



Rickettsial diseases (rickettsioses) and related diseases (anaplasmosis, ehrlichiosis, Q fever, scrub typhus) are caused by a group of gram-negative, obligately intracellular coccobacilli. All, except for Coxiella burnetii, have an arthropod vector. Symptoms usually include sudden-onset fever with severe headache, malaise, prostration, and, in most cases, a characteristic rash. Diagnosis is clinical, confirmed by immunofluorescence assay or polymerase chain reaction (PCR). First-line treatment is with doxycycline., have an arthropod vector. Symptoms usually include sudden-onset fever with severe headache, malaise, prostration, and, in most cases, a characteristic rash. Diagnosis is clinical, confirmed by immunofluorescence assay or polymerase chain reaction (PCR). First-line treatment is with doxycycline.

")





Rickettsia, Orientia, Ehrlichia, Anaplasma, and Coxiella species were once thought to belong to the same family but now, based on genetic analysis, are considered distinct entities. Although this group of organisms require living cells for growth, they are true bacteria because they have metabolic enzymes and cell walls, use oxygen, and are susceptible to antibiotics.
These organisms typically have an animal reservoir and an arthropod vector; exceptions are R. prowazekii, for which humans are the primary reservoir, and C. burnetii, which does not require an arthropod vector. For some organisms (eg, R. rickettsii and other spotted fever rickettsia, and R. akari, R. felis, and Orientia), the vector is also the reservoir, and the geographic distribution of these rickettsia is determined by that of the infected arthropod. Specific vectors, reservoirs, and endemic regions differ widely (see table Diseases Caused by Rickettsia, Orientia, Ehrlichia, Anaplasma, and Coxiella Species).
There are many rickettsial species, but 3 cause most human rickettsial infections:
R. rickettsii
R. prowazekii
R. typhi
Diseases Caused by Rickettsia, Orientia, Ehrlichia, Anaplasma, and Coxiella Species
Disease | Organism | Rash or Eschar | Vector | Endemic Region |
|---|---|---|---|---|
Typhus | ||||
Rickettsia prowazekii | Trunk to extremities May be absent in Brill-Zinsser disease No eschar | Body lice | Worldwide | |
R. typhi, R. felis | Trunk to extremities No eschar | Rat flea, cat flea | Worldwide | |
Scrub typhus | ||||
Scrub typhus (tsutsugamushi disease) | Orientia tsutsugamushi (formerly R. tsutsugamushi) | Trunk to extremities Eschar present | Trombiculid mite larvae (chiggers) | Asia-Pacific area bounded by Japan, Korea, China, India, and northern Australia |
Spotted fever | ||||
R. rickettsii | Extremities to trunk No eschar | Ixodid (hard) ticks, including Dermacentor andersoni (wood tick), principally in the western United States, and D. variabilis (dog tick), principally in the eastern and southern United States | Western Hemisphere, including most of the United States (except Maine, Hawaii, and Alaska); Central and South America | |
R. sibirica | Trunk, extremities, face Multiple eschars present | Ixodid ticks | Central Asia, Siberia, Mongolia, China | |
Queensland tick typhus | R. australis | Trunk, extremities, face Eschar present | Ixodid ticks | Australia |
African tick typhus (African tick bite fever) | R. africae | Multiple eschars on extremities at the sites of the tick bites | Ixodid ticks | Sub-Saharan Africa, West Indies |
Mediterranean spotted fever (boutonneuse fever)* | R. conorii | Trunk, extremities, face Eschar present | Rhipicephalus sanguineus (brown dog tick) | Africa; India; southern Europe; the Middle East adjacent to the Mediterranean, Black, and Caspian Seas |
R. akari | Trunk, extremities, face Eschar present | Mites | United States, Russia, Korea, Africa | |
R. parkeri rickettsiosis | R. parkeri | Eschar present | Gulf Coast tick (Amblyomma maculatum) | Southern United States, South America |
Pacific Coast tick fever | R. philipii (364D) | Eschar present Mild disease | Pacific Coast tick (Dermacentor occidentalis) | California |
Monocytic ehrlichiosis | Ehrlichia chaffeensis | Uncommon but more common among children No eschar | Ticks (A. americanum, also known as the lone star tick) | Southeastern and south central United States |
Granulocytic anaplasmosis | Anaplasma phagocytophilum | None No eschar | Ticks (Ixodes scapularisin the eastern and Midwest United States, I. pacificus in the western United States, possibly I. ricinus in Europe) | In the United States, the Northeast, mid-Atlantic, upper Midwest, and West Coast; Europe |
Q Fever | ||||
Coxiella burnetii | Rare but more common among children No eschar | No vector needed | Worldwide | |
* Often known by the area in which it occurs (eg, Indian tick typhus, Marseilles fever). | ||||
Symptoms and Signs of Rickettsial Infections
Rickettsiae multiply at the site of arthropod attachment and often produce a local lesion (eschar). They penetrate the skin or mucous membranes; some (R. rickettsii) multiply in the endothelial cells of small blood vessels, causing vasculitis, and others replicate in white blood cells (Ehrlichia species in monocytes, Anaplasma species in granulocytes).
Symptoms usually include sudden-onset fever with severe headache, malaise, prostration, and, in most cases, a characteristic rash.
Regional lymphadenopathy is common with infection by Orientia species or members of the spotted fever group (except for R. rickettsii).
The endovasculitis of R. rickettsii causes a petechial rash (due to focal areas of hemorrhage), encephalitic signs, and gangrene of skin and tissues.
Patients seriously ill with a rickettsial disease of the typhus or spotted fever group may have ecchymotic skin necrosis, edema (due to increased vascular permeability), digital gangrene, circulatory collapse, shock, oliguria, anuria, azotemia, anemia, hyponatremia, hypochloremia, delirium, and coma.
Diagnosis of Rickettsial and Related Infections
History and physical examination
Biopsy of rash with fluorescent antibody staining to detect organisms
Acute and convalescent serologic testing (serologic testing not useful acutely)
Polymerase chain reaction (PCR)
Differentiating rickettsial from other infections
Rickettsial and related diseases must be differentiated from other acute infections, primarily meningococcemia, rubeola, and rubella. A history of louse or flea contact, tick bite, or presence in a known endemic area is helpful, but such history is often absent. Clinicians should specifically ask about travel to an endemic region within the incubation period of the disease.
Clinical features may help distinguish diseases:
Meningococcemia: The rash may be pink, macular, maculopapular, or petechial in the subacute form and petechially confluent or ecchymotic in the fulminant form. The rash develops rapidly in acute meningococcal disease and, when ecchymotic, is usually tender when palpated.
Rubeola: The rash begins on the face, spreads to the trunk and arms, and soon becomes confluent.
Rubella: The rash usually remains discrete. Postauricular lymph node enlargement and lack of toxicity suggest rubella.


