

Reentrant (paroxysmal) supraventricular tachycardias (PSVT) involve reentrant pathways with a component above the bifurcation of the His bundle. Subtypes include atrioventricular nodal reentrant tachycardia (AVNRT), atrioventricular reentrant tachycardia (AVRT) using an accessory pathway, atrial reentrant tachycardia, and sinus nodal reentrant tachycardia. Patients have sudden episodes of palpitations that begin and terminate abruptly; some have dyspnea or chest discomfort. Diagnosis is clinical and by electrocardiography. Initial treatment is usually with vagotonic maneuvers. If these maneuvers are ineffective, treatment is with IV adenosine or nondihydropyridine calcium channel blockers for narrow QRS rhythms or for wide QRS rhythms known to be a reentrant SVT with aberrant conduction that requires atrioventricular nodal conduction. Procainamide or amiodarone are effective for other wide QRS rhythms. Synchronized cardioversion can be done for all cases in which medications are ineffective or there is hemodynamic instability.Reentrant (paroxysmal) supraventricular tachycardias (PSVT) involve reentrant pathways with a component above the bifurcation of the His bundle. Subtypes include atrioventricular nodal reentrant tachycardia (AVNRT), atrioventricular reentrant tachycardia (AVRT) using an accessory pathway, atrial reentrant tachycardia, and sinus nodal reentrant tachycardia. Patients have sudden episodes of palpitations that begin and terminate abruptly; some have dyspnea or chest discomfort. Diagnosis is clinical and by electrocardiography. Initial treatment is usually with vagotonic maneuvers. If these maneuvers are ineffective, treatment is with IV adenosine or nondihydropyridine calcium channel blockers for narrow QRS rhythms or for wide QRS rhythms known to be a reentrant SVT with aberrant conduction that requires atrioventricular nodal conduction. Procainamide or amiodarone are effective for other wide QRS rhythms. Synchronized cardioversion can be done for all cases in which medications are ineffective or there is hemodynamic instability.
(See also Overview of Arrhythmias.)
Pathophysiology of Reentrant SVTs
Reentrant (paroxysmal) supraventricular tachycardias are defined as the sudden-onset, sudden-offset, rapid (120 to 250 beats per minute), regular (successive RR interval variations ≤ 0.04 seconds), narrow QRS complex (or wide QRS complex with bundle branch block) tachycardias that are not sinus tachycardia, atrial fibrillation, or atrial flutter. So defined, the incidence of reentrant (paroxysmal) supraventricular tachycardia is approximately 35/100,000, and the prevalence is 2 to 3/1000 people in the United States (1). In adult patients, the proportions of subtypes are (2):
Atrioventricular (AV) nodal reentrant tachycardia (AVNRT) (50% to 60%)
Atrioventricular reentrant tachycardia (AVRT) using accessory bypass tract (20% to 30%) OR
Atrial reentrant tachycardia and sinoatrial (SA) node reentrant tachycardia (10% to 15%)
Atrioventricular reentrant tachycardia (AVRT) is the most common type seen in Wolff-Parkinson-White syndrome. In children, atrioventricular nodal reentrant tachycardia is much less common; atrioventricular reentrant tachycardia, atrial reentrant tachycardia, and junctional ectopic tachycardia are more common.
