



Acute kidney injury is a rapid (days to weeks) decline in the kidneys’ ability to filter metabolic waste products from the blood.




Causes include conditions that decrease blood flow to the kidneys, that damage the kidneys themselves, or that block drainage of urine from the kidneys.
Symptoms may include swelling, nausea, fatigue, itching, difficulty breathing, and symptoms of the disorder that caused the acute kidney injury.
Serious complications include heart failure and high levels of potassium in the blood.
Diagnosis is with blood and urine tests and usually imaging studies.
Treatment involves correcting the cause of acute kidney injury and sometimes doing dialysis.
(See also Overview of Kidney Failure.)


Acute kidney injury can result from any condition that decreases the blood supply to the kidneys, any disease or toxic substances (also called toxins) affecting the kidneys themselves, or any condition that obstructs urine flow anywhere along the urinary tract.
In many people, no cause of acute kidney injury can be identified.
If both kidneys function normally, damage to one kidney (for example, due to blockage by a kidney stone) does not usually cause major problems because the remaining good kidney can compensate and usually maintain near-normal kidney function, as determined by laboratory measurements. Thus, acute kidney injury may be hard for doctors to detect. For acute kidney injury to cause significant problems, usually both kidneys must be damaged or function abnormally.
Major Causes of Acute Kidney Injury
Cause | Underlying Problem |
|---|---|
Insufficient blood supply to the kidneys | Blood loss Loss of large amounts of sodium and fluid Physical injury that blocks blood vessels Inadequate pumping of the heart (heart failure) Extremely low blood pressure (shock) Liver failure (hepatorenal syndrome) Medications that decrease blood flow to the kidneys |
Injury to the kidneys | Blood supply to the kidneys decreased long enough to damage the kidneys Toxic substances (for example, medications, iodinated contrast agents used in imaging tests, and poisons) Rhabdomyolysis (toxic effect to the kidneys caused by excessive muscle breakdown) Allergic reactions (for example, to certain antibiotics) Disorders affecting the filtering units (nephrons) of the kidneys (for example, acute glomerulonephritis, tubulointerstitial nephritis, tumors damaging the kidneys, or injury to blood vessels as occurs with hemolytic-uremic syndrome, systemic lupus erythematosus [lupus], atheroembolic kidney disease, Goodpasture syndrome, granulomatosis with polyangiitis, or microscopic polyangiitis) Serious bodywide infection (sepsis) |
Obstructed urine flow | Blockage (obstruction) of the bladder (for example, by an enlarged prostate, narrowing of the urethra, or bladder cancer) Tumor pressing on the urinary tract Stones in the ureters or bladder Obstruction within the kidneys (for example, by crystals or stones such as oxalate or uric acid) |
Symptoms of Acute Kidney Injury
Symptoms depend on the
Severity of decline in kidney function
Rate of decline in kidney function
Cause of decline in kidney function
Early symptoms include
Water retention, causing weight gain and swelling of the feet and ankles or puffiness of the face and hands
Decreased amount of urine
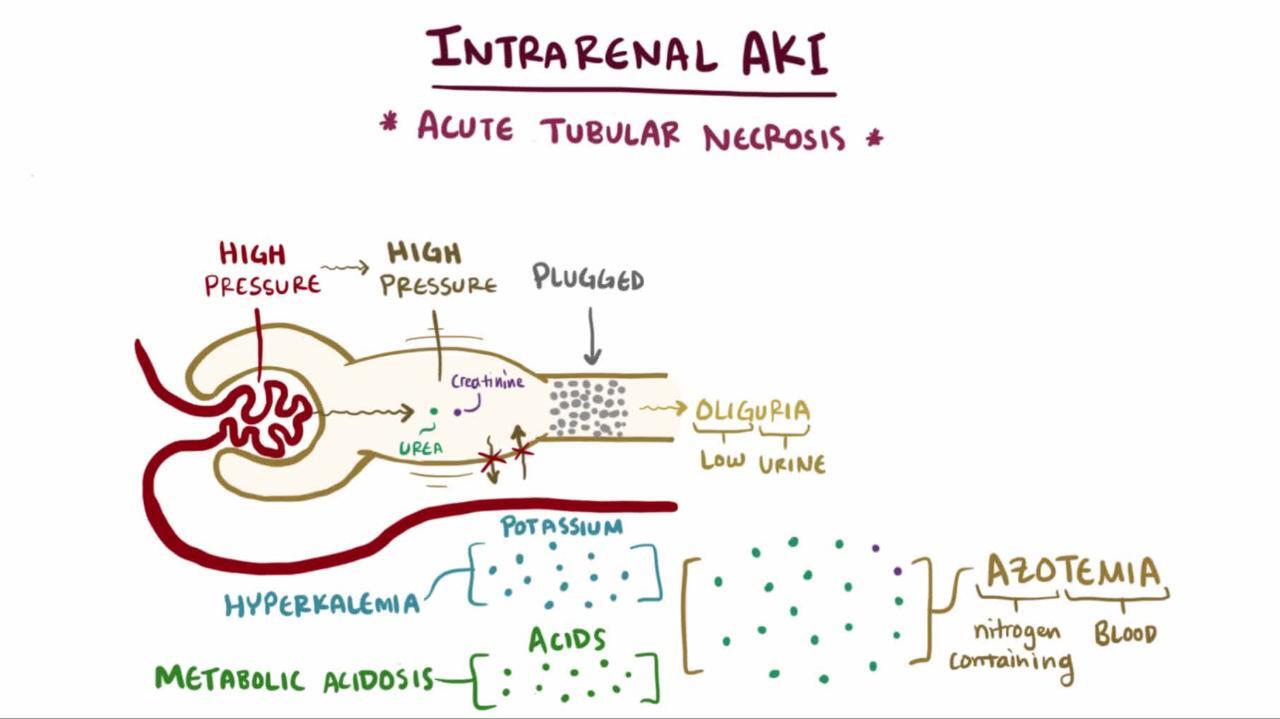
The amount of urine (which for most healthy adults is between 3 cups [about 750 milliliters] and 2 quarts [about 2 liters] per day) often decreases to less than 2 cups (about 500 milliliters) per day or stops completely. Very little urine production is called oliguria, and no urine production is called anuria. However, some people with acute kidney injury continue to produce normal amounts of urine.
