)Receive antibiotics (eg, metronidazole 500 mg IV every 8 hours and ciprofloxacin 500 mg IV every 12 hours)
Perhaps receive infliximabPerhaps receive infliximab
Having the patient roll over in bed from the supine to prone position every 2 to 3 hours may help redistribute colonic gas and prevent progressive distention. Insertion of a soft rectal tube may also be helpful but must be done with extreme caution to avoid bowel perforation. Even if decompression of a dilated colon is achieved, the patient is not out of danger unless the underlying inflammatory process is controlled; otherwise, colectomy will still be necessary.
If intensive medical measures do not produce definite improvement within 24 to 48 hours, immediate surgery is required or the patient may die of sepsis caused by bacterial translocation or even perforation.
Maintenance therapy
After effective treatment of a flare-up, corticosteroids are tapered based on clinical response and then stopped because they are ineffective as maintenance. Patients should remain on 5-ASA drugs—oral or rectal, depending on location of disease—indefinitely because stopping maintenance therapy often allows disease relapse. Dosage intervals for rectal preparations may be gradually lengthened to every 2nd or 3rd day. There is ample evidence that combination oral and rectal therapy is significantly more effective than either therapy alone.
Patients who cannot be withdrawn from corticosteroids should be given thiopurines (azathioprine or 6-mercaptopurine), methotrexate, biologics, Janus kinase inhibitors, the sphingosine 1-phosphate receptor modulator ozanimod, or a combination of these medications.Patients who cannot be withdrawn from corticosteroids should be given thiopurines (azathioprine or 6-mercaptopurine), methotrexate, biologics, Janus kinase inhibitors, the sphingosine 1-phosphate receptor modulator ozanimod, or a combination of these medications.
Patients started on infliximab for induction therapy should continue this medication for maintenance, too.Patients started on infliximab for induction therapy should continue this medication for maintenance, too.
Surgery
Nearly one third of patients with extensive ulcerative colitis ultimately require surgery. Total proctocolectomy is curative: Life expectancy is restored to normal, and the risk of colon cancer is significantly decreased. However, some studies report up to 25% of patients subsequently develop inflammation in the small bowel mucosa consistent with Crohn disease (1, 2); this may occur many years after surgery. After total proctocolectomy with ileal pouch-anal anastomosis (IPAA), there remains a small risk of dysplasia or cancer in the rectal cuff anal transition zone and even in the ileal pouch. After proctocolectomy with ileostomy or IPAA, the quality of life is improved; however, new quality-of-life challenges are created.
Emergency colectomy is indicated for massive hemorrhage, fulminating toxic colitis, or perforation. Subtotal colectomy with ileostomy and rectosigmoid closure (Hartmann procedure) or mucous fistula is usually the procedure of choice because most critically ill patients cannot tolerate more extensive surgery. The rectosigmoid stump may be electively removed later or may be used for ileoanal anastomosis with a pouch. The intact rectal stump should not be allowed to remain indefinitely because of the risks of disease activation and malignant transformation.
Elective surgery is indicated for cancer, symptomatic strictures, growth retardation in children, or, most commonly, intractable chronic disease resulting in invalidism or corticosteroid dependence. Severe colitis-related extraintestinal manifestations (eg, pyoderma gangrenosum), now better controlled by intensive medical therapies, are only rarely indications for surgery.
The elective procedure of choice in patients with normal sphincter function is restorative proctocolectomy with ileoanal anastomosis. This procedure creates a pelvic reservoir or pouch from distal ileum, which is connected to the anus. The intact sphincter allows continence, typically with 4 to 9 bowel movements/day (including 1 or 2 at night).
Pouchitis is an inflammatory reaction occurring after restorative proctocolectomy with IPAA+ in about 50% of patients. The risk of pouchitis appears to be higher in patients with primary sclerosing cholangitis, in patients with preoperative extraintestinal manifestations, and possibly in patients with high preoperative serologic titers of perinuclear antineutrophilic antibodies and other inflammatory bowel disease biomarkers. Pouchitis is thought to be related to bacterial overgrowth and is treated with antibiotics (eg, quinolones). Probiotics may be protective. Most cases of pouchitis are readily controlled, but 5 to 10% prove refractory to all medical therapy and require conversion to a conventional (Brooke) ileostomy. For a minority of patients who are older, who have well-established families and lifestyles, who have poor sphincter tone or cannot tolerate frequent bowel movements, or who are simply unable or unwilling to face the consequences of frequent or chronic pouchitis, the Brooke ileostomy remains the procedure of choice.
Ileitis after IPAA or end ileostomy is managed the same as other forms of IBD. Surgical procedures are rarely required.
In any event, the physical and emotional burdens imposed by any form of colon resection must be recognized, and care should be taken to see that the patient receives all the instructions and all the medical and psychologic support that is necessary before and after surgery.