Atrioventricular nodal reentrant tachycardia (AVNRT)
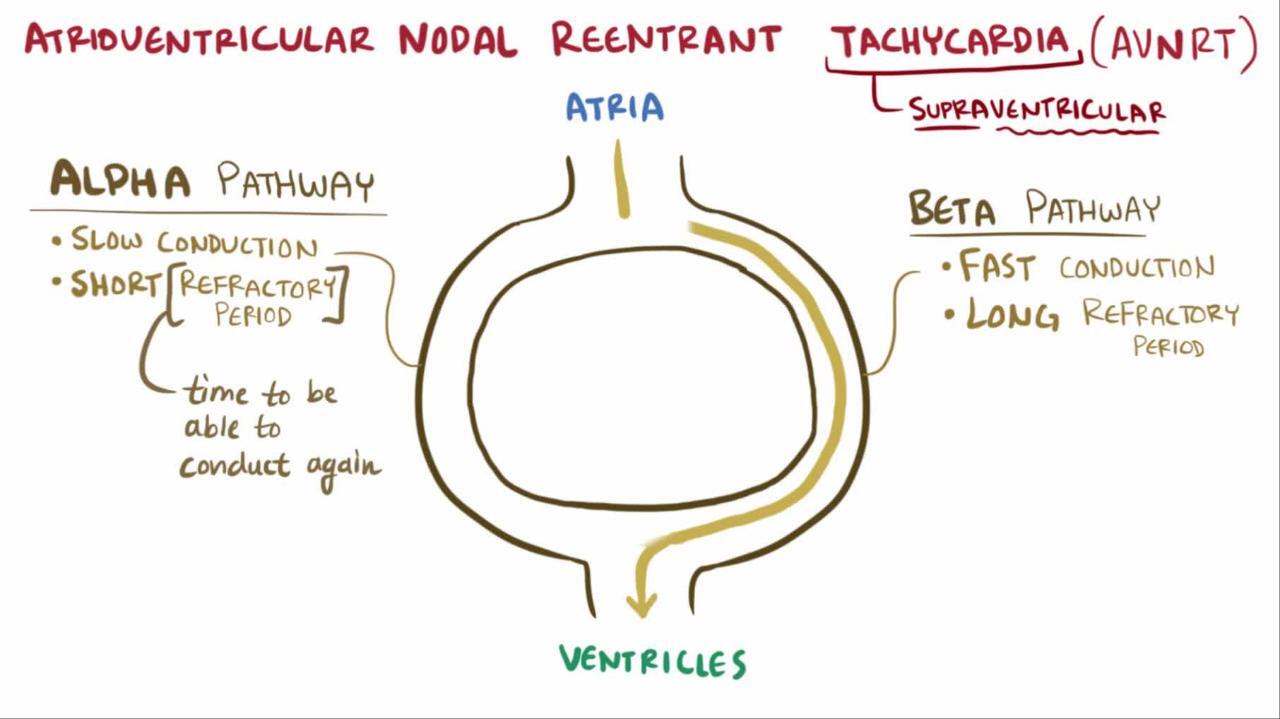
AVNRT occurs most often in otherwise healthy people. It is most commonly triggered by an atrial premature beat. The AV node has multiple extensions that serve as routes for atrial activations to enter the AV node. In most people, the superior/anterior extension bypasses much of the AV node and the antegrade conduction time to the His-Purkinje system and ventricles is short (a fast pathway) while the inferior/posterior extension uses all of the AV node and the antegrade conduction time to the His-Purkinje system and ventricles is long (a slow pathway).
The fast pathway tends to have a longer refractory period, which blocks antegrade transmission of a premature atrial depolarization at longer AA intervals, while the slow pathway tends to have a shorter refractory period, which blocks antegrade transmission of a premature atrial depolarization at shorter AA intervals. At a premature atrial depolarization coupling interval longer than the refractory period of both pathways the antegrade transmission through the fast pathway reaches the His-Purkinje system and the ventricles while the antegrade transmission through the slow pathway finds the His-Purkinje system refractory, having just been activated by the fast pathway, and the slow pathway transmission is blocked. The ECG shows a normal PR interval for this beat.
At a premature atrial depolarization coupling interval shorter than the refractory period of both pathways neither antegrade transmission reaches the His-Purkinje system and ventricles. The ECG shows a blocked premature atrial beat. At a premature atrial depolarization coupling interval less than the refractory period of the fast pathway but longer than the refractory period of the slow pathway, antegrade fast pathway transmission is blocked, but antegrade slow pathway conduction proceeds. The ECG shows a sudden increase in the PR interval for this beat (see figure Initiation of Atrioventricular Nodal Reentry Tachycardia).
