



Chagas disease is infection with Trypanosoma cruzi, transmitted by Triatominae bug bites or, less commonly, via ingestion of sugar cane juice or foods contaminated with infected Triatominae bugs or their feces, via blood transfusion or an organ transplant from an infected donor, or via maternal-fetal transmission. Symptoms after a Triatominae bite typically begin with a skin lesion or unilateral periorbital edema, then progress to fever, malaise, generalized lymphadenopathy, and hepatosplenomegaly; years later, 20 to 30% of infected patients develop arrhythmias, chronic cardiomyopathy, or, less commonly, megaesophagus or megacolon. In patients with AIDS, the skin or brain may be affected. Diagnosis is by detecting trypanosomes in peripheral blood or aspirates from infected organs. Antibody tests are sensitive and can be helpful. Treatment is with nifurtimox or benznidazole; however, antiparasitic drugs do not reverse the course of cardiac or intestinal disease that has developed., transmitted by Triatominae bug bites or, less commonly, via ingestion of sugar cane juice or foods contaminated with infected Triatominae bugs or their feces, via blood transfusion or an organ transplant from an infected donor, or via maternal-fetal transmission. Symptoms after a Triatominae bite typically begin with a skin lesion or unilateral periorbital edema, then progress to fever, malaise, generalized lymphadenopathy, and hepatosplenomegaly; years later, 20 to 30% of infected patients develop arrhythmias, chronic cardiomyopathy, or, less commonly, megaesophagus or megacolon. In patients with AIDS, the skin or brain may be affected. Diagnosis is by detecting trypanosomes in peripheral blood or aspirates from infected organs. Antibody tests are sensitive and can be helpful. Treatment is with nifurtimox or benznidazole; however, antiparasitic drugs do not reverse the course of cardiac or intestinal disease that has developed.
Topic Resources


Chagas disease is caused by Trypanosoma cruzi. Infection is transmitted to humans when bitten by Triatominae (reduviid, kissing, or assassin) bugs in South and Central America, Mexico, and very rarely in the US. Less commonly, T. cruzi is transmitted via ingestion of sugar cane juice or food contaminated with infected Triatominae bugs or their feces, transplacentally from an infected mother to her fetus, or via blood transfusion or an organ transplant from an infected donor.
Nonhuman reservoirs include domestic dogs, opossums, armadillos, rats, raccoons, and many other animals.
Worldwide, an estimated 8 million people are chronically infected with T. cruzi. Most reside in Latin America, but about 300,000 of those infected in Latin America now live in the US; others live in Europe or elsewhere (see Centers for Disease Control and Prevention: Epidemiology & Risk Factors). The incidence of T. cruzi infection has been decreasing in Latin America because of improved housing, screening of blood and organ donors, and other control measures.
There are an estimated 40,000 T. cruzi-infected women of childbearing age in the US. It is estimated that 1 to 5% of their children are born with congenital infection.
Pathophysiology of Chagas Disease
Chagas disease is most commonly spread when a Triatominae bug bites an infected person or animal, then bites another person. While biting, infected bugs deposit feces containing metacyclic trypomastigotes on the skin. These infective forms enter through the bite wound or penetrate the conjunctivae or mucous membranes.
The parasites invade macrophages at the site of entry and transform into amastigotes that multiply by binary fission; the amastigotes develop into trypomastigotes, enter the bloodstream and tissue spaces, and infect other cells. Cells of the reticuloendothelial system, myocardium, muscles, and nervous system are most commonly involved.

