


The normal heart beats in a regular, coordinated way because electrical impulses generated and spread by myocytes with unique electrical properties trigger a sequence of organized myocardial contractions. Arrhythmias and conduction disorders are caused by abnormalities in the generation or conduction of these electrical impulses or both.
Any heart disorder, including congenital abnormalities of structure (eg, accessory atrioventricular connection) or function (eg, hereditary ion channelopathies), can disturb rhythm. Systemic factors that can cause or contribute to a rhythm disturbance include electrolyte abnormalities (particularly low potassium or magnesium), hypoxia, hormonal imbalances (eg, hypothyroidism, hyperthyroidism), and drugs and toxins (eg, alcohol, caffeine).
Anatomy of the Cardiac Conduction System
At the junction of the superior vena cava and high lateral right atrium is a cluster of cells called the sinoatrial (SA) or sinus node; the SA node generates the initial electrical impulse of each normal heart beat. Electrical discharge of these pacemaker cells stimulates adjacent cells, leading to stimulation of successive regions of the heart in an orderly sequence.
Impulses are transmitted through the atria to the atrioventricular (AV) node via preferentially conducting internodal tracts and unspecialized atrial myocytes. The AV node is located on the right side of the interatrial septum. It has a slow conduction velocity and thus delays impulse transmission. AV nodal transmission time is heart-rate–dependent and is modulated by autonomic tone and circulating catecholamines to maximize cardiac output at any given atrial rate.
The atria are electrically insulated from the ventricles by the annulus fibrosus except in the anteroseptal region. There, the bundle of His, the continuation of the AV node, enters the top of the interventricular septum, where it bifurcates into the left and right bundle branches, which terminate in Purkinje fibers. The right bundle branch conducts impulses to the anterior and apical endocardial regions of the right ventricle. The left bundle branch fans out over the left side of the interventricular septum. Its