Initiation of an Atrioventricular Nodal Reentry Tachycardia
There is an abnormal P wave (P′) and atrioventricular nodal delay (long P′R interval) before onset of the tachycardia. |


When antegrade conduction through the slow pathway is sufficiently slow, it can find the lower portion of the fast pathway ready to conduct, but now in the retrograde direction. When this retrograde fast pathway transmission finds the upper portion of the slow pathway ready to conduct again in the antegrade conduction, around-and-around AV nodal reentry occurs. The ECG then shows a rapid, regular, tachycardia. Such typical, or slow-fast, AV nodal reentry is the usual (90%) type of AV nodal reentry (2). Less commonly, and more often induced by a ventricular premature beat, the reentry occurs in the opposite direction (atypical or fast-slow AV nodal reentry).
Atrioventricular reentrant tachycardia (AVRT)
AVRT occurs in patients with an accessory AV connection and is the most common type seen in Wolff-Parkinson-White syndrome. It runs most commonly from an atrium to a ventricle and rarely from an atrium to a portion of the conduction system or from a portion of the conduction system to the ventricle. An accessory pathway connecting an atrium and a ventricle is the substrate for the Wolff-Parkinson-White syndrome. When the accessory AV connection conducts in the antegrade direction, the AV nodal delay is bypassed, and a portion of ventricular myocardium is activated before the remainder of ventricular myocardium is activated by the normal conduction system. This ventricular pre-excitation produces the short PR interval and delta wave that, along with symptoms of paroxysmal tachycardia, define the classic (manifest) Wolff-Parkinson-White syndrome (3). When the accessory AV connection does not conduct in the antegrade direction, the ECG is normal, and the presence of the accessory AV connection is concealed (concealed Wolff-Parkinson-White syndrome). In either event, if the accessory AV connection conducts in the retrograde direction, it can support a form of paroxysmal supraventricular tachycardia called orthodromic atrioventricular reentrant tachycardia.


Image courtesy of L. Brent Mitchell, MD.
The accessory AV connection tends to have a longer refractory period than the AV node. At a premature atrial depolarization coupling interval less than the refractory period of the accessory AV pathway, but longer than the refractory period of the AV node, antegrade accessory AV pathway transmission is blocked but antegrade AV nodal conduction proceeds. In patients with classic (manifest) Wolff-Parkinson-White syndrome, the ECG shows a sudden increase in the PR interval and loss of the delta for this beat. In patients with concealed Wolff-Parkinson-White syndrome, the ECG only shows an increase in the PR interval for this beat.
When antegrade conduction through the AV node is sufficiently slow, it can find the distal accessory AV connection ready to conduct, but in the retrograde direction. When this retrograde accessory AC connection transmission finds the atria and, subsequently, the AV node ready to conduct again in the antegrade direction, around-and-around atrioventricular reentry occurs. The ECG then shows a rapid regular tachycardia. This orthodromic atrioventricular tachycardia is the usual (95%) type of AV reentrant tachycardia (4). Less commonly, and more often induced by a ventricular premature beat, the reentry occurs in the opposite direction (antidromic atrioventricular reentrant tachycardia).
An uncommon near-incessant form of atrioventricular reentrant tachycardia, permanent junctional reentrant tachycardia (PJRT), occurs in the setting of an antegrade concealed, usually posteroseptal, accessory AV connection that has very slow retrograde conduction. Although the tachycardia may be incessant (typically with each spontaneous termination followed by a sinus beat that re-initiates the tachycardia), some patients have a paroxysmal pattern similar to other PSVTs. The incessant form may lead to a tachycardia-induced cardiomyopathy and heart failure. Since 5% of patients with an accessory AV connection have multiple accessory AV connections (2), it is also possible to have a dual accessory AV connection atrioventricular reentrant tachycardia that uses one accessory AV connection for antegrade conduction and another accessory AV connection for retrograde conduction.