Treatment references
1. Hercun J, Côté-Daigneault J, Lahaie RG, et al: Crohn's disease after proctocolectomy and IPAA for ulcerative colitis. Dis Colon Rectum 64(2):217–224, 2021. doi: 10.1097/DCR.0000000000001721
2. Shamah S, Schneider J, Korelitz BI: High incidence of recurrent Crohn's disease following colectomy for ulcerative colitis revealed with long follow-up. Dig Dis Sci 63(2):446–451, 2018. doi: 10.1007/s10620-017-4873-7
Prognosis for Ulcerative Colitis
Usually, ulcerative colitis is chronic with repeated exacerbations and remissions. In some of patients, an initial attack becomes fulminant with massive hemorrhage, perforation, or sepsis and toxemia. Complete recovery after a single attack occurs in a few patients.
Patients with localized ulcerative proctitis have the best prognosis. Severe systemic manifestations, toxic complications, and malignant degeneration are unlikely, and late extension of the disease occurs only in a small group of patients. Surgery is rarely required, and life expectancy is normal. The symptoms, however, may prove stubborn and refractory. Moreover, because extensive ulcerative colitis may begin in the rectum and spread proximally, proctitis should not be considered localized until it has been observed for ≥ 6 months. Localized disease that later extends is often more severe and more refractory to therapy.
Colon cancer
The risk of colon cancer is proportional to the duration of disease and amount of colon affected but not necessarily to the clinical severity of the attacks. Some studies suggest that sustained microscopic inflammation is a risk factor, and that use of 5-aminosalicylic acid (5-ASA) to control inflammation is protective.
The high risk of colon cancer conferred by IBD has been noted in multiple studies. More recent data suggests that the prevalence of colon cancer is decreasing and was overestimated by researches at tertiary care centers (1).
Patients who have inflammatory bowel disease and primary sclerosing cholangitis are at a higher risk of cancer from the time of colitis diagnosis.
Regular colonoscopic surveillance, preferably during remission, is advised for patients with disease duration > 8 to 10 years (except for those with isolated proctitis) or when there is concomitant primary sclerosing cholangitis, in which case surveillance colonoscopy should begin at the time of diagnosis. The guidelines (2) suggest doing random biopsies (taken every 10 cm throughout the colon) when using high-definition white-light colonoscopy but doing only targeted biopsies of visible lesions when using chromoendoscopy to detect dysplasia. Definite dysplasia of any grade within an area affected by colitis is liable to progress to more advanced neoplasia and even cancer. After complete removal of endoscopically resectable polypoid or nonpolypoid dysplastic lesions, colonoscopic surveillance is suggested rather than colectomy. Patients with dysplasia that is not visible endoscopically should probably be referred to a gastroenterologist with expertise in IBD surveillance using chromoendoscopy and/or high-definition colonoscopy to decide whether colectomy or continued colonoscopic surveillance should be done.
The optimal frequency of colonoscopic surveillance has not been established, but some authorities recommend every 2 years during the 2nd decade of disease and annually thereafter.
Long-term survival after diagnosis of colitis-related cancer is about 50%, a figure comparable to that for colorectal cancer in the general population.
Prognosis references
1. Stidham RW, Higgins PDR: Colorectal cancer in inflammatory bowel disease. Clin Colon Rectal Surg 31(3):168-178, 2018. doi: 10.1055/s-0037-1602237
2. Laine L, Kaltenbach T, Barkun A, et al: SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology 148(3):639-651.e28, 2015. doi: 10.1053/j.gastro.2015.01.031
Key Points
Ulcerative colitis begins in the rectum and may extend proximally in a contiguous fashion without intervening patches of normal bowel.
Symptoms are intermittent episodes of abdominal cramping and bloody diarrhea.
Complications include fulminant colitis, which may lead to perforation; long-term, the risk of colon cancer is increased.
Treat mild disease with 5-ASA by rectum and, for proximal disease, by mouth.
Treat extensive disease with high-dose corticosteroids, immunomodulator therapy (eg, azathioprine, 6-mercaptopurine), biologics (eg, adalimumab, infliximab, vedolizumab), tofacitinib, upadacitinib, or ozanimod.Treat extensive disease with high-dose corticosteroids, immunomodulator therapy (eg, azathioprine, 6-mercaptopurine), biologics (eg, adalimumab, infliximab, vedolizumab), tofacitinib, upadacitinib, or ozanimod.
Treat fulminant disease with high-dose IV corticosteroids or cyclosporine and antibiotics (eg, metronidazole, ciprofloxacin) or infliximab; colectomy may be required.Treat fulminant disease with high-dose IV corticosteroids or cyclosporine and antibiotics (eg, metronidazole, ciprofloxacin) or infliximab; colectomy may be required.
About one third of patients with extensive ulcerative colitis ultimately require surgery.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
American College of Gastroenterology: Guidelines for the management of ulcerative colitis in adults (2019)







