


Classic (manifest) Wolff-Parkinson-White syndrome is due to an accessory atrioventricular connection that produces a prototypical ECG consisting of a short PR interval, a wide QRS complex with an initial slurred component (delta wave), and secondary repolarization changes in association with symptomatic reentrant (paroxysmal) supraventricular tachycardia. Reentrant (paroxysmal) supraventricular tachycarida produces sudden episodes of palpitations that begin and terminate abruptly; some patients have dyspnea or chest discomfort. The accessory atrioventricular (AV) connection can facilitate very rapid ventricular response rates to any fast supraventricular arrhythmia, especially atrial fibrillation in which ultrafast ventricular response rates may initiate ventricular fibrillation and sudden death. Diagnosis is clinical and by electrocardiography. Initial treatment of reentrant (paroxysmal) supraventricular tachycardia is usually with vagotonic maneuvers. If these maneuvers are ineffective, treatment is with IV adenosine or nondihydropyridine calcium channel blockers for regular narrow QRS rhythms or for regular wide QRS rhythms known to be a reentrant SVT with aberrant conduction. Procainamide or amiodarone are effective for irregular or other wide QRS rhythms. Synchronized cardioversion can be done when medications are ineffective or there is hemodynamic instability.Classic (manifest) Wolff-Parkinson-White syndrome is due to an accessory atrioventricular connection that produces a prototypical ECG consisting of a short PR interval, a wide QRS complex with an initial slurred component (delta wave), and secondary repolarization changes in association with symptomatic reentrant (paroxysmal) supraventricular tachycardia. Reentrant (paroxysmal) supraventricular tachycarida produces sudden episodes of palpitations that begin and terminate abruptly; some patients have dyspnea or chest discomfort. The accessory atrioventricular (AV) connection can facilitate very rapid ventricular response rates to any fast supraventricular arrhythmia, especially atrial fibrillation in which ultrafast ventricular response rates may initiate ventricular fibrillation and sudden death. Diagnosis is clinical and by electrocardiography. Initial treatment of reentrant (paroxysmal) supraventricular tachycardia is usually with vagotonic maneuvers. If these maneuvers are ineffective, treatment is with IV adenosine or nondihydropyridine calcium channel blockers for regular narrow QRS rhythms or for regular wide QRS rhythms known to be a reentrant SVT with aberrant conduction. Procainamide or amiodarone are effective for irregular or other wide QRS rhythms. Synchronized cardioversion can be done when medications are ineffective or there is hemodynamic instability.
