



- Overview of Vasculitis
- Behçet Disease
- Cutaneous Vasculitis
- Eosinophilic Granulomatosis with Polyangiitis (EGPA)
- Giant Cell Arteritis
- Granulomatosis with Polyangiitis (GPA)
- Immunoglobulin A–Associated Vasculitis (IgAV)
- Microscopic Polyangiitis (MPA)
- Polyarteritis Nodosa (PAN)
- Polymyalgia Rheumatica
- Takayasu Arteritis
Takayasu arteritis is an inflammatory disease affecting the aorta, its branches, and pulmonary arteries. It occurs predominantly in young females. Etiology is unknown. Vascular inflammation may cause arterial stenosis, occlusion, dilation, or aneurysms. Patients may present with asymmetric pulses or unequal blood pressure measurements between limbs (eg, between limbs on opposite sides or between the arm and leg on the same side), limb claudication, symptoms of decreased cerebral perfusion (eg, transient visual disturbances, transient ischemic attacks, strokes), and hypertension or its complications. Diagnosis is by aortic arteriography or magnetic resonance angiography. Treatment is with corticosteroids and other immunosuppressants and, for organ-threatening ischemia, vascular interventions such as bypass surgery.



(See also Overview of Vasculitis.)
Takayasu arteritis is rare. It is most common in Asia but occurs worldwide. Female:male ratio is 8:1, and age at onset is typically 15 to 30 years. In North America, annual incidence is estimated to be 2.6 cases/million (1).
General reference
1. Hall S, Barr W, Lie JT, Stanson AW, Kazmier FJ, Hunder GG. Takayasu arteritis. A study of 32 North American patients. Medicine (Baltimore) 64(2):89-99, 1985.
Etiology of Takayasu Arteritis
The cause of Takayasu arteritis is unknown. Cell-mediated immune mechanisms may be involved.
Pathophysiology of Takayasu Arteritis
Takayasu arteritis affects primarily large elastic arteries. The most commonly affected are
Innominate and subclavian arteries
Aorta (mainly the ascending aorta and the arch)
Common carotid arteries
Renal arteries
Most patients have stenoses or occlusions. Aneurysms occur in approximately one-third of patients. Usually, the wall of the aorta or its branches thickens irregularly, with intimal wrinkling. When the aortic arch is affected, orifices of the major arteries emerging from the aorta may be markedly narrowed or even obliterated by intimal thickening. In one-half of patients, pulmonary arteries are also affected. Sometimes the medium-sized branches of the pulmonary arteries are involved.
Histologically, early changes consist of adventitial mononuclear infiltrate with perivascular cuffing of the vasa vasorum. Later, intense mononuclear inflammation of the media may occur, sometimes accompanied by granulomatous changes, giant cells, and patchy necrosis of the media. Morphologic changes may be indistinguishable from those of giant cell arteritis. Panarteritic inflammatory infiltrates cause marked thickening of the affected artery and subsequent luminal narrowing and occlusion.
Symptoms and Signs of Takayasu Arteritis
Most patients present with only focal symptoms that reflect hypoperfusion of the affected organ or limb.
Approximately 50% of patients report constitutional symptoms such as fever, malaise, night sweats, weight loss, fatigue, and/or arthralgias.
Repetitive arm movements and sustained arm elevation may cause pain and fatigue. Arterial pulses in arms and legs may be absent or diminished and asymmetric. Extremities may have findings of ischemia (eg, coolness, leg claudication). Bruits are often audible over the subclavian arteries (above the clavicle in the supraclavicular fossa), brachial arteries, carotid arteries, abdominal aorta, or femoral arteries. Reduced blood pressure in one or both arms is common.
Involvement of the carotid and vertebral arteries results in reduced cerebral blood flow manifested by dizziness, syncope, orthostatic hypotension, headaches, transient visual disturbances, transient ischemic attacks, or strokes.
Stenotic lesions in a subclavian artery near the origin of a patent vertebral artery can cause posterior circulation ischemic neurologic symptoms or syncope when the arm is used (called subclavian steal syndrome). The mechanisms are retrograde flow through the vertebral artery to supply the subclavian artery distal to the stenosis and vasodilation of the arterial bed in the upper limb during exercise.
Angina pectoris or myocardial infarction may result from narrowing of the coronary artery orifice due to aortitis or coronary arteritis. Aortic regurgitation may occur if the ascending aorta is markedly dilated. Heart failure can develop.