Atrial reentrant tachycardia and sinus nodal reentrant tachycardia
Atrial reentrant tachycardias include the micro-reentrant atrial tachycardias (see Focal atrial tachycardia) and the macro-reentrant atrial tachycardias. The latter most commonly occur in patients with structural heart disease but may occur in isolation. The macro-reentrant tachycardias are produced by wide area reentry around normal or abnormal, anatomical or functional barriers. When the ECG shows continuous atrial electrical activity (flutter waves without intervening isoelectric periods), such rhythms are also called atypical atrial flutter. When the ECG shows discrete P-waves with intervening isoelectric periods, the distinction from focal atrial tachycardia due to micro-reentry is arbitrary and requires intracardiac mapping. Sinus nodal reentrant tachycardia is a focal atrial tachycardia with a P-wave morphology the same as that during sinus rhythm. The reentry in this instance is located in the upper crista terminalis near the sinus node, and it is debatable whether the sinus node is actually involved in the circuit.
(See also figure Mechanism of Typical Reentry.)

Pathophysiology references
1. Orejarena LA, Vidaillet H Jr, DeStefano F, et al: Paroxysmal supraventricular tachycardia in the general population. J Am Coll Cardiol 31(1):150–157, 1998. doi: 10.1016/s0735-1097(97)00422-1
2. Kadish A, Passman R: Mechanisms and management of paroxysmal supraventricular tachycardia. Cardiol Rev 7(5):254–64, 1999. doi: 10.1097/00045415-199909000-00009.
3. Brugada J, Katritsis DG, Arbelo E, et al: 2019 ESC Guidelines for the management of patients with supraventricular tachycardia. The Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J 41(5):655-720, 2020. doi: 10.1093/eurheartj/ehz467
4. Page RL, Joglar JA, Caldwell MA, et al: 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society [published correction appears in J Am Coll Cardiol. 2016 Dec 27;68(25):2922-2923]. J Am Coll Cardiol 67(13):e27–e115, 2016. doi: 10.1016/j.jacc.2015.08.856
Symptoms and Signs of Reentrant SVTs
Most patients present during young adulthood or middle age. They typically have episodes of sudden-onset, sudden-offset, rapid, regular palpitations often associated with symptoms of hemodynamic compromise (eg, dyspnea, chest discomfort, light-headedness). Attacks may last only a few seconds or persist for several hours (rarely, > 12 hours).
Infants present with episodic breathlessness, lethargy, feeding problems, or rapid precordial pulsations. If the episode of tachycardia is protracted, infants may present with heart failure.
Examination is usually unremarkable except for a heart rate of 120 to 240 beats/minute, most commonly 180 to 210 beats/minute.
Diagnosis of Reentrant SVTs
Electrocardiography (ECG)
Diagnosis of supraventricular tachycardia is by ECG showing rapid, regular tachycardia. Previous tracings, if available, are reviewed for ECG signs of manifest WPW syndrome or pre-existing bundle branch block.
