


OCD is slightly more common among women than men in adulthood and affects about 1 to 2% of the population at any given point in time (1). Mean age of onset for OCD is 19 to 20 years, but about 25% of cases begin by age 14 (see Obsessive-Compulsive Disorder [OCD] and Related Disorders in Children and Adolescents). Up to 30% of people with OCD also have a past or current tic disorder.
General reference
1. Stein DJ, Costa DLC, Lochner C, et al: Obsessive-compulsive disorder. Nat Rev Dis Primers 5(1):52, 2019. doi: 10.1038/s41572-019-0102-3
Symptoms and Signs of OCD
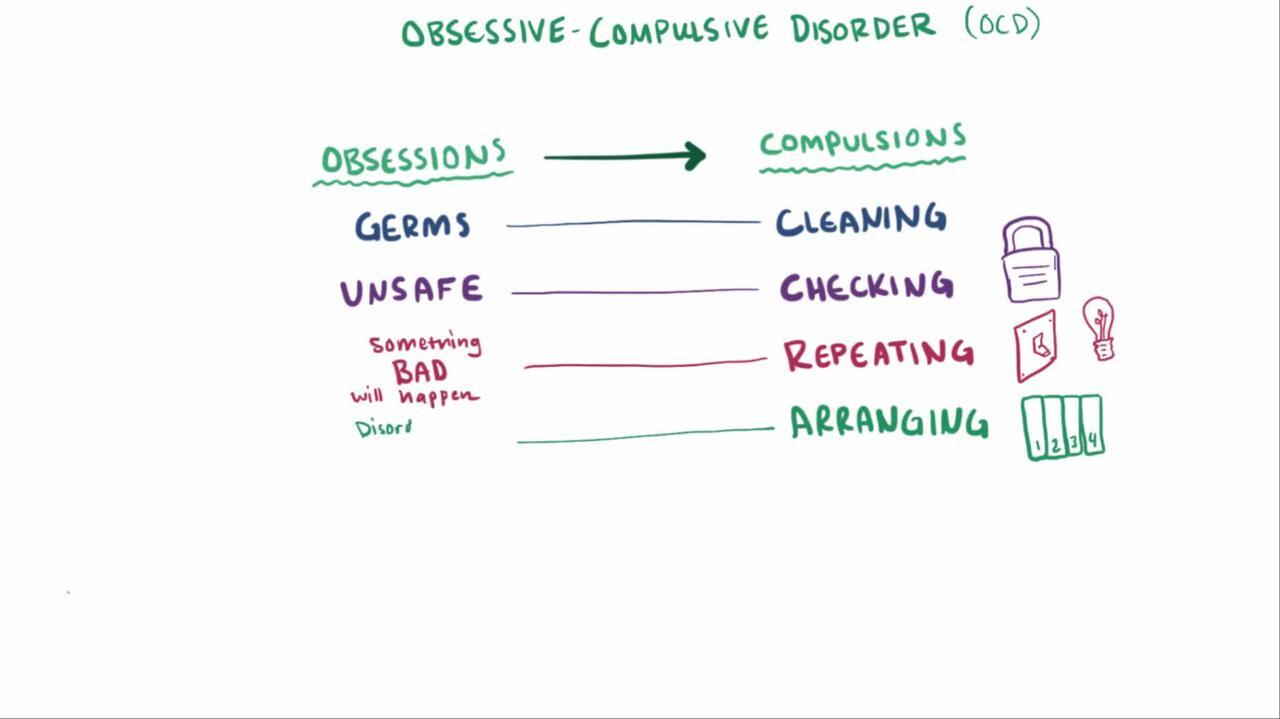
Obsessions are unwanted, intrusive thoughts, urges, or mental images, the presence of which usually causes marked distress or anxiety. The dominant themes of the obsessions include harm (eg, fears of harm to self or others), cleaning or contamination (eg, patients may obsess about becoming contaminated with dirt or germs), forbidden or taboo thoughts (eg, aggressive or sexual obsessions), and the need for symmetry. The obsessions are not pleasurable. Thus, patients usually try to ignore and/or suppress them, or they try to neutralize them by performing a compulsion.