Obstruction of the descending thoracic aorta sometimes causes signs of aortic coarctation (eg, hypertension, headache, leg claudication). Renovascular hypertension may develop if the abdominal aorta or renal arteries are narrowed. Intermittent arm or leg claudication can develop.
Pulmonary arteries are affected, sometimes causing pulmonary hypertension. Involvement of the medium-sized branches of the pulmonary arteries can cause pulmonary infarcts. Because Takayasu arteritis is chronic, collateral circulation can develop. Thus, ischemic ulcerations or gangrene due to obstruction of the arteries to the extremities is rare.
Diagnosis of Takayasu Arteritis
Imaging of the aorta and its branches with magnetic resonance angiography or CT angiography
The diagnosis of Takayasu arteritis is suspected when symptoms suggest ischemia of organs supplied by the aorta or its branches or when peripheral pulses are decreased or absent in patients at low risk of atherosclerosis and other aortic disorders, especially in young females. In these patients, arterial bruits and right/left or upper extremity/lower extremity discrepancies in pulses or in blood pressure (BP) also suggest the diagnosis.
Magnetic resonance angiography or CT angiography are be used to evaluate all branches of the aorta. Characteristic findings include stenosis, occlusion, irregularities in arterial lumens, poststenotic dilation, collateral arteries around obstructed vessels, and aneurysms.

© 2017 Elliot K. Fishman, MD.
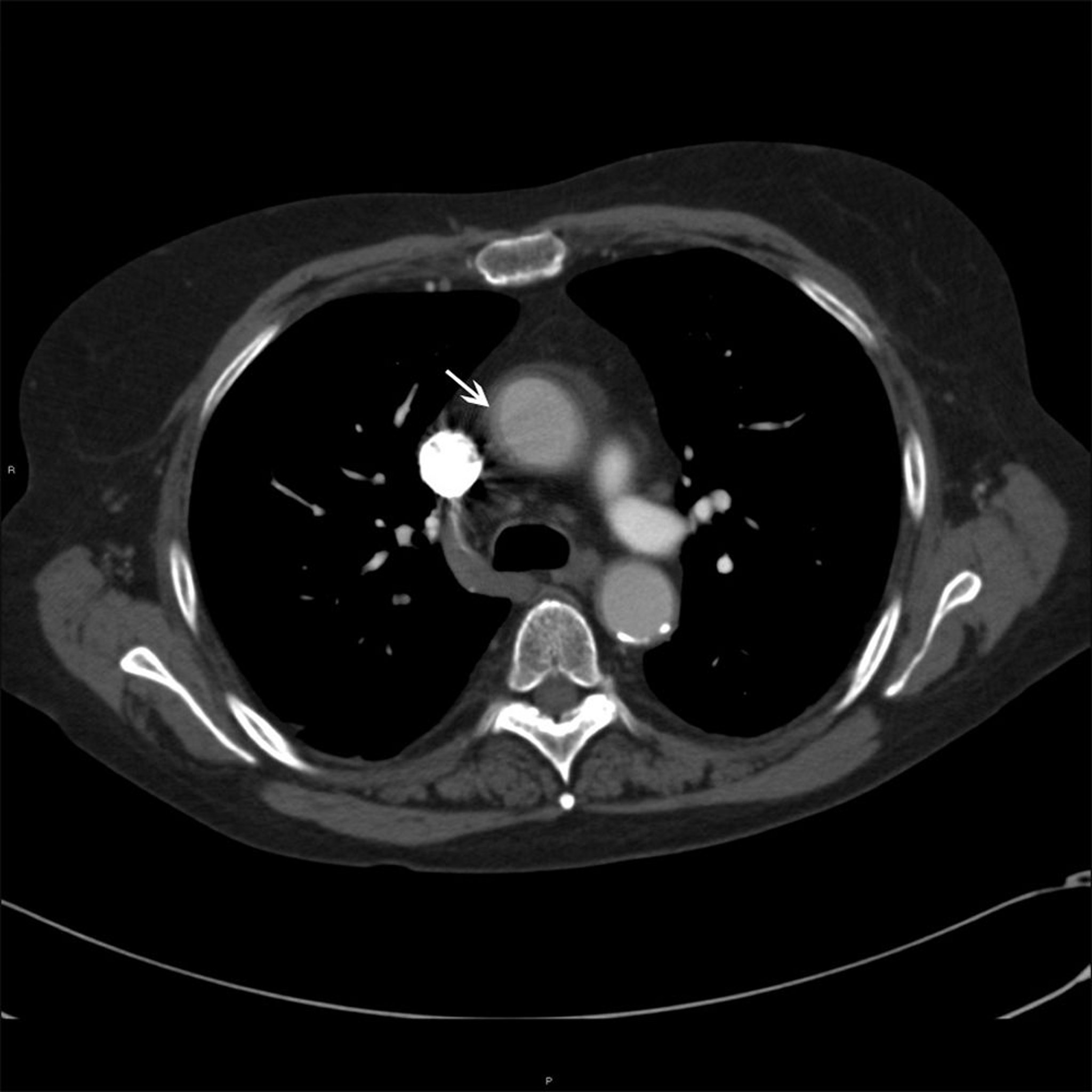
© 2017 Elliot K. Fishman, MD.