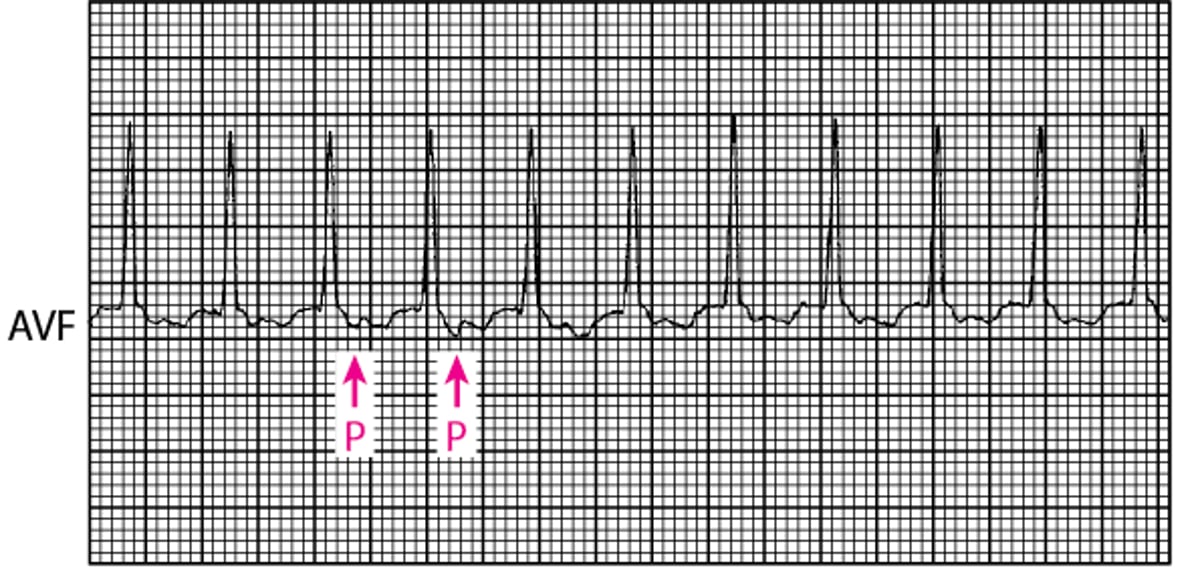
P waves vary. In most cases of typical (slow-fast) AV nodal reentrant tachycardia, retrograde P waves are in the terminal portion of the QRS complex (often producing a pseudo-R′ deflection in lead V1); about one-third occur just after the QRS complex, and very few occur immediately before. P waves always follow the QRS complex in orthodromic typical atrioventricular reentrant tachycardia using an accessory AV connection as in WPW syndrome. In either instance the P wave, when identified, is in the first half of the RR interval (RP < PR), a short RP tachycardia. The exception is the rare typical AV nodal reentrant tachycardia with a P wave immediately (≤ 0.12 seconds) before the QRS complex; this tachycardia is too short to have conducted through the AV node to have created that QRS complex.
The P wave, when identified, in atypical (fast-slow) AV nodal reentrant tachycardia, in permanent junctional reentrant tachycardia (PJRT), and in antidromic atrioventricular reentrant tachycardia is in the second half of the RR interval (RP > PR), a long RP tachycardia. In each of these paroxysmal supraventricular tachycardias, the P-wave morphology is negative in the inferior leads (II, III, and AVF), indicating that the atrial activation wavefront is moving from low to high through the atria. In atrial reentrant tachycardia, the P-wave may fall anywhere in the RR interval as determined by the relationship between the tachycardia rate and the AV conduction delay; the P-wave morphology may or may not be negative in the inferior leads (II, III, and AVF), depending on the site of origin of atrial depolarization.
The QRS complex is narrow except with coexisting bundle branch block. Wide QRS complexes also result from activation of the ventricles exclusively down an accessory AV connection in antidromic atrioventricular reentrant tachycardia or dual accessory connection atrioventricular reentrant tachycardia. If a wide-complex tachycardia is not known to be supraventricular in origin, it must be treated acutely as ventricular tachycardia.
In addition to the position of the P-wave, the 2 most common forms of reentrant (paroxysmal) supraventricular tachycardia, typical AV nodal reentrant tachycardia amd orthodromic atrioventricular reentrant tachycardia, also differ in that typical AV nodal reentrant tachycardia patients are more often female and usually present in their third or fourth decade with a tachycardia in the 150 to 200 beats/minute range. Patients with orthodromic atrioventricular tachycardia are more often male and usually present in their second or third decade with a tachycardia in the 180 to 220 beats/minute range.