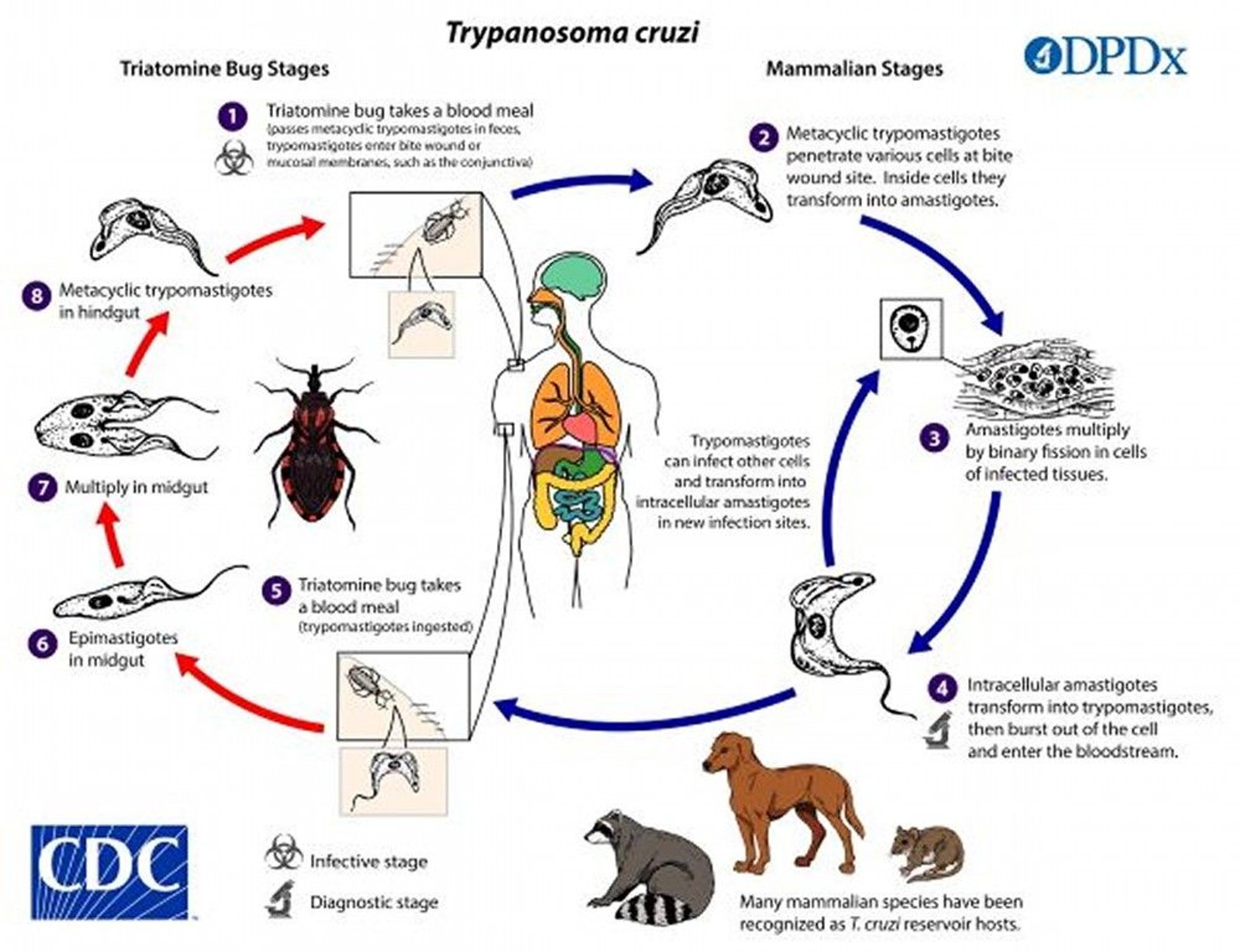
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Symptoms and Signs of Chagas Disease
T. cruzi infection has 3 stages:
Acute
Chronic indeterminate
Chronic
Acute infection is followed by a latent (chronic indeterminate) period, which may remain asymptomatic or progress to chronic disease. Immunosuppression may reactivate infection, causing high parasitemia and in some people skin or brain lesions.
Acute
Acute T. cruzi infection in endemic areas usually occurs in childhood and can be asymptomatic. When present, symptoms start 1 to 2 weeks after exposure. An indurated, erythematous skin lesion (a chagoma) appears at the site of parasite entry. When the inoculation site is the conjunctiva, unilateral periocular and palpebral edema with conjunctivitis and preauricular lymphadenopathy are collectively called the Romaña sign.


CDC image courtesy of the WHO/TDR Image Library.
Acute Chagas disease is fatal in a small percentage of patients; death results from acute myocarditis with heart failure or meningoencephalitis. In the remainder, symptoms subside without treatment.
Primary acute Chagas disease in immunocompromised patients, such as those with AIDS, may be severe and atypical, with skin lesions and, rarely, ring-enhancing brain lesions.
Congenital infections are mostly asymptomatic, but in 10 to 40% of cases nonspecific manifestations occur, including prematurity, low birth weight, fever, hepatosplenomegaly, anemia, and thrombocytopenia. Rarely, death can result from fulminant disease. Signs of acute infection resolve even without therapy in the majority of congenital infections.
Chronic indeterminate
Patients with chronic indeterminate infection have parasitologic and/or serologic evidence of T. cruzi infection but have neither symptoms, abnormal physical findings, nor evidence of cardiac or gastrointestinal involvement as assessed by ECG and rhythm strip, cardiac ultrasonography, chest x-ray, or other studies.