(See also Overview of Arrhythmias and Atrioventricular Reentrant Tachycardia.)
Pathophysiology of WPW Syndrome
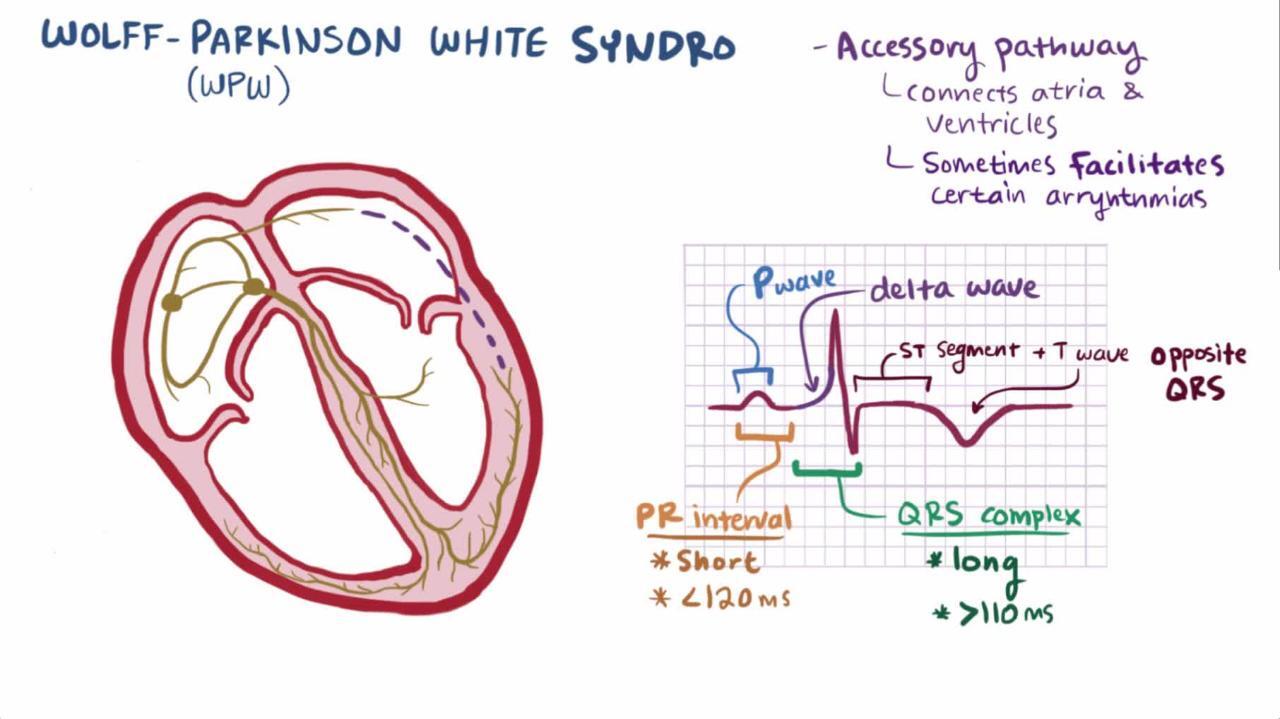
An accessory pathway connecting an atrium and a ventricle is the substrate for the Wolff-Parkinson-White syndrome. When the accessory AV connection conducts in the antegrade direction, the AV nodal delay is bypassed and a portion of ventricular myocardium is activated before the rest is activated by the normal conduction system. This ventricular pre-excitation produces a short PR interval (< 0.12 seconds), a wide QRS complex (≥ 0.12 seconds) with an initial slurred component (the delta wave) which, along with symptoms of paroxysmal tachycardia, define the classic (manifest) Wolff-Parkinson-White syndrome (1). Classic (manifest) Wolff-Parkinson-White syndrome occurs in about 1 to 3/1000 people ([2] sampled in Canadian men).
Depending on the orientation of the delta wave, a pseudoinfarction pattern Q-wave may be present. Because the early depolarized parts of the ventricle also repolarize early, the T-wave vector may be abnormal.
If the accessory AV connection can conduct in the retrograde direction, it can support a form of paroxysmal supraventricular tachycardia called orthodromic atrioventricular reentrant tachycardia. The accessory AV connection tends to have a longer refractory period at baseline heart rates than the AV node. At a premature atrial depolarization coupling interval less than the refractory period of the accessory AV pathway, but longer than the refractory period of the AV node, antegrade accessory AV pathway transmission is blocked but antegrade AV nodal conduction proceeds. The ECG shows a sudden increase in the PR interval and loss of the delta wave. When antegrade conduction through the AV node is sufficiently slow, it can find the distal accessory AV connection ready to conduct, but now in the retrograde (ventricle to atrium) direction. When this retrograde accessory AC connection transmission finds the atria and, subsequently, the AV node ready to conduct again in the antegrade direction, around-and-around atrioventricular reentry occurs. The ECG then shows a rapid, regular, tachycardia. This orthodromic atrioventricular tachycardia is the usual (95%) type of AV reentrant tachycardia (3).
Less commonly, and more often induced by a ventricular premature beat, the reentry occurs in the opposite direction (antidromic atrioventricular reentrant tachycardia). Since 5% of patients with an accessory AV connection have multiple accessory AV connections (4), it is also possible to have a dual accessory AV connection atrioventricular reentrant tachycardia that uses one accessory AV connection for antegrade conduction and another accessory AV connection for retrograde conduction.
