


Scrub typhus is a mite-borne disease caused by Orientia tsutsugamushi (formerly Rickettsia tsutsugamushi). Symptoms are fever, a primary lesion, a macular rash, and lymphadenopathy.
Topic Resources

(See also Overview of Rickettsial and Related Infections.)
Scrub typhus is related to rickettsial diseases.
O. tsutsugamushi is transmitted by trombiculid mite larvae (chiggers), which feed on forest and rural rodents, including rats, voles, and field mice. Human infection also follows a chigger bite. The mites are both the vector and the natural reservoir for O. tsutsugamushi.
Scrub typhus is endemic in an area of Asia-Pacific bounded by Japan, Korea, China, India, and northern Australia.
Symptoms and Signs of Scrub Typhus
After an incubation period of 6 to 21 days (mean 10 to 12 days), symptoms of scrub typhus start suddenly and include fever, chills, headache, and generalized lymphadenopathy. At onset of fever, an eschar often develops at the site of the chigger bite. The typical lesion of scrub typhus begins as a red, indurated lesion about 1 cm in diameter; it eventually vesiculates, ruptures, and becomes covered with a black scab. The capacity of different strains of O. tsutsugamushi to result in an eschar varies, and an eschar is easier to detect in light-skinned people. Regional lymph nodes enlarge.
Fever rises during the first week, often to 40 to 40.5° C. Headache is severe and common, as is conjunctival injection. A macular rash develops on the trunk during the 5th to 8th day of fever, often extending to the arms and legs. It may disappear rapidly or become maculopapular and intensely colored. Cough is present during the first week of fever, and pneumonitis may develop during the second week.
In severe cases, pulse rate increases; blood pressure drops; and delirium, stupor, and muscular twitching develop. Splenomegaly may be present, and interstitial myocarditis is more common than in other rickettsial diseases. In untreated patients, high fever may persist ≥ 2 weeks, then falls gradually over several days. With therapy, defervescence usually begins within 36 hours. Recovery is prompt and uneventful.