Later, as acute kidney injury persists and waste products accumulate in the body, people may experience
Fatigue
Decreased ability to concentrate on mental tasks
Loss of appetite
Nausea
Overall itchiness (pruritus)
People with acute kidney injury may develop more serious symptoms of chest pain, muscle twitching, or even seizures. If fluid accumulates in the lungs, people may become short of breath.
The passing of cola-colored urine may indicate a number of kidney diseases that damage the glomeruli, the filtering units of the kidney. The brown color results from blood passing through the filtering units and may be the first sign of a condition known as a glomerulonephritis (inflammation of the filtering units). Examples include postinfectious glomerulonephritis, antiglomerular basement membrane disease, and lupus nephritis.
If acute kidney injury is caused by a blockage (an obstruction), the backup of urine within the kidneys causes the drainage system to stretch (a condition called hydronephrosis—see figure Hydronephrosis—A Distended Kidney). Urinary tract obstruction often causes a constant dull ache under the lower ribs but may cause crampy pain—ranging from mild to excruciating—usually along the sides (flanks) of the body. Some people with hydronephrosis have blood in their urine from an underlying cause, such as kidney stones. If the obstruction is located below the bladder, the bladder will enlarge. If the bladder enlarges rapidly, people are likely to feel severe pain and pressure in the pelvis, just above the pubic bone. If the bladder enlarges slowly, pain may be minimal, but the lower part of the abdomen may swell because of the enlarged bladder.
If acute kidney injury develops during hospitalization, the condition often relates to some recent injury, surgery, medication, or illness such as infection. Symptoms due to the cause of the acute kidney injury may predominate. For example, high fever, life-threateningly low blood pressure (shock), and symptoms of heart failure or liver failure may occur before symptoms of kidney failure and be more obvious and urgent.
Some of the conditions that cause acute kidney injury also affect other parts of the body. For example, granulomatosis with polyangiitis, which damages blood vessels in the kidneys, may also damage blood vessels in the lungs, causing a person to cough up blood. Rashes are typical of some causes of acute kidney injury, including microscopic polyangiitis, systemic lupus erythematosus (lupus), and some toxic drug exposures.
Diagnosis of Acute Kidney Injury
Blood and urine tests
Imaging tests
Did You Know...
|
The doctor evaluates whether the person has acute kidney injury and, very importantly, its cause.
Physical examination
The physical examination findings may help doctors identify the cause of the acute kidney injury. For example, an enlarged bladder may indicate obstruction of the urinary tract causing hydronephrosis.
Blood tests
Blood tests that measure levels of creatinine and urea nitrogen in the blood are needed to confirm the diagnosis. A progressive daily rise in creatinine indicates acute kidney injury.
The level of creatinine is also the best indicator of the degree or severity of kidney function decline. The higher the level, the more severe the decline in kidney function is likely to be.
Other blood tests detect metabolic imbalances that occur if the decline in kidney function is severe, such as an increase in blood acidity (acidosis, which means low bicarbonate level), a high potassium level (hyperkalemia), a low sodium level (hyponatremia), low calcium (hypocalcemia), and a high phosphorus level (hyperphosphatemia).