anterior portion (left anterior hemifascicle) and its posterior portion (left posterior hemifascicle) stimulate the left side of the interventricular septum, which is the first part of the ventricles to be electrically activated. Thus, the interventricular septum depolarizes left to right, followed by near-simultaneous activation of both ventricles from the endocardial surface through the ventricular walls to the epicardial surface (see figure Electrical pathway through the heart).
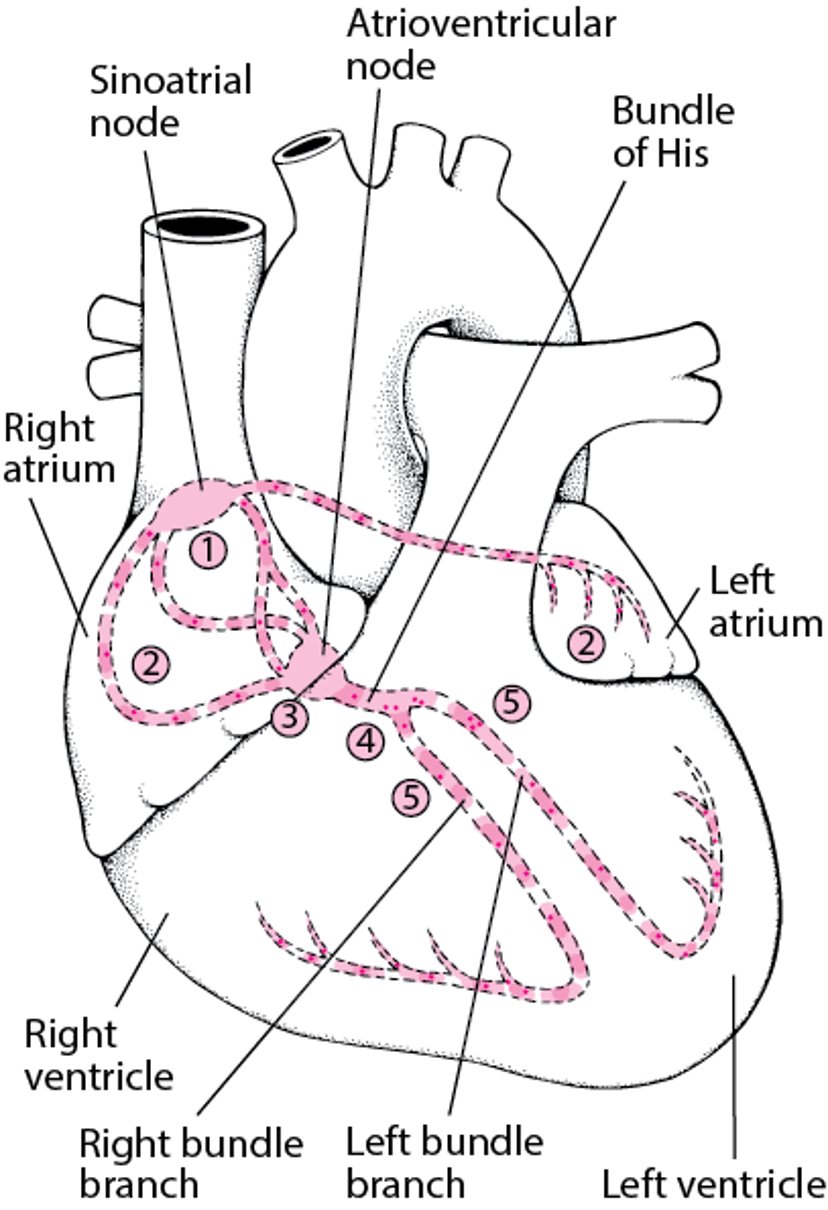
Electrical Pathway Through the Heart
The sinoatrial (sinus) node (1) initiates an electrical impulse that flows through the right and left atria (2), making them contract. When the electrical impulse reaches the atrioventricular node (3), it is delayed slightly. The impulse then travels down the bundle of His (4), which divides into the right bundle branch for the right ventricle (5) and the left bundle branch for the left ventricle (5). The impulse then spreads through the ventricles, making them contract. |

Cardiac Physiology
An understanding of normal cardiac physiology is essential before rhythm disturbances can be understood.
Electrophysiology
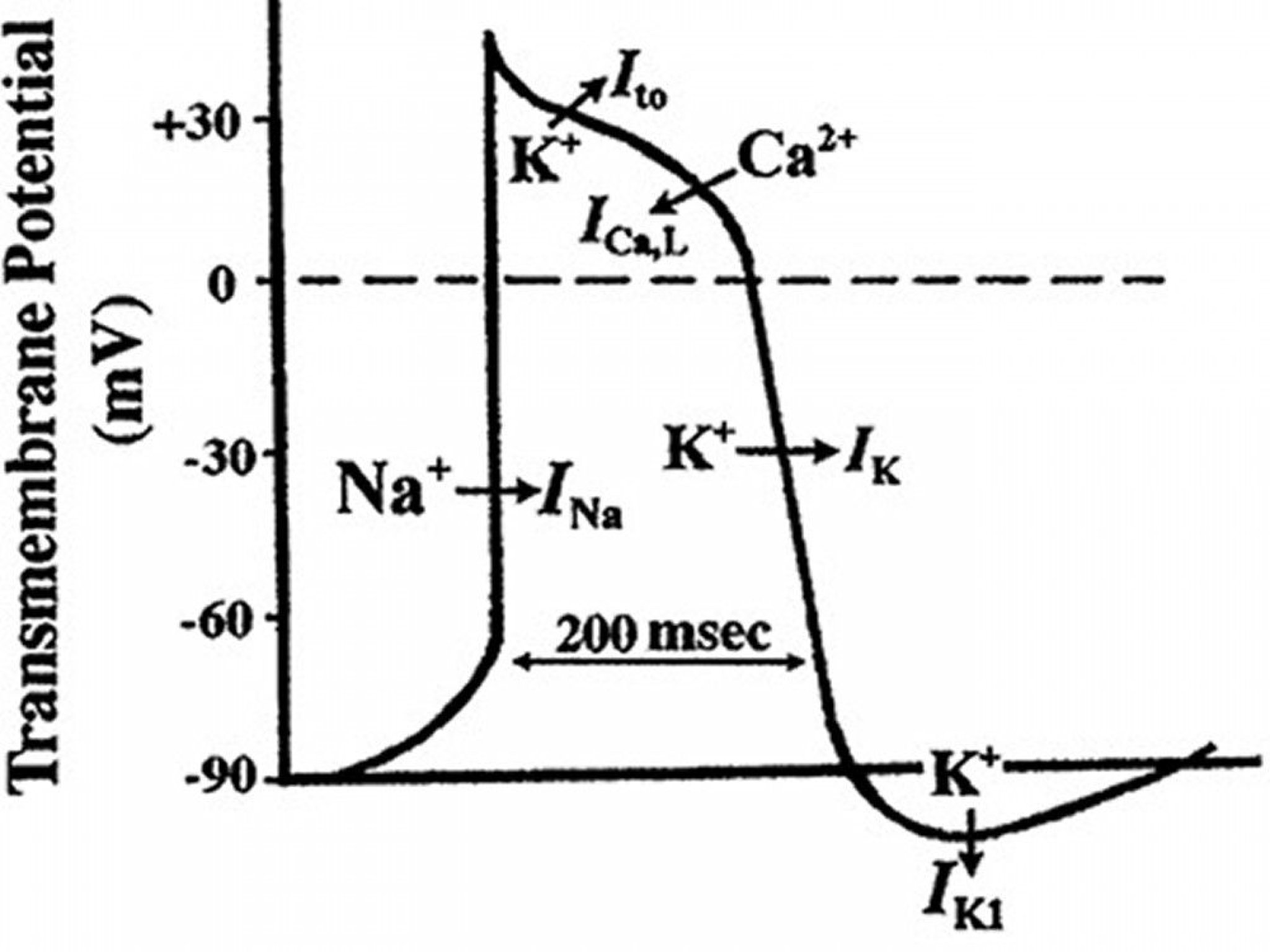
The passage of ions across the myocyte cell membrane is regulated through specific ion channels that cause cyclical depolarization and repolarization of the cell, called an action potential. The action potential of a working myocyte begins when the cell is depolarized from its diastolic −90 mV transmembrane potential to a potential of about −50 mV. At this threshold potential, voltage-dependent fast sodium channels open, causing rapid depolarization mediated by sodium influx down its steep concentration gradient. The fast sodium channel is rapidly inactivated and sodium influx stops, but other time- and voltage-dependent ion channels open, allowing calcium to enter through slow calcium channels (a depolarizing event) and potassium to leave through potassium channels (a repolarizing event).

© Springer Science+Business Media
