



Cholestasis is a reduction of bile formation or bile flow. As a result, bilirubin backs up into the bloodstream (hyperbilirubinemia), leading to a yellow to yellow-green discoloration of the whites of the eyes and skin called jaundice.
Topic Resources

Cholestasis has numerous causes, including infections, metabolic problems, genetic defects, and blockages.
The most common symptoms are jaundice and dark urine.
The diagnosis is made by blood tests, imaging tests, and sometimes liver biopsy.
Treatment depends on the cause.
Bilirubin is a yellow substance formed when hemoglobin (the part of red blood cells that carries oxygen) is broken down as part of the normal process of recycling old or damaged red blood cells.
Bilirubin is carried in the bloodstream to the liver and processed so that it can be excreted out of the liver as part of bile (the digestive fluid produced by the liver). Bilirubin processing in the liver involves attaching it to another chemical substance in a process called conjugation.
Processed bilirubin in the bile is called conjugated bilirubin.
Unprocessed bilirubin is called unconjugated bilirubin.
Bile is transported through the bile ducts into the beginning of the small intestine (duodenum). If bilirubin cannot be processed and excreted by the liver and bile ducts quickly enough, it builds up in the blood (hyperbilirubinemia). The excess bilirubin settles in the skin, the whites of the eyes, and other tissues, causing them to turn yellow (jaundice).
In cholestasis, the liver cells process bilirubin properly, but the excretion of bile is impaired at some point between the liver cells and the duodenum. This results in an increase in conjugated bilirubin in the blood and a decrease in bile delivered to the small intestine.
Another effect of bile not being excreted normally into the small intestine is that digestion is impaired. Bile is important for digestion because it helps the body absorb fats and the fat-soluble vitamins A, D, E, and K. When there is not enough bile in the intestine, fat absorption is impaired, which can lead to vitamin deficiency, inadequate nutrition, and a failure to grow and gain weight.
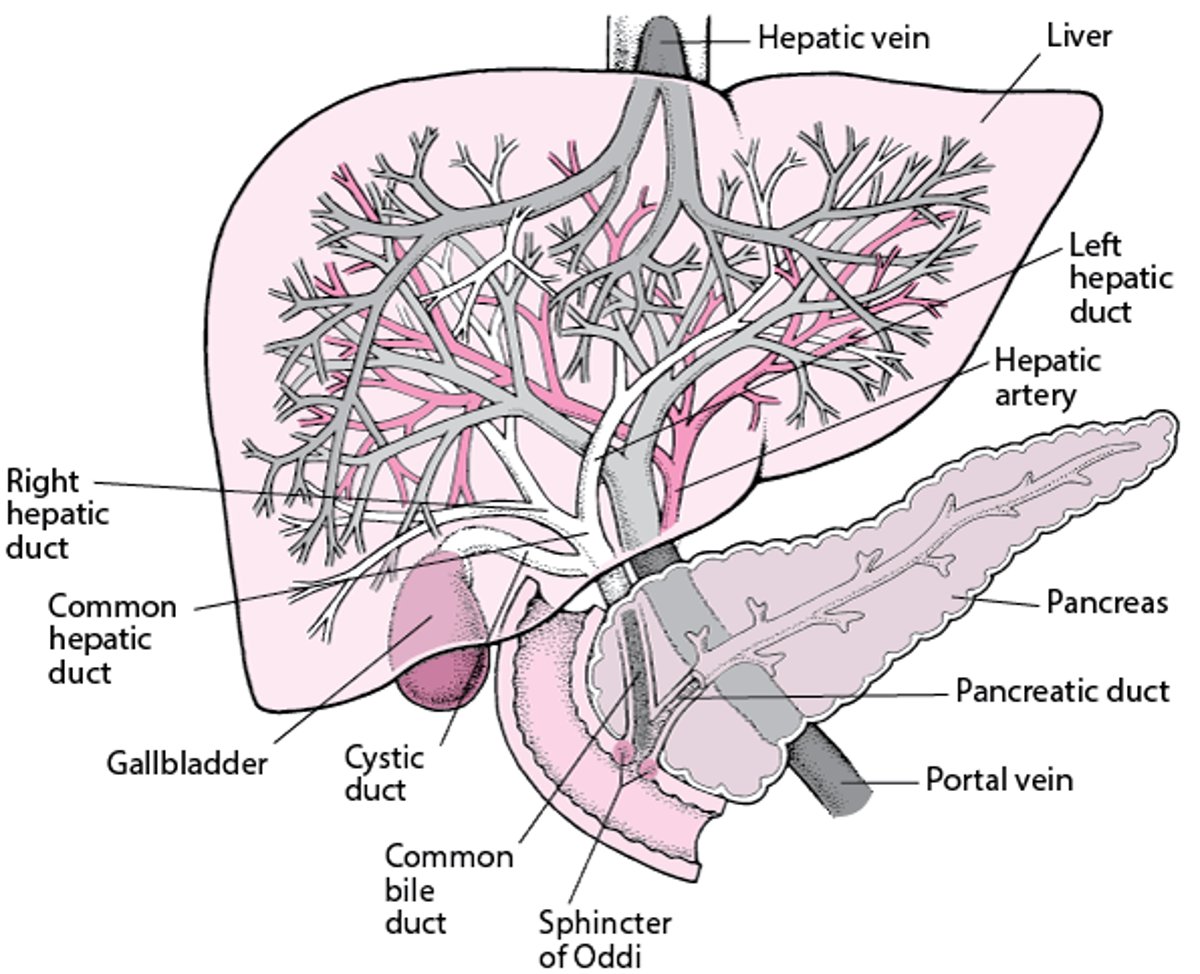
View of the Liver

Causes of Cholestasis in Newborns
Cholestasis in the newborn can be caused by
Biliary atresia (blockage of the bile ducts)
Biliary cysts
Infection
An immune disorder
Metabolic disorders
Genetic defects
Toxic causes