Urine tests
Urine tests, such as urinalysis and measurement of certain electrolytes (sodium, potassium, calcium, phosphate), may enable doctors to determine whether the cause of kidney injury is insufficient blood flow to the kidneys, damage to the kidneys, or urinary obstruction.
Imaging
Imaging of the kidneys using ultrasound or computed tomography (CT) is helpful, sometimes by identifying hydronephrosis or an enlarged bladder. Imaging can also reveal the size of the kidneys.
CT of the arteries or veins that lead to and from the kidneys (angiography) may be done if obstruction of blood vessels is the suspected cause. However, angiography is done only when other tests do not provide enough information, because angiography uses an intravenous contrast agent that contains iodine, which carries a risk of additional kidney damage.
Magnetic resonance angiography (MRA) can provide information similar to that provided by angiography. However, MRA has traditionally used gadolinium, a substance that, in people who have severely reduced kidney function, rarely causes a disorder that triggers production of scar tissue in the body (nephrogenic fibrosing dermopathy). The risk of this condition decreased with the newer gadolinium formulations, so MRA could be a good option after discussion with the health care team. If other tests do not reveal the cause of kidney injury, a biopsy may be necessary to determine the diagnosis and the prognosis.
Treatment of Acute Kidney Injury
Treating any treatable causes
Restricting or adjusting fluid intake, electrolytes, and doses of medications eliminated through the kidneys
Sometimes starting dialysis
Some complications of acute kidney injury are serious and may even be life-threatening. People may need to be treated in a critical care unit (also called an intensive care unit [ICU]).
Any treatable cause of acute kidney injury is treated as soon as possible. For example, if obstruction is the cause, a catheter (a tube placed into the bladder to remove urine), cystoscopy (procedure to look inside the bladder with a camera to eliminate the blockage), or surgery may be needed to relieve the obstruction.
Often, the kidneys can heal themselves, especially if the kidney injury has existed for only a few days and there are no complicating problems such as infection. During this time, measures are taken to prevent the decreased kidney function from causing serious problems. Such measures may include the following:
Restricting use of certain medications that may be harsh on the kidneys
Restricting fluids, sodium, phosphorus, and potassium in the diet
Maintaining good nutrition
Giving medications if blood levels of potassium or phosphate are too high, or if bicarbonate is too low
Starting dialysis
Dietary measures
Salt (sodium) and potassium intake is usually restricted. Fluid intake is restricted to replacing the amount lost from the body, unless fluid is needed because there is too little blood flowing to the kidneys. Weight is measured every day because a change in weight is a good indicator of whether there is too much or too little fluid in the body.
A healthy diet is provided to people whose condition allows them to eat. Moderate amounts of protein are acceptable, typically 0.8 to 1 gram per kilogram of body weight (0.4 to 0.5 gram per pound) per day. Restricting the intake of foods that are high in phosphorus, such as dairy products, liver, legumes, nuts, and most soft drinks, lowers the phosphate concentration in the blood.
Medications
Potassium-lowering medications are sometimes given by mouth or rectally to treat a high level of potassium in the blood. Phosphorus-lowering medications (also called phosphorus binders) may be given by mouth with meals to prevent or treat a high level of phosphorus in the blood.
Dialysis
Acute kidney injury may be prolonged, necessitating removal of waste products and excess water. Waste removal can be done through dialysis, usually hemodialysis. If loss of kidney function is predicted to be prolonged or changes in diet and medication(s) are predicted to be ineffective, dialysis is started. Dialysis helps control the complications of acute kidney injury. Dialysis may be needed only temporarily, until the kidneys recover their function, usually in several days to several weeks, sometimes after hospital discharge. If the kidneys do not recover, dialysis (hemodialysis or peritoneal dialysis) is continued indefinitely or kidney transplantation is pursued.
Treament of acute kidney injury caused by obstruction
Fluids are not restricted in people who are recovering from acute kidney injury caused by obstruction. During the recovery period, the kidneys are unable to reabsorb sodium and water normally, and a large amount of urine may be produced for a period of time after the obstruction is relieved. During recovery, people may need replacement of fluids and also electrolytes, such as sodium, potassium, and magnesium.
Prognosis for Acute Kidney Injury
Acute kidney injury and its immediate complications, such as water retention, high acid and potassium levels in the blood, and increased urea nitrogen in the blood, can often be treated successfully. Typically, prognosis is favorable for people whose acute kidney injury is due to decreased blood flow because body fluids have been lost through bleeding, vomiting, or diarrhea—conditions that are reversible with treatment. Prognosis is worse for people in whom some other organs (such as the heart, lungs, or liver) are failing at the same time. How long the person requires dialysis therapy (for example, from days to life-long) depends on the person's overall health and kidney health before acute kidney injury develops.