At first, these 2 processes are balanced, maintaining a positive transmembrane potential and prolonging the plateau phase of the action potential. During this phase, calcium entering the cell is responsible for electromechanical coupling and myocyte contraction. Eventually, calcium influx ceases, and potassium efflux increases, causing rapid repolarization of the cell back to the −90 mV resting transmembrane potential. While depolarized, the cell is resistant (refractory) to a subsequent depolarizing event. Initially, a subsequent depolarization is not possible (absolute refractory period), and after partial but incomplete repolarization, a subsequent depolarization is possible but occurs slowly (relative refractory period).
There are 2 general types of cardiac tissue:
Fast-channel tissues
Slow-channel tissues
Fast-channel tissues (working atrial and ventricular myocytes, His-Purkinje system) have a high density of fast sodium channels and action potentials characterized by
Little or no spontaneous diastolic depolarization (and thus very slow rates of pacemaker activity)
Very rapid initial depolarization rates (and thus rapid conduction velocity)
Loss of refractoriness coincident with repolarization (and thus short refractory periods and the ability to conduct repetitive impulses at high frequencies)
Slow-channel tissues (SA and AV nodes) have a low density of fast sodium channels and action potentials characterized by
More rapid spontaneous diastolic depolarization (and thus more rapid rates of pacemaker activity)
Slow initial depolarization rates (and thus slow conduction velocity)
Loss of refractoriness that is delayed after repolarization (and thus long refractory periods and the inability to conduct repetitive impulses at high frequencies)
Normally, the SA node has the most rapid rate of spontaneous diastolic depolarization, so its cells produce spontaneous action potentials at a higher frequency than other tissues. Thus, the SA node is the dominant automatic tissue (pacemaker) in a normal heart. If the SA node does not produce impulses, tissue with the next highest automaticity rate, typically the AV node, functions as the pacemaker. Sympathetic stimulation increases the discharge frequency of pacemaker tissue, and parasympathetic stimulation decreases it.