The reentrant SVTs may also differ in their response to vagal maneuvers or adenosine administration. Although each of the reentrant SVTs may have no response to these interventions, the SVTs with conduction through the AV as part of their reentrant circuit must terminate if a single AV nodal transmission is blocked. These SVTs are both typical and atypical AV nodal reentrant tachycardias and both orthodromic and antidromic atrioventricular reentrant tachycardias. Other than no response, the most common response of an atrial reentrant tachycardia to vagal maneuvers or The reentrant SVTs may also differ in their response to vagal maneuvers or adenosine administration. Although each of the reentrant SVTs may have no response to these interventions, the SVTs with conduction through the AV as part of their reentrant circuit must terminate if a single AV nodal transmission is blocked. These SVTs are both typical and atypical AV nodal reentrant tachycardias and both orthodromic and antidromic atrioventricular reentrant tachycardias. Other than no response, the most common response of an atrial reentrant tachycardia to vagal maneuvers oradenosine is for AV nodal block to occur transiently without termination of the tachycardia. This produces a long RR interval in which previously hidden P-wave should become more evident on the ECG. Although atrial reentrant tachycardias do not require AV nodal conduction for their perpetuation, some such rhythms may terminate with vagal maneuvers or adenosine, particularly if their mechanism is triggered automaticity or micro-reentry. Termination with the final event being a P-wave on the ECG strongly suggests that the SVT is not atrial in origin as this would require the coincidence that the atrial driver terminated at exactly the same time as the AV node failed to conduct.
Vagal maneuvers or adenosine are also useful to distinguish reentrant SVTs from atrial flutter (the usual response being to produce AV block without termination of the flutter but with the flutter waves being evident on the ECG) or sinus tachycardia (the usual response being gradual slowing to a new rate followed by gradual acceleration to the previous rate).
Pearls & Pitfalls
|
Narrow QRS Tachycardia: Orthodromic Atrioventricular Reentrant Tachycardia Using an Accessory AV Connection in Wolff-Parkinson-White Syndrome
Activation is as follows: atrioventricular node, His-Purkinje system, ventricle, accessory connection, atria. The P wave occurs shortly after the QRS complex; it is a short RP interval tachycardia (RP < PR). |

Treatment of Reentrant SVTs
Vagotonic maneuvers
AdenosineAdenosine
Verapamil, diltiazem, or a beta-blocker if narrow, regular QRS complexVerapamil, diltiazem, or a beta-blocker if narrow, regular QRS complex
For frequent recurrence, ablation
Many episodes stop spontaneously before treatment.
Vagotonic maneuvers (eg, Valsalva maneuver, unilateral carotid sinus massage, ice water facial immersion, swallowing of ice-cold water), particularly if used early, may terminate the tachyarrhythmia; some patients use these maneuvers at home (1).
AV node blockers are used if vagotonic maneuvers are ineffective and the QRS complex is narrow (indicating orthodromic conduction) and regular (indicating the episode is not atrial fibrillation); blocking conduction through the AV node for one beat interrupts the reentrant cycle. Adenosine is the first choice. Dose is 6 mg by rapid IV bolus (0.05 to 0.1 mg/kg in children), followed by a 20-mL saline bolus. If this dosage is ineffective, 2 subsequent 12-mg doses are given every 5 minutes. are used if vagotonic maneuvers are ineffective and the QRS complex is narrow (indicating orthodromic conduction) and regular (indicating the episode is not atrial fibrillation); blocking conduction through the AV node for one beat interrupts the reentrant cycle. Adenosine is the first choice. Dose is 6 mg by rapid IV bolus (0.05 to 0.1 mg/kg in children), followed by a 20-mL saline bolus. If this dosage is ineffective, 2 subsequent 12-mg doses are given every 5 minutes.Adenosine sometimes causes a brief (2- to 3-second) period of cardiac standstill, which may distress patient and physician. Verapamil 5 mg IV or diltiazem 0.25 to 0.35 mg/kg IV are alternatives (sometimes causes a brief (2- to 3-second) period of cardiac standstill, which may distress patient and physician. Verapamil 5 mg IV or diltiazem 0.25 to 0.35 mg/kg IV are alternatives (2).