Compulsions (often called rituals) are excessive, repetitive, purposeful behaviors that people feel they must do to prevent or reduce the anxiety caused by their obsessive thoughts or to neutralize their obsessions. Examples are
Washing (eg, handwashing, showering)
Checking (eg, that the stove is turned off, that doors are locked)
Counting (eg, repeating a behavior a certain number of times)
Ordering (eg, arranging tableware or workspace items in a specific pattern)
Most rituals, such as handwashing or checking locks, are observable, but some mental rituals, such as silent repetitive counting or statements muttered under the breath, are not. Typically, the compulsive rituals must be done in a precise way according to rigid rules. The rituals may or may not be connected realistically to the feared event. When connected realistically (eg, showering to avoid being dirty, checking the stove to prevent fire), the compulsions are clearly excessive—eg, showering for hours each day or always checking the stove 30 times before leaving the house. In all cases, the obsessions and/or compulsions must be time-consuming (ie, they take up an 1 hour a day or often much more) or cause patients significant distress or impairment in functioning; at their extreme, obsessions and compulsions may be incapacitating.
The degree of insight varies. Most people with obsessive-compulsive disorder (OCD) recognize to at least some degree that the beliefs underlying their obsessions are not realistic (eg, that they really will not get cancer if they touch an ashtray). However, occasionally, insight is completely lacking (ie, patients are convinced that the beliefs underlying their obsessions are true and that their compulsions are reasonable).
Because people with this disorder may fear embarrassment or stigmatization, they often conceal their obsessions and rituals. The time, distress, or poor functioning associated with the obsessions and compulsions may cause relationships to be disrupted and performance in school or at work to decline.
Many people with OCD have coexisting past or current psychologic disorders, including
Anxiety disorders (76%) (1)
Mood disorders (63%; the most common is major depressive disorder [41%] (2))
Obsessive-compulsive personality disorder (23 to 32%) (3)
Almost 50% of people with OCD have suicidal thoughts at some point, and about 10% attempt suicide (see Suicidal Behavior) (4, 5). Risk of an attempt is increased if people also have major depressive disorder.
Symptoms and signs references
1. Pallanti S, Grassi G, Sarrecchia ED, et al: Obsessive-compulsive disorder comorbidity: Clinical assessment and therapeutic implications. Front Psychiatry 21;2:70, 2011. doi: 10.3389/fpsyt.2011.00070
2. Ruscio AM, Stein DJ, Chiu WT, et al: The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry 15(1):53-63, 2010. doi: 10.1038/mp.2008.94
3. Coles ME, Pinto A, Mancebo MC, et al: OCD with comorbid OCPD: A subtype of OCD? J Psychiatr Res 42(4):289-296, 2008. doi: 10.1016/j.jpsychires.2006.12.009
4. Pellegrini L, Maietti E, Rucci P, et al: Suicide attempts and suicidal ideation in patients with obsessive-compulsive disorder: A systematic review and meta-analysis. J Affect Disord 276:1001-1021, 2020. doi: 10.1016/j.jad.2020.07.115
5. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Text Revision (DSM-5-TR). Washington, DC, American Psychiatric Association, 2022.
Diagnosis of OCD
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) criteria
Diagnosis of obsessive-compulsive disorder is clinical, based on the presence of obsessions, compulsions, or both.
Obsessions are defined by both of the following:
Recurrent and persistent thoughts, urges, or images that are experienced, at some time during the disturbance, as intrusive and unwanted, and that in most individuals cause marked anxiety or distress.
The individual attempts to ignore or suppress such thoughts, urges, or images, or to neutralize them with some other thought or action (ie, by performing a compulsion).
Compulsions are defined by both of the following:
Repetitive behaviors (eg, hand washing, ordering, checking) or mental acts (eg, praying, counting, repeating words silently) that the individual feels driven to perform in response to an obsession, or according to rules that must be applied rigidly.
The behaviors or mental acts are aimed at preventing or reducing anxiety or distress or preventing some dreaded event or situation; however, these behaviors or mental acts either are not connected in a realistic way with what they are designed to neutralize or prevent, or are clearly excessive.
