



- Overview of Neuro-ophthalmologic and Cranial Nerve Disorders
- Conjugate Gaze Palsies
- Internuclear Ophthalmoplegia
- Third Cranial (Oculomotor) Nerve Disorders
- Fourth Cranial (Trochlear) Nerve Palsy
- Sixth Cranial (Abducens) Nerve Palsy
- Trigeminal Neuralgia
- Hemifacial Spasm
- Facial Nerve Palsy
- Glossopharyngeal Neuralgia
Facial nerve (7th cranial nerve) palsy is often idiopathic (formerly called Bell palsy). Idiopathic facial nerve palsy is sudden, unilateral peripheral facial nerve palsy. Symptoms of facial nerve palsy are hemifacial paresis of the upper and lower face. Tests (eg, chest x-ray, serum angiotensin-converting enzyme [ACE] level, tests for Lyme disease, serum glucose) are done to diagnose treatable causes. Treatment may include lubrication of the eye, intermittent use of an eye patch, and, for idiopathic facial nerve palsy, corticosteroids.
Topic Resources

(See also Overview of Neuro-ophthalmologic and Cranial Nerve Disorders.)
Etiology of Facial Nerve Palsy
Historically, Bell palsy was thought to be idiopathic facial nerve (peripheral 7th cranial nerve) palsy. However, facial nerve palsy is now considered a clinical syndrome with its own differential diagnosis, and the term "Bell palsy" is not always considered synonymous with idiopathic facial nerve palsy. About half the cases of facial nerve palsy are idiopathic.
The mechanism for what was previously thought to be idiopathic facial nerve palsy is presumably swelling of the facial nerve due to an immune or viral disorder. Current evidence suggests that common viral causes are
Herpes simplex virus infection (most common)
Herpes zoster (possibly the second most common)
Other viral causes include SARS-CoV-2, coxsackievirus, cytomegalovirus, adenovirus, and the Epstein-Barr, mumps, rubella, and influenza B viruses. The swollen nerve is maximally compressed as it passes through the labyrinthine portion of the facial canal, resulting in ischemia and paresis.
Various other disorders (eg, diabetes, Lyme disease, sarcoidosis) can cause facial nerve palsy. Lyme disease can cause facial nerve palsy that, unlike Bell palsy, may be bilateral. Particularly in people of African-American ancestry, sarcoidosis is a common cause of facial nerve palsy and may be bilateral.
Pathophysiology of Facial Nerve Palsy
The facial muscles are innervated peripherally (infranuclear innervation) by the ipsilateral 7th cranial nerve and centrally (supranuclear innervation) by the contralateral cerebral cortex. Central innervation tends to be bilateral for the upper face (eg, forehead muscles) and unilateral for the lower face. As a result, both central and peripheral lesions tend to paralyze the lower face. However, peripheral lesions (facial nerve palsy) tend to affect the upper face more than central lesions (eg, stroke) do.
Symptoms and Signs of Facial Nerve Palsy
Pain behind the ear often precedes facial paresis in idiopathic facial nerve palsy. Paresis, often with complete paralysis, develops within hours and is usually maximal within 48 to 72 hours.
Patients may report a numb or heavy feeling in the face. The affected side becomes flat and expressionless; the ability to wrinkle the forehead, blink, and grimace is limited or absent. In severe cases, the palpebral fissure widens and the eye does not close, often irritating the conjunctiva and drying the cornea.