For a regular, wide QRS complex tachycardia known to be an antidromic reciprocating tachycardia not involving double accessory pathways (which must be identified by the history; they cannot be established acutely), AV nodal blockers may also be effective. However, if the mechanism of the tachycardia is unknown and ventricular tachycardia has not been excluded, AV nodal blockers should be avoided because they may worsen hemodynamics in ventricular tachycardias. In such cases (or those in which medications are ineffective), IV procainamide or amiodarone can be used. Alternatively, For a regular, wide QRS complex tachycardia known to be an antidromic reciprocating tachycardia not involving double accessory pathways (which must be identified by the history; they cannot be established acutely), AV nodal blockers may also be effective. However, if the mechanism of the tachycardia is unknown and ventricular tachycardia has not been excluded, AV nodal blockers should be avoided because they may worsen hemodynamics in ventricular tachycardias. In such cases (or those in which medications are ineffective), IV procainamide or amiodarone can be used. Alternatively,synchronized cardioversion with 50 joules (0.5 to 2 joules/kg for children) is quick and safe and may be preferred to these more toxic agents (2).
When episodes of reentrant (paroxysmal) supraventricular tachycardia are frequent or bothersome, transvenous catheter ablation is the preferred treatment and is usually curative (2). If ablation is not acceptable, medication prophylaxis usually begins with digoxin and proceeds, as required, to beta-blockers, nondihydropyridine calcium channel blockers, or both, then to one or more class Ia, class Ic, or class III antiarrhythmics (see table ). If ablation is not acceptable, medication prophylaxis usually begins with digoxin and proceeds, as required, to beta-blockers, nondihydropyridine calcium channel blockers, or both, then to one or more class Ia, class Ic, or class III antiarrhythmics (see tableAntiarrhythmic Medications). However, postadolescent patients with manifest Wolff-Parkinson-White syndrome (in whom atrial fibrillation becomes more likely) should not receive digoxin, a nondihydropyridine calcium channel blocker, or a beta-blocker alone (). However, postadolescent patients with manifest Wolff-Parkinson-White syndrome (in whom atrial fibrillation becomes more likely) should not receive digoxin, a nondihydropyridine calcium channel blocker, or a beta-blocker alone (2) (see also Atrial Fibrillation and Wolff-Parkinson-White Syndrome).
Treatment references
1. Waxman MB, Wald RW, Sharma AD, et al: Vagal techniques for termination of paroxysmal supraventricular tachycardia. Am J Cardiol 46(4):655–664, 1980. doi: 10.1016/0002-9149(80)90517-2
2. Brugada J, Katritsis DG, Arbelo E, et al: 2019 ESC Guidelines for the management of patients with supraventricular tachycardia. The Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J 41(5):655–720, 2020. doi: 10.1093/eurheartj/ehz467
Key Points
Symptoms of reentrant (paroxysmal) supraventricular tachycardias (PSVT) begin and end suddenly.
AV nodal re-entry is the most common PSVT.
Wolff-Parkinson-White syndrome, whether manifest or concealed, is the most common accessory pathway PSVT.
QRS complexes are typically narrow, rapid, and regular; however, wide complexes may occur and must be differentiated from ventricular tachycardia.
Vagotonic maneuvers (eg, Valsalva maneuver) sometimes help.
Use atrioventricular (AV) nodal blockers for narrow complex tachycardia; adenosine is the first choice, and if ineffective, verapamil or diltiazem are alternatives.Use atrioventricular (AV) nodal blockers for narrow complex tachycardia; adenosine is the first choice, and if ineffective, verapamil or diltiazem are alternatives.
Avoid AV nodal blockers for wide complex tachycardia not known to be PSVT; use synchronized cardioversion or procainamide or amiodarone.Avoid AV nodal blockers for wide complex tachycardia not known to be PSVT; use synchronized cardioversion or procainamide or amiodarone.
Drugs Mentioned In This Article