The accessory atrioventricular connection in WPW syndrome behaves like atrial myocardium, a fast channel tissue, the refractory period of which shortens with increasing rates. Accordingly, should a rapid supraventricular rhythm occur, the ventricular response may not be controlled by the usual increased refractoriness of the AV node as the accessory AV connection may be able to conduct at very rapid rates. This is particularly relevant to the ventricular response rate to atrial fibrillation which may be sufficiently rapid as to produce hemodynamic compromise and may induce ventricular fibrillation and sudden death. Sudden death may be the first clinical manifestation of WPW syndrome, particularly in adolescence. In some patients with an accessory AV connection that conducts in the retrograde direction (and can, therefore, participate in orthodromic atrioventricular reentrant tachycardia) the accessory AV connection does not conduct in the antegrade direction. Such patients do not have the WPW pattern on their ECG and are said to have concealed WPW syndrome. They are not at risk of rapidly conducted supraventricular arrhythmias.
WPW syndrome is mainly idiopathic, although it is more common among patients with hypertrophic cardiomyopathy, transposition of the great vessels, or Epstein's anomaly.
Pathophysiology references
1. Bhatia A, Sra J, Akhtar M: Preexcitation Syndromes. Curr Probl Cardiol 41(3):99–137, 2016. doi: 10.1016/j.cpcardiol.2015.11.002
2. Krahn AD, Manfreda J, Tate RB, Mathewson FA, Cuddy TE: The natural history of electrocardiographic preexcitation in men. The Manitoba Follow-up Study. Ann Intern Med 116(6):456–460, 21992 doi: 10.7326/0003-4819-116-6-456
3. Page RL, Joglar JA, Caldwell MA, et al: 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society [published correction appears in J Am Coll Cardiol 2016 Dec 27;68(25):2922-2923. doi: 10.1016/j.jacc.2016.11.014]. J Am Coll Cardiol 67(13):e27–e115, 2016. doi: 10.1016/j.jacc.2015.08.856
4. Kadish A, Passman R: Mechanisms and management of paroxysmal supraventricular tachycardia. Cardiol Rev 7(5):254–264, 1999. doi: 10.1097/00045415-199909000-00009
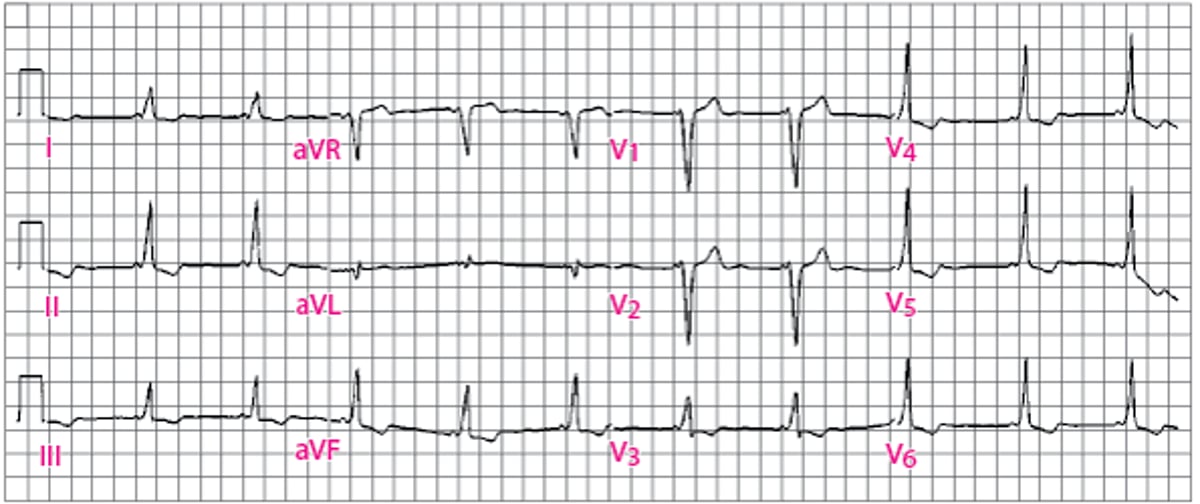
Classic Wolff-Parkinson-White (WPW) Pattern
Leads I, II, III, V3 through V6 show classic features of WPW syndrome, with a short PR interval and a delta wave during sinus rhythm. |

Symptoms and Signs of WPW Syndrome
Most patients present with symptoms of atrioventricular reentrant tachycardia during young adulthood or middle age. They typically have episodes of sudden-onset, sudden-offset, rapid, regular palpitations often associated with symptoms of hemodynamic compromise (eg, dyspnea, chest discomfort, light-headedness). Attacks may last only a few seconds or persist for several hours (rarely, > 12 hours). Syncope is uncommon but may occur. Infants present with episodic breathlessness, lethargy, feeding problems, or rapid precordial pulsations. If the episode of tachycardia is protracted, infants may present with heart failure.