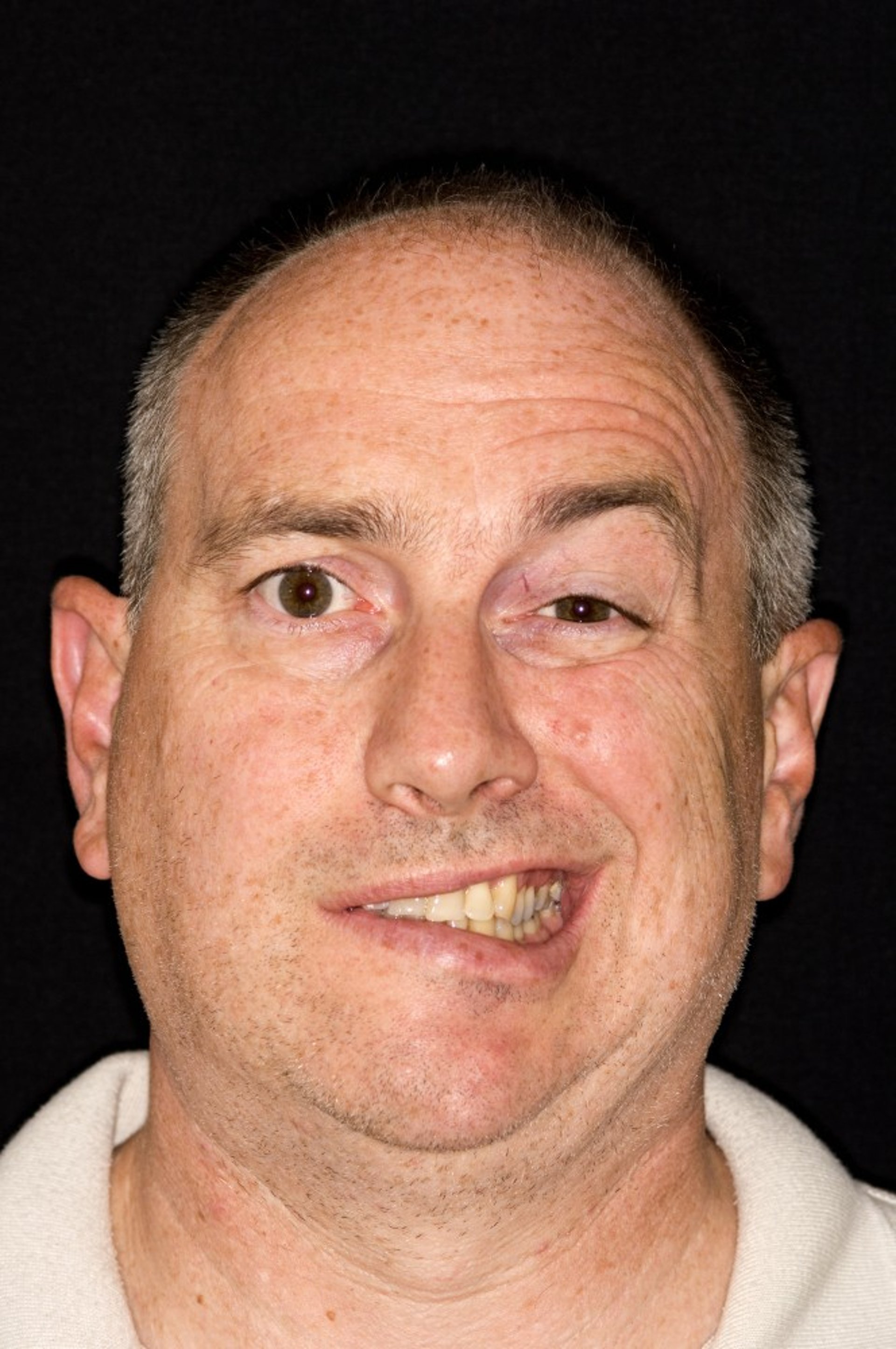
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Sensory examination is normal, but the external auditory canal and a small patch behind the ear (over the mastoid) may be painful to the touch. If the nerve lesion is proximal to the geniculate ganglion, salivation, taste, and lacrimation may be impaired, and hyperacusis may be present.
Diagnosis of Facial Nerve Palsy
Clinical evaluation
Chest x-ray or CT and serum angiotensin-converting enzyme (ACE) levels to check for sarcoidosis
MRI if onset was gradual or other neurologic deficits are present
Other testing if indicated by clinical findings
Facial nerve palsy is diagnosed based on clinical evaluation. There are no specific diagnostic tests.
Facial nerve palsy can be distinguished from a central facial nerve lesion (eg, due to hemispheric stroke or tumor), which causes weakness primarily of the lower face, sparing the forehead muscle and allowing patients to wrinkle their forehead; also, patients with central lesions can usually furrow their brow and close their eyes tightly.