There is an inward sodium/potassium current, termed the "funny current," that travels through a hyperpolarization-activated cyclic nucleotide-gated channel (HCN-channel) in sinus node cells that accounts for a large part of their automaticity. Inhibition of this current prolongs the time it takes to achieve critical spontaneous depolarization of pacemaker cells, and thus lowers the heart rate.
Normal cardiac rhythm
The resting sinus heart rate in adults is usually 60 to 100 beats/minute. Slower rates (sinus bradycardia) occur in young people, particularly athletes, and during sleep. Faster rates (sinus tachycardia) occur during exercise, illness, or periods of intense emotion through sympathetic neural and circulating catecholamine drive.
Normally, a marked diurnal variation in heart rate occurs, with lowest rates just before early morning awakening. A slight increase in rate during inspiration with a decrease in rate during expiration (respiratory sinus arrhythmia) is also normal; it is mediated by oscillations in vagal tone and is particularly common among healthy young people. The oscillations lessen but do not entirely disappear with age. Absolute regularity of the sinus rhythm rate is pathologic and occurs in patients with autonomic denervation (eg, in advanced diabetes) or any heart disorder severe enough to decrease parasympathetic cardiac (vagal) tone and activate sympathetic tone. Thus, measures of heart rate variability have been suggested to be useful general measures of cardiovascular health.
Most cardiac electrical activity is represented on the electrocardiogram (ECG—see figure Diagram of the Cardiac Cycle), although SA node, AV node, and His-Purkinje depolarization do not involve enough tissue to be detected. The P wave represents atrial depolarization. The QRS complex represents ventricular depolarization, and the T wave represents ventricular repolarization.
The PR interval (from the beginning of the P wave to the beginning of the QRS complex) is the time from the beginning of atrial activation to the beginning of ventricular activation. Much of this interval reflects slowing of impulse transmission in the AV node. The R-R interval (time between 2 QRS complexes) represents the ventricular rate. The QT interval (from the beginning of the QRS complex to the end of the T wave) represents the duration of ventricular depolarization. Normal values for the QT interval are slightly longer in women; they are also longer in patients with a slower heart rate. The QT interval is corrected (QTc) for the influence of heart rate. The most common formula (all intervals in seconds) is



Pathophysiology of Arrhythmias
Rhythm disturbances result from abnormalities of impulse formation, impulse conduction, or both.
Bradyarrhythmias result from decreased intrinsic pacemaker function or blocks in conduction, principally within the AV node or the His-Purkinje system.
Most tachyarrhythmias are caused by reentry; some result from enhanced normal automaticity or from abnormal mechanisms of automaticity.
Reentry
Reentry is the circular propagation of an impulse around 2 interconnected pathways with different conduction characteristics and refractory periods (see figure Mechanism of typical reentry).