BP is measured in all extremities. However, accurate measurement of BP can be difficult. If both subclavian arteries are severely affected, systemic BP can be accurately measured only in the legs. If the disorder affects both subclavian arteries and patients have coarctation of the descending aorta and/or involvement of both iliac or femoral arteries, BP cannot be accurately measured in any limb. Then, central arterial pressure must be measured via angiography to detect occult hypertension, which can cause complications.
Other clues to occult hypertension can be funduscopic signs of hypertensive retinopathy and/or echocardiographic signs of concentric left ventricular hypertrophy. When severe hypertension is not recognized, complications can be confused with signs of vasculitis causing organ ischemia.
Laboratory test results are nonspecific and not helpful in diagnosis. Common findings include anemia of chronic disease, elevated platelet levels, occasionally elevated white blood cell counts, and elevated erythrocyte sedimentation rate and C-reactive protein.
The following are indicators of disease activity in Takayasu arteritis:
Symptoms and signs: New systemic symptoms (eg, fever, fatigue, weight loss, anorexia, night sweats), symptoms suggesting vasculitis involving new arterial territories (eg, claudication), new bruits, and/or new changes in BP measurements
Laboratory tests: Evidence of inflammation detected by blood tests (although markers of inflammation may be normal in active arteritis)
Imaging studies: Development of stenosis or aneurysms in previously unaffected arteries (assessed with periodic imaging [usually magnetic resonance angiography])
However, Takayasu arteritis can progress silently even when clinical and laboratory studies suggest complete remission. Therefore, periodic imaging of the aorta and large arteries is mandatory. BP should be measured regularly in an unaffected limb.
Imaging Tests Used in Takayasu Arteritis
Test | Uses | Comments |
|---|---|---|
Conventional angiography (aortic arteriography) | Preferred when a surgical intervention is being considered and when proximal aortic blood pressure cannot be measured any other way | Provides descriptive anatomic information about the vascular lumen |
Magnetic resonance angiography of the aorta and large arteries | Avoids the risk of arterial puncture and of exposure to iodinated contrast or radiation Usually the test of choice in young females, who are less likely to have extensive atherosclerosis and are more susceptible to radiation-induced cancer | Provides some information about arterial wall anatomy Does not provide sufficient information about distal aortic branches because the resolution is too low Provides little information about the content of arterial plaque, making discrimination between vasculitic and atherosclerotic disease difficult |
CT angiography | Used to generally survey the aorta and its proximal branches when magnetic resonance angiography is contraindicated or is not available | Can characterize aortic calcification May provide information about arterial wall thickness Unclear whether it is useful in monitoring disease activity |
Positron emission tomography with fluorine-18 (18F) deoxyglucose | Used to assess regional differences in glucose metabolism and may help locate regions of inflammation (because inflammatory cells take up more glucose) | Does not provide information about changes in lumen size |
Disorders that mimic Takayasu arteritis must be excluded. They include
Inherited noninflammatory connective tissue disorders (eg, Ehlers-Danlos syndrome or Marfan syndrome)
Vascular infections (tuberculous, fungal, or syphilitic)
Fibromuscular dysplasias
Disorders causing arterial thrombosis (eg, hypercoagulable states)
Idiopathic inflammatory conditions (eg, ankylosing spondylitis with aortitis, rheumatoid arthritis, Cogan syndrome or Behçet syndrome, Kawasaki disease, sarcoidosis)
All of these disorders can affect large vessels.
Treatment of Takayasu Arteritis
Corticosteroids
Other immunosuppressants
Antihypertensives and/or vascular interventions as needed
Medications
Corticosteroids are the cornerstone of Takayasu arteritis treatment (1). A second immunosuppressant is frequently considered at onset of treatment with corticosteroid, especially in severe cases.