Many infected patients are identified by screening enzyme-linked immunosorbent blood assay (ELISA) and confirmatory radioimmunoprecipitation assay (RIPA) when they donate blood.
Chronic with cardiac or intestinal tract involvement
Chronic Chagas disease develops in 20 to 30% of patients after the chronic indeterminate phase, which may last years or decades. The parasites are probably present in chronic disease; an autoimmune reaction also may contribute to organ damage. The main effects are
Cardiac
Gastrointestinal
Cardiac disease usually manifests with conduction abnormalities including right bundle branch block or left anterior fascicular block. Chronic cardiomyopathy often follows with flaccid enlargement of all chambers, apical aneurysms, and progression of lesions in the conduction system. Patients may present with heart failure, syncope, sudden death due to heart block or ventricular arrhythmia, or thromboembolism. ECG may show right bundle branch or complete heart block.
Gastrointestinal disease manifests with symptoms resembling achalasia or Hirschsprung disease. Chagas megaesophagus manifests as dysphagia and may lead to pulmonary infections caused by aspiration or to severe undernutrition. Megacolon may result in long periods of obstipation and intestinal volvulus.
Diagnosis of Chagas Disease
Light microscopy of blood smears (thin or thick) or tissue (acute Chagas disease)
Screening serologic test confirmed by a second test
Polymerase chain reaction–based tests
The number of trypanosomes in peripheral blood is large during the acute phase of Chagas disease and can be readily detected by examining thin or thick smears. In contrast, few parasites are present in blood during latent infection or chronic disease. Definitive diagnosis of acute-stage Chagas disease may also be made by examining tissue from lymph nodes or heart.
In immunocompetent patients with chronic Chagas disease, serologic tests, such as indirect fluorescent antibody (IFA), enzyme immunoassays (EIA), or enzyme-linked immunosorbent assay (ELISA), are often done to detect antibodies to T. cruzi. Serologic tests are sensitive but may yield false-positive results in patients with leishmaniasis or other diseases. Thus, an initial positive test is followed by one or more different tests (typically, radioimmunoprecipitation assay [RIPA] in the US) or sometimes light microscopy of blood smears or a tissue sample to confirm the diagnosis. Serologic tests are also used to screen blood donors for T. cruzi in endemic areas and the US.
Polymerase chain reaction (PCR)–based tests are used when the level of parasitemia is likely to be high, as occurs in acute Chagas disease, in transplacentally transmitted (congenital) Chagas disease, or after transmission via blood transfusion, transplantation, or laboratory exposure. In endemic areas, xenodiagnosis has been used; it involves examining the intestinal contents of Triatominae bugs raised in a laboratory after they took a blood meal from a person thought to have Chagas disease.
Ancillary testing in patients with chronic Chagas disease
After Chagas disease is diagnosed, the following tests should be done, depending on findings:
No symptoms but documented T. cruzi infection: A screening ECG and rhythm strip and a chest x-ray
Potential cardiac abnormalities on a screening test or symptoms suggesting heart disease: Echocardiography
Dysphagia or other gastrointestinal (GI) symptoms or findings: GI contrast studies and/or endoscopy
Treatment of Chagas Disease
Benznidazole or nifurtimoxBenznidazole or nifurtimox
Supportive care
Treatment of acute-stage Chagas disease with antiparasitic drugs does the following:
Rapidly reduces parasitemia
Shortens the clinical illness
Reduces risk of mortality
Decreases the likelihood of chronic disease
Antiparasitic treatment is indicated for all cases of acute, congenital, or reactivated Chagas disease and for chronic indeterminate infection in children up to age 18 years. The younger the patient and the earlier treatment is started, the more likely that treatment will result in parasitologic cure.
The efficacy of treatment decreases as the duration of infection lengthens, and adverse effects are more likely in adults. Treatment is indicated for T. cruzi-infected children up to age 18 years. It is recommended for those 18 to 50 years unless they have evidence of advanced cardiac or gastrointestinal (GI) disease. For patients > 50 years, treatment is individualized based on potential risks and benefits.
Once signs of advanced cardiac or GI disease appear, antiparasitic drugs are not recommended.
Supportive measures include treatment for heart failure, pacemakers for heart block, antiarrhythmic medications, cardiac transplantation, esophageal dilation, botulinum toxin injection into the lower esophageal sphincter, and GI tract surgery for megacolon.