Patients with WPW syndrome may also experience rapidly conducted supraventricular arrhythmias such as 1:1 conduction of atrial flutter or rapidly conducted atrial fibrillation wherein symptoms of hemodynamic compromise, including syncope are more common.
Rapidly conducted atrial fibrillation may also induce ventricular fibrillation and sudden death. This risk is low (approximately 1%) but is more likely to occur in adolescence.
Between episodes of arrhythmia, examination is normal.
Diagnosis of WPW Syndrome
Electrocardiography (ECG)
Diagnosis of WPW syndrome is by ECG showing a short PR interval (< 0.12 seconds), a wide QRS complex (≥ 0.12 seconds) with an initial slurred component (the delta wave), and secondary ST and T wave changes (see figure Classic Wolff-Parkinson-White (WPW) Pattern) (1). During the most common arrhythmia in WPW syndrome, orthodromic atrioventricular tachycardia, the ECG shows a rapid (120 to 250 beats/minute), regular, tachycardia. The QRS complex is usually narrow but may be wide (≥ 0.12 seconds) with coexistent bundle branch block. If found, the P-wave is in the first half of the RR interval (a short RP tachycardia), often in the ST segment or early T-wave, and is negative in the inferior leads (II, III, AVF) (see figure Narrow QRS Tachycardia: Orthodromic Atrioventricular Reentrant Tachycardia Using an Accessory AV Connection in Wolff-Parkinson-White Syndrome).
During antidromic atrioventricular reentrant tachycardia, the ECG shows a rapid (120 to 250 beats/minute), regular tachycardia. The QRS complex is wide (≥ 0.12 seconds) due to total ventricular preexcitation. When the accessory AV connection functions as a bystander conducting a supraventricular arrhythmia, the QRS complexes may show total ventricular preexcitation, intermittent total preexcitation mingled with normally conducted narrow QRS complexes, and/or variable degrees of fusion QRS complexes between the QRS complexes of total ventricular preexcitation and those of normal conduction.
Conduction of atrial fibrillation via the accessory AV connection in WPW syndrome can be very dangerous if antegrade conduction is very fast. Clues to the presence of pre-excited atrial fibrillation include a very rapid, dominantly wide QRS complex arrhythmia with the occasional occurrence of a narrow QRS complex that is not the result of a long proceeding RR interval. The QRS complex morphology may vary, but all QRS complexes are a fusion of that of the widest QRS complex and that of a normal narrow QRS complex. In pre-excited atrial fibrillation, the normal rate-limiting effects of the AV node are bypassed, and the resultant excessive ventricular rates (sometimes 200 to 300 beats/minutes) may lead to ventricular fibrillation (2). Risk factors for ventricular fibrillation in WPW syndrome include younger age, exercise, prior tachyarrhythmias, multiple accessory AV connections, presence of negative dromotropic medications (especially digitalis),and minimum RR interval during pre-excited atrial fibrillation ≤ 0.25 seconds (2). The estimated risk of developing atrial fibrillation in patients with WPW syndrome is 1.5%/year and that of sudden death is 0.1%/year (3).