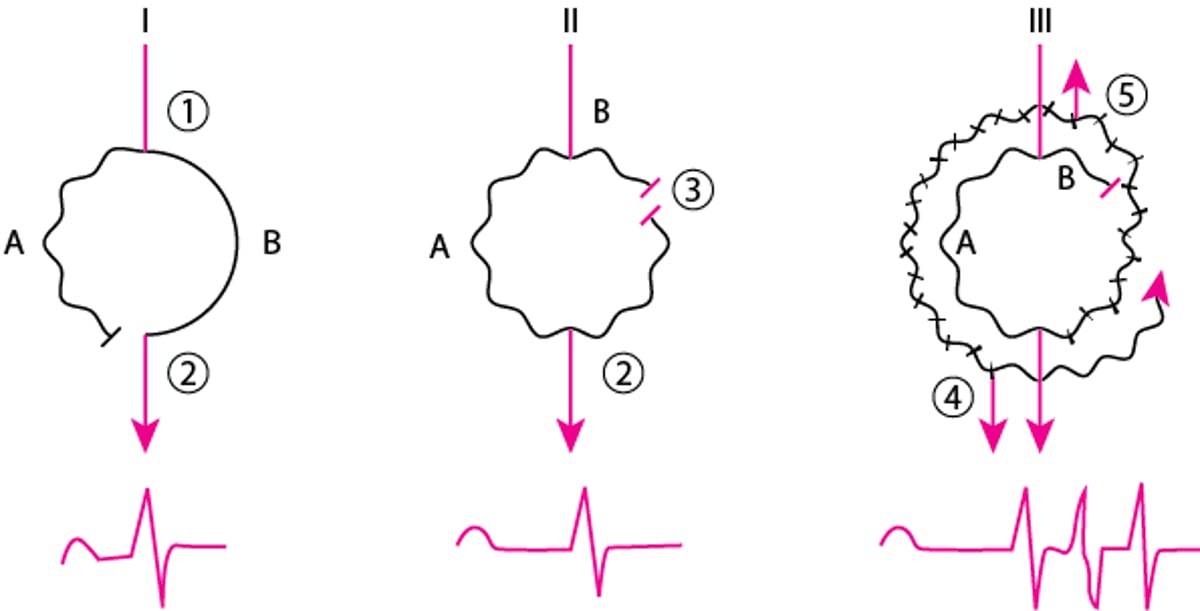
Mechanism of Typical Reentry
Atrioventricular nodal reentry is used here as an example. Two pathways connect the same points. Pathway A has slower conduction and a shorter refractory period. Pathway B conducts normally and has a longer refractory period. I. A normal impulse arriving at 1 goes down both A and B pathways. Conduction through pathway A is slower and finds tissue at 2 already depolarized and thus refractory. A normal sinus beat results. II. A premature impulse finds pathway B refractory and is blocked, but it can be conducted on pathway A because its refractory period is shorter. On arriving at 2, the impulse continues forward and retrograde up pathway B, where it is blocked by refractory tissue at 3. A premature supraventricular beat with an increased PR interval results. III. If conduction over pathway A is sufficiently slow, a premature impulse may continue retrograde all the way up pathway B, which is now past its refractory period. If pathway A is also past its refractory period, the impulse may reenter pathway A and continue to circle, sending an impulse each cycle to the ventricle (4) and retrograde to the atrium (5), producing a sustained reentrant tachycardia. |

Initiation of an Atrioventricular Nodal Reentry Tachycardia
There is an abnormal P wave (P′) and atrioventricular nodal delay (long P′R interval) before onset of the tachycardia. |


Under certain conditions, typically precipitated by a premature beat, reentry can cause continuous circulation of an activation wavefront, causing a tachyarrhythmia (see figure Initiation of an atrioventricular nodal reentry tachycardia). Normally, reentry is prevented by tissue refractoriness following stimulation. However, 3 conditions favor reentry:
Shortening of tissue refractoriness (eg, by sympathetic stimulation)
Lengthening of the conduction pathway (eg, by hypertrophy or abnormal conduction pathways)
Slowing of impulse conduction (eg, by ischemia)
Symptoms and Signs of Arrhythmias
Arrhythmia and conduction disturbances may be asymptomatic or cause palpitations (sensation of skipped beats or rapid or forceful beats), symptoms of hemodynamic compromise (eg, dyspnea, chest discomfort, presyncope, syncope), or cardiac arrest. Occasionally, polyuria results from release of atrial natriuretic peptide during prolonged supraventricular tachycardias (SVTs).