The obsessions or compulsions must be time-consuming (eg, > 1 hour a day) or cause clinically significant distress or impairment of functioning. In addition, they must not be attributable to the physiologic effects of a substance (eg, medication, illicit drug) or another medical condition.
Treatment of OCD
Cognitive behavioral therapy (CBT)
Selective serotonin reuptake inhibitor (SSRI) or clomipramine, plus, if needed, an augmenting medicationSelective serotonin reuptake inhibitor (SSRI) or clomipramine, plus, if needed, an augmenting medication
Cognitive behavioral therapy, which encompasses exposure and ritual prevention therapy, has been shown to be effective for in patients with obsessive-compulsive disorder (1). The essential element of exposure and ritual prevention therapy is gradually exposing patients to situations or people that trigger the anxiety-provoking obsessions and rituals while asking them not to perform their rituals. For example, a patient with contamination obsessions and washing compulsions may be asked to touch a toilet seat without washing her hands. This approach allows the anxiety triggered by exposure to diminish through habituation and learning. Improvement often continues for years, especially in patients who master the approach and use it even after formal treatment has ended. However, some patients have incomplete responses (as some also do to medications).
Cognitive therapy techniques (eg, cognitive restructuring) may also be useful in targeting some symptoms of obsessive-compulsive disorder.
SSRIs and clomipramine (a tricyclic antidepressant with potent serotonergic effects), are often very effective. Patients often require higher doses than are typically needed for depression and most anxiety disorders. and clomipramine (a tricyclic antidepressant with potent serotonergic effects), are often very effective. Patients often require higher doses than are typically needed for depression and most anxiety disorders.
Some patients who do not substantially improve with adequate trials of these medications may benefit from augmentation with a medication such as an atypical neuroleptic (eg, aripiprazole, risperidone). Patients with current or past tic comorbidity may be more responsive to augmentation with a neuroleptic (Some patients who do not substantially improve with adequate trials of these medications may benefit from augmentation with a medication such as an atypical neuroleptic (eg, aripiprazole, risperidone). Patients with current or past tic comorbidity may be more responsive to augmentation with a neuroleptic (2). Augmentation with a glutamate modulator (eg, memantine, ). Augmentation with a glutamate modulator (eg, memantine,N-acetylcysteine) has also shown promise (-acetylcysteine) has also shown promise (3). However, there are more supporting data for atypical neuroleptics as SSRI-augmenting agents than for other medications.
Many experts believe that combining exposure and ritual prevention with medications is best, especially for severe cases.
Treatment references
1. Öst L-G, Havnen A, Hansen B, et al: Cognitive behavioral treatments of obsessive-compulsive disorder. A systematic review and meta-analysis of studies published 1993-2014. Clin Psychol Rev 40:156-169, 2015. doi: 10.1016/j.cpr.2015.06.003
2. Bloch MH, Landeros-Weisenberger A, Kelmendi B, et al: A systematic review: Antipsychotic augmentation with treatment refractory obsessive-compulsive disorder. Mol Psychiatry11(7):622-632, 2006. doi: 10.1038/sj.mp.4001823
3. Paydary K, Akamaloo A, Ahmadipour A, et al: N-acetylcysteine augmentation therapy for moderate-to-severe obsessive-compulsive disorder: Randomized, double-blind, placebo-controlled trial. Clin Pharm Ther 41(2):214-219, 2016. doi: 10.1111/jcpt.12370
Key Points
Obsessions are intrusive, unwanted thoughts, images, or urges that usually cause marked distress or anxiety.
Compulsions are excessive, repetitive rituals that people feel they must do to reduce the anxiety caused by their obsessive thoughts or to neutralize their obsessions.
Obsessions and/or compulsions must be time-consuming (eg, > 1 hour a day, often much more) or cause patients significant distress or impairment in functioning.
Treat by gradually exposing patients to situations that trigger the anxiety-provoking obsessions and rituals while requiring them not to perform their rituals. The addition of cognitive approaches to exposure and response prevention may be helpful.
Consider combining exposure and ritual prevention with medications (ie, an SSRI or clomipramine), particularly for severe cases.Consider combining exposure and ritual prevention with medications (ie, an SSRI or clomipramine), particularly for severe cases.
Drugs Mentioned In This Article