Diagnosis references
1. Brugada J, Katritsis DG, Arbelo E, et al: 2019 ESC Guidelines for the management of patients with supraventricular tachycardia. The Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J 41(5):655-720, 2020. doi: 10.1093/eurheartj/ehz467
2. Klein GJ, Bashore TM, Sellers TD, Pritchett EL, Smith WM, Gallagher JJ: Ventricular fibrillation in the Wolff-Parkinson-White syndrome. N Engl J Med 301(20):1080–1085, 1979. doi: 10.1056/NEJM197911153012003
3. Brugada J, Keegan R: Asymptomatic Ventricular Pre-excitation: Between Sudden Cardiac Death and Catheter Ablation. Arrhythm Electrophysiol Rev 7(1):32–38, 2018. doi: 10.15420/aer.2017.51
Treatment of WPW Syndrome
Acute: treatment of the presenting arrhythmia
Long-term: chronic antiarrhythmic therapy for arrhythmia prevention or ablation of the accessory AV connection
Acute
When a patient with WPW syndrome presents with a rapid, regular, narrow QRS complex tachycardia, the mechanism of the tachycardia is almost always orthodromic atrioventricular reentrant tachycardia and may be treated as any other regular, narrow QRS complex tachycardia (see Reentrant (Paroxysmal) Supraventricular Tachycardia (PSVT) ). Vagal maneuvers are attempted first.
If the patient is hemodynamically unstable or unresponsive to other medical therapies, synchronized DC cardioversion is used. For hemodynamically stable patients, IV adenosine is preferred. If unresponsive to IV adenosine, United States guidelines recommend a class IIb such as an IV beta blocker, IV diltiazem, or IV verapamil (If the patient is hemodynamically unstable or unresponsive to other medical therapies, synchronized DC cardioversion is used. For hemodynamically stable patients, IV adenosine is preferred. If unresponsive to IV adenosine, United States guidelines recommend a class IIb such as an IV beta blocker, IV diltiazem, or IV verapamil (1). This class IIb recommendation in patients with known WPW syndrome (rather than the class IIa recommendation in the setting of other causes of PSVT) recognizes the rare possibility that the PSVT will terminate to pre-excited atrial fibrillation with a more rapid ventricular response rate because of the presence of one of these medications. Alternatively, synchronized DC cardioversion is performed.
When a patient with WPW syndrome presents with a rapid, regular, wide QRS complex tachycardia the possibilities include orthodromic atrioventricular reentrant tachycardia with bundle branch block, antidromic atrioventricular reentrant tachycardia, dual accessory connection atrioventricular tachycardia, accessory AV connection of another supraventricular arrhythmia (atrial tachycardia, atrial flutter, or atrioventricular nodal reentrant tachycardia), or ventricular tachycardia. Synchronized cardioversion is used if hemodynamic instability is present. If stable and vagal maneuvers are unsuccessful, therapy with IV procainamide, IV amiodarone, or synchronized cardioversion is recommended (When a patient with WPW syndrome presents with a rapid, regular, wide QRS complex tachycardia the possibilities include orthodromic atrioventricular reentrant tachycardia with bundle branch block, antidromic atrioventricular reentrant tachycardia, dual accessory connection atrioventricular tachycardia, accessory AV connection of another supraventricular arrhythmia (atrial tachycardia, atrial flutter, or atrioventricular nodal reentrant tachycardia), or ventricular tachycardia. Synchronized cardioversion is used if hemodynamic instability is present. If stable and vagal maneuvers are unsuccessful, therapy with IV procainamide, IV amiodarone, or synchronized cardioversion is recommended (1).