The optimal dose of corticosteroids, tapering schedule, and length of treatment have not been determined. Prednisone is usually started at 1 mg/kg orally once a day, and then tapered slowly over several months. The optimal dose of corticosteroids, tapering schedule, and length of treatment have not been determined. Prednisone is usually started at 1 mg/kg orally once a day, and then tapered slowly over several months.
Methotrexate, azathioprine, mycophenolate mofetil, tumor necrosis factor (TNF) inhibitors (eg, infliximab), tocilizumab, and less commonly cyclophosphamide have been used successfully in combination with corticosteroids (Methotrexate, azathioprine, mycophenolate mofetil, tumor necrosis factor (TNF) inhibitors (eg, infliximab), tocilizumab, and less commonly cyclophosphamide have been used successfully in combination with corticosteroids (2, 3). Methotrexate is started at a dose of 15 mg once a week, which is increased up to 25 mg/week. Mycophenolate mofetil can also be tried. Cyclophosphamide should be considered in patients with coronary vasculitis or other serious complications thought to be due to active arteritis.
An antiplatelet agent (eg, aspirin 325 mg orally once a day) is frequently used because platelet-mediated occlusion may play a role in the progression of ischemia. Hypertension should be treated aggressively; angiotensin-converting enzyme (ACE) inhibitors may be effective.An antiplatelet agent (eg, aspirin 325 mg orally once a day) is frequently used because platelet-mediated occlusion may play a role in the progression of ischemia. Hypertension should be treated aggressively; angiotensin-converting enzyme (ACE) inhibitors may be effective.
Procedures
Vascular intervention, usually a bypass procedure, may be needed to reestablish blood flow to ischemic tissues if pharmacotherapy is ineffective. Indications include the following:
Aortic insufficiency
Coronary artery stenosis causing symptomatic coronary artery disease or ischemic cardiomyopathy
Dissection of enlarged aortic aneurysm
Severe hypertension secondary to renal artery stenosis that is refractory to medical management
Limb ischemia that interferes with daily activities
Brain ischemia
Coarctation of the aorta
Inability to measure blood pressure accurately (in any limb)
Bypass grafting preferably with an autologous graft has the best patency rates. The anastomosis should be made at disease-free sites of the affected arteries to help prevent aneurysm formation and occlusion; vessels that are likely to be involved in the future, such as the subclavian arteries, are usually not used for revascularization.
Percutaneous transluminal coronary angioplasty (PTCA) has few risks and may be effective for short lesions. But long-term restenosis rates seem much higher than those with bypass grafting. Vascular stenting is usually not recommended because the restenosis rate is high.
For aortic regurgitation, valvular surgery with aortic root replacement may be necessary.
Treatment references
1. Maz M, Chung SA, Abril A, et al: 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Giant Cell Arteritis and Takayasu Arteritis. Arthritis Rheumatol 73(8):1349–1365, 2021. doi:10.1002/art.41774
2. Mekinian A, Neel A, Sibilia J, et al: Efficacy and tolerance of infliximab in refractory Takayasu arteritis: French multicentre study. Rheumatology 51:882–886, 2012. doi: 10.1093/rheumatology/ker380
3. Mekinian A, Comarmond C, Resche-Rigon A, et al: Efficacy of biological-targeted treatments in Takayasu arteritis: Multicenter, retrospective study of 49 patients. Circulation 132:1693–1700, 2015. doi: 10.1161/CIRCULATIONAHA.114.014321
Prognosis for Takayasu Arteritis
For 20% of patients, the course is monophasic. For the rest, the course is relapsing and remitting or chronic and progressive. Even when symptoms and laboratory abnormalities suggest quiescence, new vascular lesions occur and are evident on imaging studies. A progressive course and the presence of complications (eg, hypertension, aortic regurgitation, heart failure, aneurysms) predict a less favorable prognosis.
Key Points
Takayasu arteritis is a rare arteritis affecting mostly women aged 15 to 30 years.
Involvement of the aorta, pulmonary artery, and their branches can cause manifestations such as asymmetric pulses or blood pressure measurements, limb claudication, symptoms of decreased cerebral perfusion (eg, transient visual disturbances, transient ischemic attacks, strokes), and hypertension (systemic and pulmonary) or its complications.
Diagnose by magnetic resonance angiography or sometimes CT or conventional angiography.
Treat with corticosteroids, other immunosuppressants, aspirin, and, when indicated, antihypertensive medications.Treat with corticosteroids, other immunosuppressants, aspirin, and, when indicated, antihypertensive medications.
Refer patients for vascular intervention if, despite pharmacotherapy, they have severe vascular complications (eg, end-organ ischemia; aortic dissection, coarctation, or insufficiency).