The only effective antiparasitic drugs are
Benznidazole:Benznidazole: For adults and children > 12 years, 2.5 to 3.5 mg/kg orally twice a day for 60 days
For children ≤ 12 years, 2.5 to 3.75 mg/kg twice a day for 60 days
Nifurtimox:Nifurtimox: For patients ≥ 17 years, 2 to 2.5 mg/kg orally 4 times a day for 90 days
For children aged 11 to 16 years, 3 to 3.75 mg/kg 4 times a day for 90 days
For children aged 1 to 10 years, 4 to 5 mg/kg 4 times a day for 90 days
Benznidazole is generally better tolerated, and the duration of treatment is shorter. Both benznidazole and nifurtimox have substantial toxicity, which increases with age. Contraindications for treatment include severe liver or kidney disease. Young children usually tolerate treatment better than adults. When women are diagnosed with Chagas during pregnancy, treatment is typically delayed until after delivery, and the infant is then treated if infected.Benznidazole is generally better tolerated, and the duration of treatment is shorter. Both benznidazole and nifurtimox have substantial toxicity, which increases with age. Contraindications for treatment include severe liver or kidney disease. Young children usually tolerate treatment better than adults. When women are diagnosed with Chagas during pregnancy, treatment is typically delayed until after delivery, and the infant is then treated if infected.
Common adverse effects of benznidazole include allergic dermatitis, anorexia, weight loss, peripheral neuropathy, and insomnia. Common adverse effects of benznidazole include allergic dermatitis, anorexia, weight loss, peripheral neuropathy, and insomnia.
Common adverse effects of nifurtimox are anorexia, nausea, vomiting, weight loss, polyneuropathy, headache, dizziness, and vertigo.Common adverse effects of nifurtimox are anorexia, nausea, vomiting, weight loss, polyneuropathy, headache, dizziness, and vertigo.
It is recommended that these medications not be used in pregnant women or in breastfeeding mothers.
Prevention of Chagas Disease
Plastering walls and replacing thatched roofs or repeated spraying of houses with residual insecticides (those that have prolonged duration of action) can control Triatominae bugs. Infection in travelers is rare and can be avoided by not sleeping in adobe dwellings or, if sleeping in such dwellings is unavoidable, by using bed nets.
Another preventive measure is avoiding fresh sugar cane juice or other foods that might be contaminated.
Screening of at-risk women of childbearing age and treatment before pregnancy decrease the likelihood of congenital infection.
Blood and organ donors are screened in many endemic areas and, since 2006, in the US to prevent transfusion- and organ transplant–related Chagas disease.
Key Points
Chagas disease is caused by Trypanosoma cruzi, which is transmitted by Triatominae (reduviid, kissing, or assassin) bugs.
Infection is endemic in South and Central America and Mexico; an estimated 8 million people worldwide, including an estimated 300,000 people in the US (primarily immigrants), are infected.
Acute infection is followed by a chronic indeterminate period, which may remain asymptomatic, but in 20 to 30% of patients, it progresses to chronic disease, which particularly affects the heart and/or gastrointestinal (GI) tract.
Diagnose acute Chagas using light microscopy of blood smears (thin or thick) or a tissue sample or PCR-based assays.
Diagnose chronic T. cruzi infection by screening enzyme-linked immunosorbent blood assay (ELISA) with confirmatory radioimmunoprecipitation assay (RIPA) or other assay for antibodies.
Use PCR-based tests to evaluate cases potentially transmitted transplacentally or via transfusion, transplantation, or laboratory exposure.
To detect chronic Chagas disease, do echocardiography if patients have symptoms suggesting heart disease or potential cardiac abnormalities on a chest x-ray, ECG, or rhythm strip; do GI contrast studies or endoscopy if they have dysphagia or other GI symptoms.
The antiparasitic drugs benznidazole or nifurtimox are used to treat acute, congenital, or reactivated Chagas disease. They are also used for chronic infection in children up to age 18 years. They are strongly recommended for adults 18 to 50 years who do not have advanced cardiac or evidence of GI disease. For patients > 50 years with chronic infection, treatment is individualized based on balance of risks and benefits. The antiparasitic drugs benznidazole or nifurtimox are used to treat acute, congenital, or reactivated Chagas disease. They are also used for chronic infection in children up to age 18 years. They are strongly recommended for adults 18 to 50 years who do not have advanced cardiac or evidence of GI disease. For patients > 50 years with chronic infection, treatment is individualized based on balance of risks and benefits.
Antiparasitic drugs are not effective in patients with advanced Chagas cardiac or gastrointestinal disease, but supportive measures (eg, treatment of heart failure, pacemakers for heart block, antiarrhythmic drugs, cardiac transplantation, esophageal dilation, botulinum toxin injection into the lower esophageal sphincter, GI tract surgery) are often helpful.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.