Palpation of pulse and cardiac auscultation can determine ventricular rate and its regularity or irregularity. Examination of the jugular venous pulse waves may help in the diagnosis of AV blocks and tachyarrhythmias. For example, in complete AV block, the atria intermittently contract when the AV valves are closed, producing large a (cannon) waves in the jugular venous pulse. There are few other physical findings of arrhythmias.
Diagnosis of Arrhythmias
ECG
History and physical examination may detect an arrhythmia and suggest possible causes, but diagnosis requires a 12-lead ECG or, less reliably, a rhythm strip, preferably obtained during symptoms to establish the relationship between symptoms and rhythm.
The ECG is approached systematically; calipers measure intervals and identify subtle irregularities. The key diagnostic features are
Rate and regularity of atrial activation
Rate and regularity of ventricular activation
The relationship between the two
Irregular activation signals are classified as regularly irregular or irregularly irregular (no detectable pattern). Regular irregularity is intermittent irregularity in an otherwise regular rhythm (eg, premature beats) or a predictable pattern of irregularity (eg, recurrent relationships between groups of beats).
A narrow QRS complex (< 0.12 seconds) indicates a supraventricular origin (above the His bundle bifurcation).
A wide QRS complex (≥ 0.12 seconds) indicates a ventricular origin (below the His bundle bifurcation) or a supraventricular rhythm conducted with an intraventricular conduction defect or with ventricular preexcitation in the Wolff-Parkinson-White syndrome.
Bradyarrhythmias
Bradyarrhythmias have a slow ventricular rate (< 60 beats/minute in adults). ECG diagnosis of bradyarrhythmias depends on the presence or absence of P waves, morphology of the P waves, and the relationship between P waves and QRS complexes.
Atrioventricular (AV) block is partial or complete interruption of impulse transmission from the atria to the ventricles. There are 3 degrees of AV block: first, second, and third.
In first-degree AV block, each P wave is followed by a QRS complex but the PR interval is > 0.2 seconds. First-degree AV block does not itself cause bradycardia but often coexists with other conditions that do.
In second-degree AV block, some normal P waves are followed by QRS complexes, but some are not. Bradycardia may or may not be present.
Third-degree AV block is indicated by a bradyarrhythmia with no relationship between P waves and QRS complexes and more P waves than QRS complexes; the escape rhythm can be
Junctional with normal AV conduction (narrow QRS complex)
Junctional with aberrant AV conduction (wide QRS complex)
Ventricular (wide QRS complex)
Absence of second- or third-degree AV block is indicated by a regular QRS bradyarrhythmia with a 1:1 relationship between P waves and QRS complexes. P waves preceding QRS complexes indicate sinus bradycardia (if P waves are normal, even if first-degree AV block is present) or sinus arrest with an escape atrial bradycardia (if P waves are abnormal).
P waves after QRS complexes indicate sinus arrest with a junctional or ventricular escape rhythm and retrograde atrial activation. A ventricular escape rhythm results in a wide QRS complex; a junctional escape rhythm usually has a narrow QRS (or a wide QRS with bundle branch block or pre-excitation).
When the QRS rhythm is irregular, P waves usually outnumber QRS complexes; some P waves produce QRS complexes, but some do not (indicating second-degree AV block). An irregular QRS rhythm with a 1:1 relationship between P waves and the following QRS complexes usually indicates sinus arrhythmia with gradual acceleration and deceleration of the sinus rate (if P waves are normal).
Pauses in an otherwise regular QRS rhythm may be caused by blocked P waves (an abnormal P wave can usually be discerned just after the preceding T wave or distorting the morphology of the preceding T wave), sinus arrest or sinus exit block, as well as by second-degree AV block.
Tachyarrhythmias
Tachyarrhythmias have a rapid ventricular rate (> 100 beats/minute in resting adults); tachyarrhythmias may be divided into 4 groups, defined by the QRS complexes:
Visibly regular vs irregular QRS complexes
Narrow vs wide QRS complexes
Irregular, narrow QRS complex tachyarrhythmias include the following 4 rhythms. Differentiation is based on atrial ECG signals, which are best seen in the longer pauses between QRS complexes.