Biliary atresia is a blockage of the bile ducts that starts in the fetus near the end of the pregnancy or in the first several weeks of life. It is more common among full-term infants than premature infants or newborns. Affected infants typically develop jaundice in the first several weeks of life.
Biliary cysts or bile duct cysts are enlargements of parts of the bile ducts. These rare cysts are typically caused by a birth defect in the area where the bile duct and the pancreatic duct meet (see figure View of the Liver). Biliary cysts are more common among infants who have polycystic kidney disease (PKD). PKD is an inherited disorder that causes cysts to form in the kidneys.
Infections can lead to cholestasis in the newborn. Some infecting organisms are
Viruses: Including cytomegalovirus, herpes simplex virus, and rubella
Bacteria: Most often urinary tract infection and/or bloodstream infection (sepsis) caused by Escherichia coli or group B streptococcus
Parasites: Including toxoplasmosis
Gestational alloimmune liver disease is a disorder that begins before birth. In this disease, antibodies from the mother cross the placenta and attack the fetus's liver.
Metabolic disorders that cause cholestasis are numerous and include alpha-1 antitrypsin deficiency, galactosemia, tyrosinemia, bile acid defects, and fatty acid oxidation disorders. These disorders occur when the newborn is missing an enzyme that is needed to break down a certain substance, allowing toxic substances to accumulate and damage the liver.
Genetic defects, such as Alagille syndrome and cystic fibrosis, may cause cholestasis in the newborn. Genetic defects and other gene mutations can disrupt normal bile production and removal, which causes cholestasis.
Toxic causes include the use of intravenous feeding (parenteral nutrition) in extremely premature newborns or in infants who have short bowel syndrome. In recent years, centers have begun using a different type of fat in the intravenous formulation, which appears to have reduced the risk of cholestasis.
Neonatal hepatitis syndrome is the term used to describe inflammation in the newborn's liver for which there is no identified cause. This diagnosis is being made less frequently due to advances in tests that can determine an exact cause.
Symptoms of Cholestasis in Newborns
Symptoms of cholestasis typically develop during the first 2 weeks of a newborn's life. Infants with cholestasis have jaundice and often have dark urine, light-colored stools, and/or an enlarged liver. Bilirubin in the skin can cause itching, which makes infants irritable.