When a patient with classic (manifest) WPW syndrome presents with atrial fibrillation, at least some of the QRS complexes are expected to show ventricular pre-excitation. When most or all of the QRS complexes show ventricular pre-excitation, the ventricular response rate may be very fast. If hemodynamically unstable, synchronized DC cardioversion is used. If hemodynamically stable, IV ibutilide, IV procainamide, or synchronized DC cardioversion is recommended (When a patient with classic (manifest) WPW syndrome presents with atrial fibrillation, at least some of the QRS complexes are expected to show ventricular pre-excitation. When most or all of the QRS complexes show ventricular pre-excitation, the ventricular response rate may be very fast. If hemodynamically unstable, synchronized DC cardioversion is used. If hemodynamically stable, IV ibutilide, IV procainamide, or synchronized DC cardioversion is recommended (1).
Long-term
Long-term therapy of patients who have had a documented WPW syndrome-related tachyarrhythmia (or symptoms highly suggestive thereof) is with catheter ablation of the accessory AV connection(s) (1). A meta-analysis of ablation in WPW syndrome reports a success rate of 94%, a recurrence rate of 6% (usually treated by re-ablation), and a procedure-related complication rate of 1% (2). If ablation cannot be performed or if the patient declines ablation, medical therapy may be accomplished with almost any oral antiarrhythmic medication other than digoxin. Class IIa recommendations are given for oral flecainide or oral propafenone in the absence of a structural heart disorder (). If ablation cannot be performed or if the patient declines ablation, medical therapy may be accomplished with almost any oral antiarrhythmic medication other than digoxin. Class IIa recommendations are given for oral flecainide or oral propafenone in the absence of a structural heart disorder (1). Class IIb recommendations are given for oral dofetilide, oral sotalol, and oral amiodarone (). Class IIb recommendations are given for oral dofetilide, oral sotalol, and oral amiodarone (1). Although a class IIb recommendation is given for oral beta blockers (especially useful if symptoms occur with exercise), oral diltiazem, or oral verapamil, there is a small possibility that these mediations could be harmful should atrial fibrillation ever occur.). Although a class IIb recommendation is given for oral beta blockers (especially useful if symptoms occur with exercise), oral diltiazem, or oral verapamil, there is a small possibility that these mediations could be harmful should atrial fibrillation ever occur.
Treatment references
1. Page RL, Joglar JA, Caldwell MA, et al: 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society [published correction appears in J Am Coll Cardiol 2016 Dec 27;68(25):2922-2923. doi: 10.1016/j.jacc.2016.11.014]. J Am Coll Cardiol 2016 Apr 5;67(13):e27–e115, 2016. doi: 10.1016/j.jacc.2015.08.856
2. Ibrahim Ali Sherdia AF, Abdelaal SA, Hasan MT, et al: The success rate of radiofrequency catheter ablation in Wolff-Parkinson-White-Syndrome patients: A systematic review and meta-analysis. Indian Heart J 75(2):98–107, 2023. doi: 10.1016/j.ihj.2023.02.001
Key Points
Wolff-Parkinson-White (WPW) syndrome is characterized by a short PR interval, a wide QRS complex with an initial slurred component (delta wave), and secondary repolarization changes in association with symptomatic reentrant (paroxysmal) supraventricular tachycardia.
Episodes of reentrant supraventricular tachycardia underlie symptoms of palpitations, chest pain, and sometimes syncope. In patients with WPW syndrome who develop atrial fibrillation, excessively rapid ventricular response rates can lead to ventricular fibrillation and sudden death.
Acute treatment of WPW-related tachycardia in unstable patients is with synchronized DC cardioversion; treatment of stable patients with regular, narrow QRS complex tachycardia is IV adenosine or alternatively parenteral antiarrhythmics. Acute treatment of WPW-related tachycardia in unstable patients is with synchronized DC cardioversion; treatment of stable patients with regular, narrow QRS complex tachycardia is IV adenosine or alternatively parenteral antiarrhythmics.
Long-term treatment is with catheter ablation of the accessory pathway; oral antiarrhythmics can be used if ablation cannot be performed.