Atrial fibrillation (AF): Atrial ECG signals (usually best seen in lead V1) that are continuous, irregular in timing and morphology, and very rapid (> 300 beats/minute) without discrete P waves
Atrial flutter with variable AV conduction: Regular, discrete, uniform atrial signals (usually best seen in leads II, III, and aVF) without intervening isoelectric periods, usually at rates > 250 beats/minute
True atrial tachycardia with variable AV conduction: Regular, discrete, uniform, abnormal atrial signals with intervening isoelectric periods (usually at rates < 250 beats/minute)
Multifocal atrial tachycardia: Discrete P waves that vary from beat to beat with at least 3 different morphologies
Irregular, wide QRS complex tachyarrhythmias include
The above 4 irregular, narrow atrial tachyarrhythmias conducted with either bundle branch block or ventricular preexcitation
Polymorphic ventricular tachycardia (VT)
Differentiation is based on atrial ECG signals and the presence in polymorphic VT of a very rapid ventricular rate (> 250 beats/minute).
Regular, narrow QRS complex tachyarrhythmias include
Sinus tachycardia
Atrial flutter with a consistent AV conduction ratio
True atrial tachycardia with a consistent AV conduction ratio
Paroxysmal supraventricular tachycardias ([SVT] such as AV nodal reentrant SVT, orthodromic reciprocating AV tachycardia in the presence of an accessory AV connection, and SA nodal reentrant SVT)
Vagal maneuvers or pharmacologic AV nodal blockade can help distinguish among these tachycardias. With these maneuvers, sinus tachycardia is not terminated, but it slows or AV block develops, disclosing normal P waves. Similarly, atrial flutter and true atrial tachycardia are usually not terminated, but AV block discloses flutter waves or abnormal P waves. The most common forms of paroxysmal SVT (AV nodal reentry and orthodromic reciprocating tachycardia) must terminate if AV block occurs.
Regular, wide QRS complex tachyarrhythmias include
The above 4 regular, narrow QRS complex tachyarrhythmias conducted with bundle branch block or ventricular preexcitation