Fulminant meningococcemia initially causes petechiae, which become confluent and rapidly progress to ecchymoses.
Photo courtesy of Mr. Gust via the Public Health Image Library of the Centers for Disease Control and Prevention.


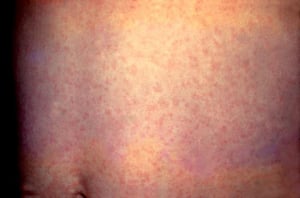
Measles (rubeola) manifests as a diffuse macular rash that becomes confluent.
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.

Rubella manifests as a diffuse rash comprising discrete, pinpoint macules that do not coalesce.
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
Fulminant meningococcemia initially causes petechiae, which become confluent and rapidly progress to ecchymoses.
Photo courtesy of Mr. Gust via the Public Health Image Library of the Centers for Disease Control and Prevention.
Measles (rubeola) manifests as a diffuse macular rash that becomes confluent.
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
Rubella manifests as a diffuse rash comprising discrete, pinpoint macules that do not coalesce.
Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.
Differentiating among rickettsial diseases
Rickettsial diseases must also be differentiated from each other. Clinical features allow some differentiation, but overlap is considerable:
Rocky Mountain spotted fever (RMSF): The rash usually appears on or about the fourth febrile day and appears as blanching macules, initially on the wrists and ankles. Then the rash spreads to the rest of the extremities and gradually becomes petechial as it spreads to the trunk, palms, and soles over several days. Some patients with RMSF never develop a rash. Vasculitis often develops; it may affect the skin, subcutaneous tissues, central nervous system, lungs, heart, kidneys, liver, or spleen.
Epidemic typhus: The rash usually appears initially in the axillary folds and on the trunk. Later, it spreads peripherally, rarely involving the palms, soles, and face. Severe physiologic and pathologic abnormalities similar to those of RMSF occur.
Murine typhus: The rash is nonpurpuric, nonconfluent, and less extensive, and renal and vascular complications are uncommon.
Scrub typhus: Manifestations are similar to those of RMSF and epidemic typhus. However, scrub typhus occurs in different geographic areas, and frequently, an eschar develops with satellite adenopathy.
Rickettsialpox: This disease is mild, and the rash, in the form of vesicles with surrounding erythema, is sparse and may resemble varicella.
African tick typhus (African tick bite fever) due to R. africae: Symptoms are similar to those of other rickettsial diseases. The rash is characterized by multiple black eschars on the distal extremities with regional adenopathy.


Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.

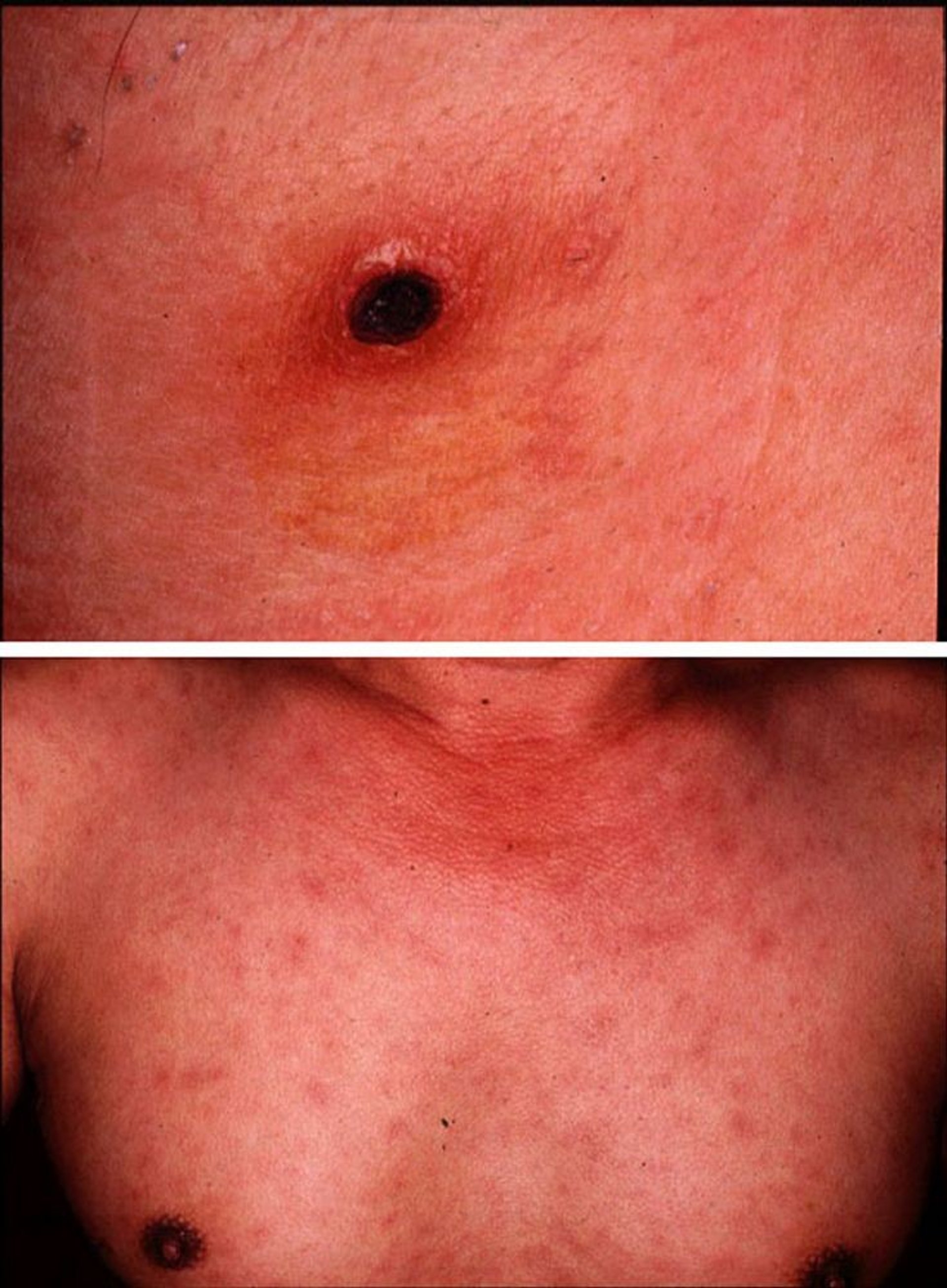
Images courtesy of Yoshiki Taniguchi, MD. From Taniguchi, Y: Eschar, fever, and rash in a 43-year-old man. Dermatology Online Journal 3(2), 1997.
Testing
Knowledge of residence and recent travel often helps in diagnosis because many rickettsiae are localized to certain geographic areas. However, testing is usually required for a definitive diagnosis.
The most useful tests for R. rickettsii are indirect immunofluorescence assay (IFA) and polymerase chain reaction (PCR) of a biopsy specimen of the rash. Culture is difficult and not clinically useful. For Ehrlichia species, PCR of blood is the best test. Serologic tests are not useful for acute diagnosis because they usually become positive only during convalescence.
Treatment of Rickettsial and Related Infections
Tetracyclines
Because diagnostic tests can take time and may be insensitive, antibiotics are usually begun presumptively to prevent significant deterioration, death, and prolonged recovery.
Tetracyclines are first-line treatment: doxycycline until the patient improves, has been afebrile for 24 to 48 hours, and has received treatment for at least 7 days. IV preparations are used in patients too ill to take oral medications. Although some tetracyclines can cause tooth staining in children < 8 years of age, the are first-line treatment: doxycycline until the patient improves, has been afebrile for 24 to 48 hours, and has received treatment for at least 7 days. IV preparations are used in patients too ill to take oral medications. Although some tetracyclines can cause tooth staining in children < 8 years of age, theCenters for Disease Control and Prevention (CDC) and others found that short courses of doxycycline (5 to 10 days, as used for rickettsial disease) can be used in children without causing tooth staining or weakening of tooth enamel (1). Doxycycline for rickettsial disease in children of all ages is recommended by the American Academy of Pediatrics and other experts (see ). Doxycycline for rickettsial disease in children of all ages is recommended by the American Academy of Pediatrics and other experts (seeThe American Academy of Pediatrics Red Book). For patients who do not tolerate doxycycline, desensitization is recommended.). For patients who do not tolerate doxycycline, desensitization is recommended.