Because infants with cholestasis may not properly absorb fats and vitamins, they may not grow well.
Other problems, such as abdominal swelling caused by fluid in the abdomen (ascites) and bleeding in the upper digestive tract caused by enlarged veins in the esophagus (esophageal varices), may develop as liver disease progresses.
Diagnosis of Cholestasis in Newborns
Blood tests
Imaging tests
Sometimes biopsy of the liver
Almost all newborns have higher bilirubin levels in their blood (hyperbilirubinemia) during the first week of life than they do later on. This normal jaundice (physiologic jaundice) resolves over a week or two, and the bilirubin level returns to normal.
If infants still have jaundice after 2 weeks of age, doctors test the blood to see if the elevated bilirubin is conjugated or unconjugated. A high level of conjugated bilirubin indicates liver dysfunction and possible cholestasis. A high level of unconjugated bilirubin is not caused by liver dysfunction. If the test indicates cholestasis is present, infants have additional blood tests to determine if the liver is inflamed or not functioning normally (see Liver Blood Tests). Doctors do other tests to determine the cause of cholestasis.
Doctors do ultrasonography of the abdomen to assess the size of the liver and view the gallbladder and major bile duct. In another type of imaging test called cholescintigraphy (hepatobiliary scintigraphy or scan), doctors inject a radioactive substance into the infant's vein. They then follow the movement of the radioactive substance as it is secreted from the liver and passes into the gallbladder and through the bile ducts into the duodenum. Another type of x-ray test that allows doctors to view the bile ducts and gallbladder, called endoscopic retrograde cholangiopancreatography (ERCP), is sometimes done at specialized medical centers.
If doctors cannot diagnose the cause, they remove a sample of the infant's liver for further evaluation (biopsy). The biopsy may be done with or without operative cholangiography, which involves the injection of a substance that can be seen on x-rays directly into the gallbladder to better determine if the bile ducts are normal.
Treatment of Cholestasis in Newborns
Treatment of the specific cause
Supportive care, including good nutrition
Treatment of the cause
Infants who have biliary atresia are treated with a surgical procedure called portoenterostomy (Kasai procedure). Ideally, this procedure should be done in the first 1 to 2 months of life. During this procedure, a part of the small intestine is attached to an area of the liver so that bile can drain into the small intestine. Even with this procedure and optimal care, most infants ultimately require a liver transplant.
Some metabolic disorders such as galactosemia can be treated. Galactosemia is treated by eliminating milk and milk products (which contain the sugar galactose) from the infant's diet. Typically, infants are given a soy formula.
Infants who have gestational alloimmune liver disease may be treated with immune globulin (antibodies obtained from the blood of people with a normal immune system) given by vein or by withdrawing a large amount of the infant's blood and replacing it with transfused blood (exchange transfusion).
Supportive care
It is important to promote good nutrition and give supplements for any deficiencies in vitamins A, D, E, and K. Infants with cholestasis typically do not absorb fat well, so using formulas that contain specialized fat (medium-chain triglycerides) improves their fat absorption and growth. Some infants are not able to drink enough formula to achieve normal growth and may need a concentrated formula that contains more calories per ounce.
Infants who do not have biliary atresia may be given ursodeoxycholic acid to relieve itching, increase bile flow, and improve their liver disease.
Prognosis for Cholestasis in Newborns
Prognosis varies greatly. Depending on the cause, infants may recover completely or develop liver failure or cirrhosis of the liver (scarring of the liver).
Biliary atresia can result in progressively worsening liver disease even if it is appropriately diagnosed and treated. Infants who are not treated, frequently die of liver failure by 1 year of age.
Cholestasis caused by intravenous nutrition will correct itself if the intravenous nutrition is stopped before the infant develops severe liver disease. If intravenous nutrition cannot be stopped, a different formulation containing fish oil can be used to relieve the cholestasis.Cholestasis caused by intravenous nutrition will correct itself if the intravenous nutrition is stopped before the infant develops severe liver disease. If intravenous nutrition cannot be stopped, a different formulation containing fish oil can be used to relieve the cholestasis.
Gestational alloimmune liver disease that is not treated early typically has a poor prognosis.