Monomorphic VT
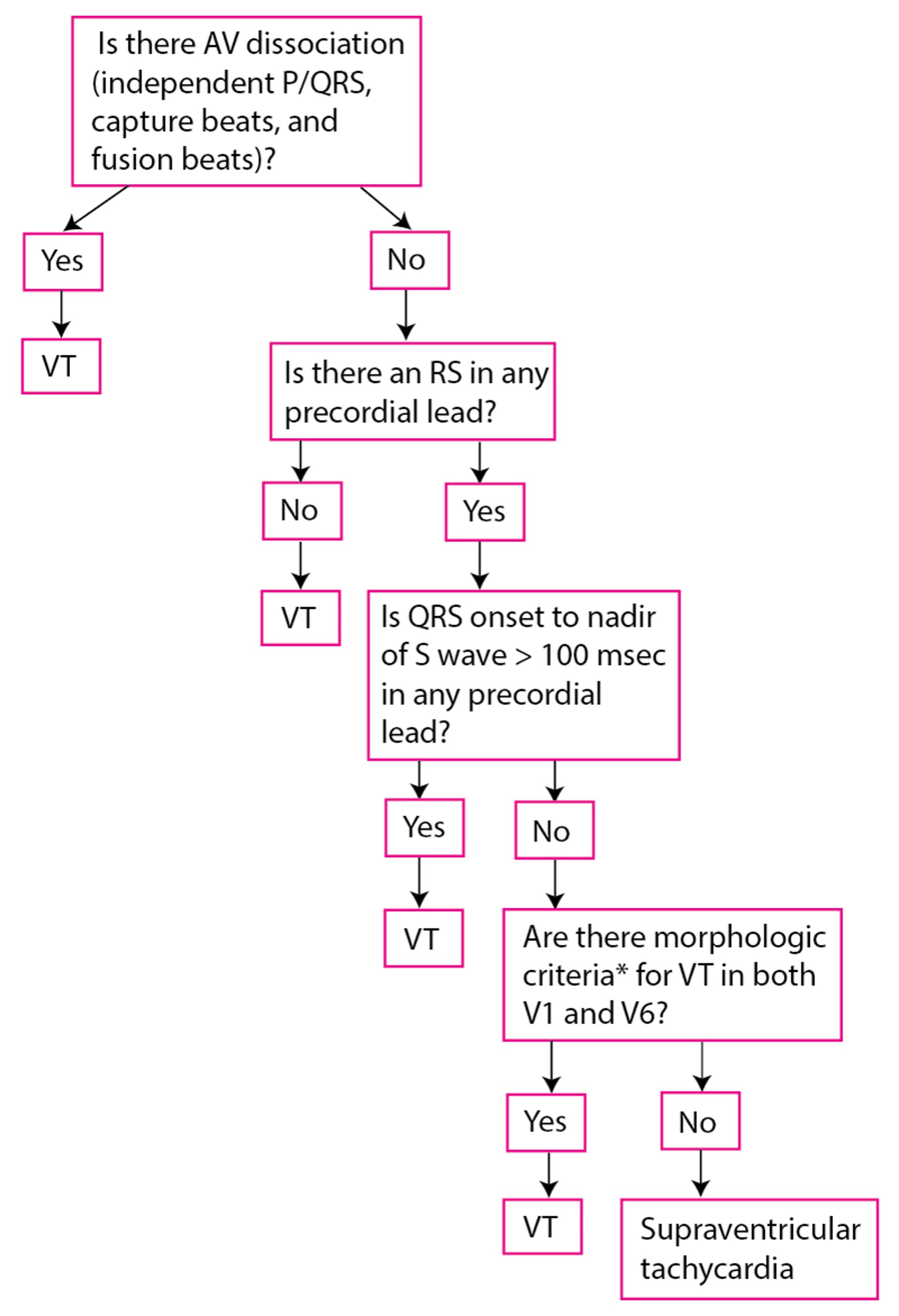
Vagal maneuvers can help distinguish among them. ECG criteria to distinguish between VT and SVT with an intraventricular conduction defect are often used (see figure Modified Brugada criteria for ventricular tachycardia). When in doubt, the rhythm is assumed to be VT because some drugs for SVTs can worsen the clinical state if the rhythm is VT; however, the reverse is not true.
Pearls & Pitfalls
|
Modified Brugada Criteria for Ventricular Tachycardia
*With RBBB QRS:
*With LBBB QRS:
|
AV = atrioventricular; LBBB = left bundle branch block; msec = millisecond; RBBB = right bundle branch block; VT = ventricular tachycardia. |

Treatment of Arrhythmias
Treatment of cause
Sometimes antiarrhythmic drugs, pacemakers, cardioversion-defibrillation, catheter ablation, or surgery
The need for treatment varies; it is guided by symptoms and risks of the arrhythmia. Asymptomatic arrhythmias without serious risks do not require treatment even if they worsen. Symptomatic arrhythmias may require treatment to improve quality of life. Potentially life-threatening arrhythmias require treatment.
Treatment is directed at causes. If necessary, direct antiarrhythmic therapy is used. Direct antiarrhythmic therapy includes, either alone or in combination,
Pacemakers (and a special form of pacing, cardiac resynchronization therapy)
Patients with arrhythmias that have caused or are likely to cause symptoms of hemodynamic compromise may have to be restricted from driving until response to treatment has been assessed.
Surgery for cardiac arrhythmias
Surgery to remove a focus of a tachyarrhythmia is becoming less necessary as the less invasive ablation techniques evolve. But surgery is indicated when an arrhythmia is refractory to ablation or when another indication requires a cardiac surgical procedure, most commonly when patients with atrial fibrillation require valve replacement or repair or when patients with ventricular tachycardia require revascularization or resection of a left ventricular aneurysm.