ChloramphenicolChloramphenicol is second-line treatment when doxycycline cannot be used. Oral is second-line treatment when doxycycline cannot be used. Oralchloramphenicol is not available in the United States, and IM administration is not effective. Chloramphenicol can cause adverse hematologic effects, which require monitoring of blood indices.
Both medications are rickettsiostatic, not rickettsicidal.
Ciprofloxacin and other fluoroquinolonesCiprofloxacin and other fluoroquinolones are effective in vitro against certain rickettsiae, but very little clinical experience supports the use of fluoroquinolones for RMSF.
Because severely ill patients with RMSF or epidemic typhus may have a marked increase in capillary permeability in later stages, IV fluids should be given cautiously to maintain blood pressure while avoiding worsening pulmonary and cerebral edema.
Treatment reference
1. Todd SR, Dahlgren FS, Traeger MS, et al: No visible dental staining in children treated with doxycycline for suspected Rocky Mountain Spotted Fever. J Pediatr 166(5):1246-51, 2015. doi: 10.1016/j.jpeds.2015.02.015
Key Points
Rickettsial diseases and related diseases (anaplasmosis, ehrlichiosis, Q fever, scrub typhus) are caused by a group of gram-negative, obligately intracellular coccobacilli; all, except for Coxiella burnetii, have an arthropod vector.
Rickettsial diseases cause fever and, depending on the disease, sometimes a local lesion (eschar), petechial rash, regional lymphadenopathy, encephalitic signs, vasculitis, gangrene of skin and tissues, organ dysfunction, and vascular collapse.
Distinguish rickettsial and related diseases from other acute infections and from each other based on history, typical examination findings, and results of tests (eg, biopsy with indirect immunofluorescence assay, serologic tests, PCR).
Treat with antibiotics presumptively, without waiting for diagnostic test results, to prevent significant deterioration, death, and prolonged recovery.
First-line treatment is with doxycycline.First-line treatment is with doxycycline.