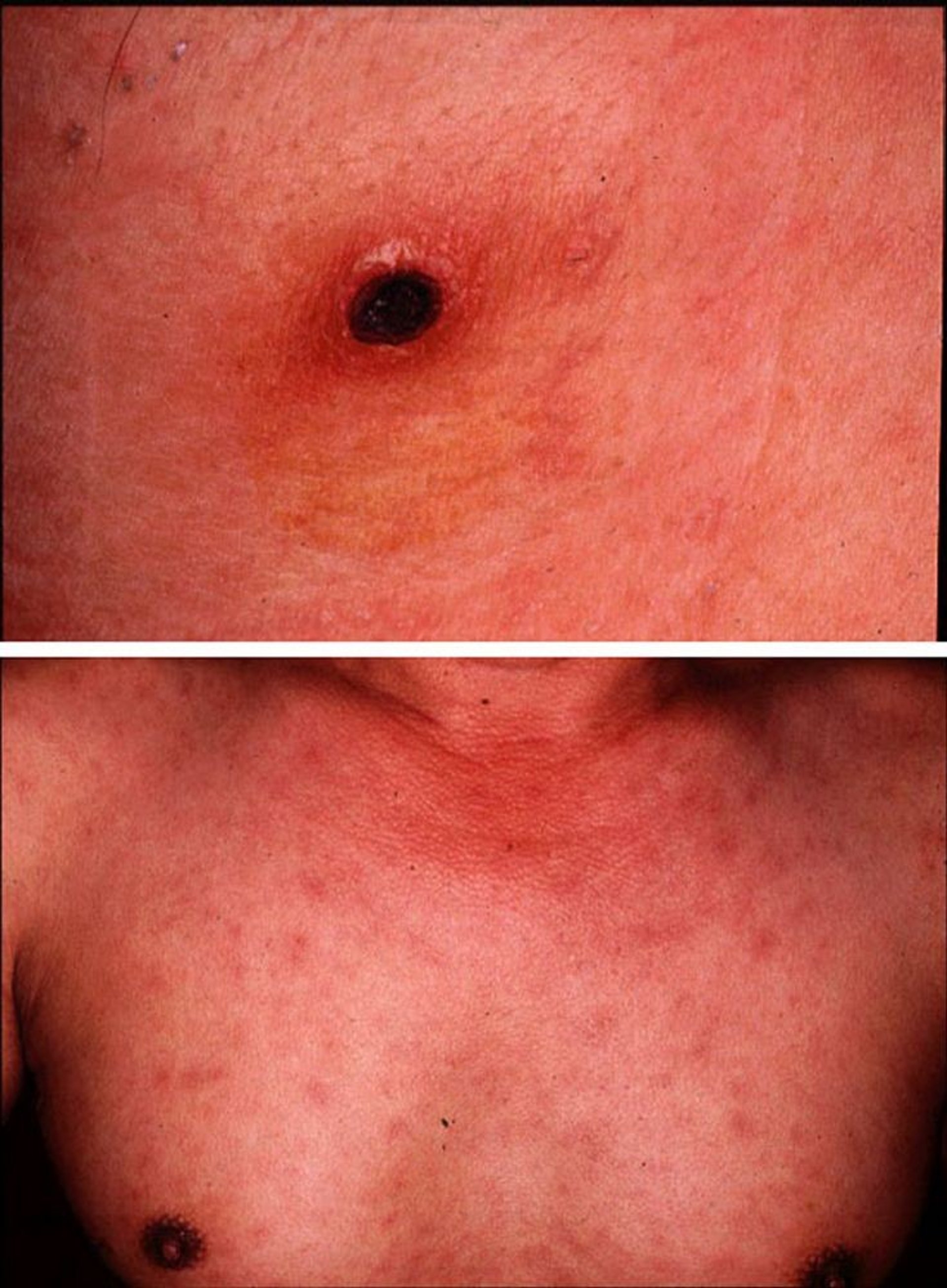
Images courtesy of Yoshiki Taniguchi, MD. From Taniguchi, Y: Eschar, fever, and rash in a 43-year-old man. Dermatology Online Journal 3(2), 1997.
Diagnosis of Scrub Typhus
History and physical examination
Biopsy of rash with fluorescent antibody staining to detect organisms
Acute and convalescent serologic testing (serologic testing not useful acutely)
Polymerase chain reaction (PCR)
Manifestations of scrub typhus are similar to those of Rocky Mountain spotted fever and epidemic typhus. However, scrub typhus occurs in different geographic areas (Asia-Pacific area bounded by Japan, Korea, China, India, and northern Australia), and frequently, an eschar develops with satellite adenopathy.
For details, see Diagnosis of Rickettsial and Related Infections.
Treatment of Scrub Typhus
DoxycyclineDoxycycline
Antibiotics are most effective if given soon after symptoms begin.
Primary treatment of scrub typhus is doxycycline until the patient improves, has been afebrile for 48 hours, and has received treatment for at least 7 days. Primary treatment of scrub typhus is doxycycline until the patient improves, has been afebrile for 48 hours, and has received treatment for at least 7 days.
Although some tetracyclines can cause tooth staining in children < 8 years of age, the Centers for Disease Control and Prevention (CDC) advises that a course of doxycycline is warranted (Although some tetracyclines can cause tooth staining in children doxycycline is warranted (1), given for 5 days for mild illness and for 10 days for high-risk children. Research indicates that short courses of doxycycline (5 to 10 days, as used for rickettsial disease) can be used in children without causing tooth staining or weakening of tooth enamel (), given for 5 days for mild illness and for 10 days for high-risk children. Research indicates that short courses of doxycycline (5 to 10 days, as used for rickettsial disease) can be used in children without causing tooth staining or weakening of tooth enamel (2). Pregnant women may be given trimethoprim/sulfamethoxazole, but not beyond 32 weeks gestation.). Pregnant women may be given trimethoprim/sulfamethoxazole, but not beyond 32 weeks gestation.
For pregnant women and patients with severe doxycycline allergy, azithromycin has been shown to be a safe and effective alternative to doxycycline (allergy, azithromycin has been shown to be a safe and effective alternative to doxycycline (3).
Chloramphenicol is an alternative treatment. Oral Chloramphenicol is an alternative treatment. Oralchloramphenicol is not available in the United States, and its use can cause adverse hematologic effects, which requires monitoring of blood indices.
Treatment references
1. Centers for Disease Control and Prevention: Information for Healthcare Providers, Typhus Fevers
2. Todd SR, Dahlgren FS, Traeger MS, et al: No visible dental staining in children treated with doxycycline for suspected Rocky Mountain Spotted Fever. : No visible dental staining in children treated with doxycycline for suspected Rocky Mountain Spotted Fever.J Pediatr 166(5):1246-51, 2015. doi: 10.1016/j.jpeds.2015.02.015
3. Lee SC, Cheng YJ, Lin CH, et al: Comparative effectiveness of azithromycin for treating scrub typhus: A PRISMA-compliant systematic review and meta-analysis. : Comparative effectiveness of azithromycin for treating scrub typhus: A PRISMA-compliant systematic review and meta-analysis.Medicine (Baltimore) 96(36):e7992, 2017. doi: 10.1097/MD.0000000000007992
Prevention of Scrub Typhus
Eliminating or decreasing mite populations by clearing brush and spraying infested areas with residual insecticides helps to prevent scrub typhus. Insect repellents (eg, diethyltoluamide [DEET]) should be used when exposure is likely.Eliminating or decreasing mite populations by clearing brush and spraying infested areas with residual insecticides helps to prevent scrub typhus. Insect repellents (eg, diethyltoluamide [DEET]) should be used when exposure is likely.
Key Points
Scrub typhus, endemic in Asia-Pacific, is transmitted by the bite of chiggers (mite larvae).
Fever (often accompanied by an eschar at the bite site), chills, severe headache, and generalized lymphadenopathy start suddenly; a rash develops and spreads.
Treat with doxycycline, which results in rapid improvement even in severe cases.Treat with doxycycline, which results in rapid improvement even in severe cases.