Usually, clinicians can also distinguish idiopathic facial nerve palsy from other disorders that cause peripheral facial nerve palsies based on their characteristic symptoms and signs; these disorders include the following:
Herpes zoster oticus (geniculate herpes, Ramsay Hunt syndrome)
Petrous bone fractures
Carcinomatous or leukemic nerve invasion
Cerebellopontine angle or glomus jugulare tumors
Also, the other disorders that cause peripheral facial nerve palsy typically develop more slowly than idiopathic facial nerve palsy. Thus, if patients have any other neurologic symptoms or signs or if symptoms developed gradually, MRI should be done.
In idiopathic facial nerve palsy, MRI may show contrast enhancement of the facial nerve at or near the geniculate ganglion or along the entire course of the nerve. However, its enhancement may reflect other causes, such as meningeal tumor. If the paralysis progresses over weeks to months, the likelihood of a tumor (eg, most commonly schwannoma) compressing the facial nerve increases. MRI can also help exclude other structural disorders causing facial nerve palsy. CT, usually negative in Bell palsy, is done if a fracture is suspected or if MRI is not immediately available and stroke is possible.
In addition, acute and convalescent serologic tests for Lyme disease are done if patients have been in a geographic area where ticks and Lyme disease are endemic.
For all patients, a chest x-ray is taken or CT is done and serum ACE is measured to check for sarcoidosis. Blood tests are done to check for diabetes. Viral titers are not helpful.
Treatment of Facial Nerve Palsy
Protection for the cornea
Corticosteroids for idiopathic facial nerve palsy
Corneal drying must be prevented by frequent use of natural tears, isotonic saline, or methylcellulose drops and by intermittent use of tape or a patch to help close the eye, particularly during sleep. Tarsorrhaphy is occasionally required.Corneal drying must be prevented by frequent use of natural tears, isotonic saline, or methylcellulose drops and by intermittent use of tape or a patch to help close the eye, particularly during sleep. Tarsorrhaphy is occasionally required.
In idiopathic facial nerve palsy, corticosteroids, ideally begun within 3 days of symptom onset, result in faster and more complete recovery (1). Prednisone 60 to 80 mg orally once a day is given for 1 week, then decreased gradually over the 2nd week.). Prednisone 60 to 80 mg orally once a day is given for 1 week, then decreased gradually over the 2nd week.
Antiviral drugs effective against herpes simplex virus (eg, valacyclovir 1 g orally 3 times a day for 7 to 10 days, famciclovir 500 mg orally 3 times a day for 5 to 10 days, acyclovir 400 mg orally 5 times a day for 10 days) have been prescribed in addition to corticosteroids, but recent data suggest that antiviral drugs provide no benefit (Antiviral drugs effective against herpes simplex virus (eg, valacyclovir 1 g orally 3 times a day for 7 to 10 days, famciclovir 500 mg orally 3 times a day for 5 to 10 days, acyclovir 400 mg orally 5 times a day for 10 days) have been prescribed in addition to corticosteroids, but recent data suggest that antiviral drugs provide no benefit (1).
Treatment reference
1. Gagyor I, Madhok VB, Daly F, Sullivan F: Antiviral treatment for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev 9 (9):CD001869, 2019. doi: 10.1002/14651858.CD001869.pub9
Prognosis for Facial Nerve Palsy
In idiopathic facial nerve palsy, the extent of nerve damage determines outcome. If some function remains, full recovery typically occurs within several months. Nerve conduction studies and electromyography are done to help predict outcome. The likelihood of complete recovery after total paralysis is 90% if nerve branches in the face retain normal excitability to supramaximal electrical stimulation and is only about 20% if electrical excitability is absent.
Regrowth of nerve fibers may be misdirected, innervating lower facial muscles with periocular fibers and vice versa. The result is contraction of unexpected muscles during voluntary facial movements (synkinesia) or crocodile tears during salivation. Chronic disuse of the facial muscles may lead to contractures.
Key Points
In facial nerve palsy, patients cannot move the upper and lower part of their face on one side; in contrast, central facial nerve lesions (eg, due to stroke) affect primarily the lower face.
Evidence that the mechanism for what was previously thought to be idiopathic facial nerve palsy is increasingly implicating herpes viruses.
Diagnosis is clinical, but if other neurologic symptoms or signs are present or if symptom onset was not clearly acute, do MRI.
If given early, corticosteroids are helpful for idiopathic facial nerve palsy; antivirals probably provide no benefit.







