



Bronchiectasis is an irreversible widening (dilation) and thickening of portions of the breathing tubes or airways (bronchi) resulting from damage to the airway wall.






The most common cause is severe or repeated respiratory infections, often in people who have an underlying problem with their lungs or immune system.
Most people develop a chronic cough that often results in mucus production, and some also cough up blood and have chest pain and recurrent episodes of pneumonia.
Chest x-rays, computed tomography, and breathing tests are usually done to determine the extent and severity of the disorder.
People often are given inhaled medications, antibiotics, and other measures to suppress and clear the buildup of mucus.
Bronchiectasis can result when conditions:
Directly injure the bronchial wall
Indirectly lead to injury by interfering with normal airway defenses
Airway defenses include the mucus layer and tiny projections (cilia) on the cells that line the airways. These cilia beat back and forth, moving the thin liquid layer of mucus that normally coats the airways. Harmful particles and bacteria trapped in this mucus layer are moved up to the throat and coughed out or swallowed.

Whether airway injury is direct or indirect, areas of the bronchial wall are damaged and become chronically inflamed. The inflamed bronchial wall becomes less elastic, resulting in the affected airways becoming widened (dilated) and developing small outpouchings, or sacs, that resemble tiny balloons. Inflammation also increases secretions (mucus). Because cells with cilia are damaged or destroyed, these secretions accumulate in the widened airways and serve as a breeding ground for bacteria. The bacteria further damage the bronchial wall, leading to a vicious cycle of infection and airway damage.
Understanding Bronchiectasis
In bronchiectasis, mucus production increases, the cilia are destroyed or damaged, and areas of the bronchial wall become chronically inflamed and are destroyed. |

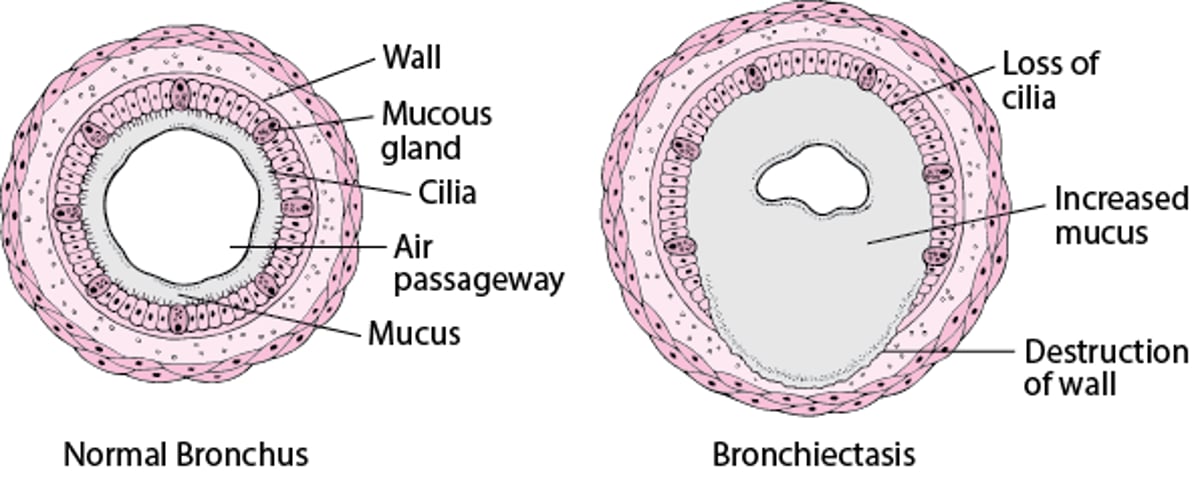
Bronchiectasis may affect many areas of the lung (diffuse bronchiectasis), or it may appear in only one or two areas (focal bronchiectasis). Typically, bronchiectasis causes widening of medium-sized airways, but often smaller airways become scarred and destroyed.
Complications
The inflammation and infection can extend to the small air sacs of the lungs (alveoli) and cause pneumonia, scarring, and a loss of functioning lung tissue (see also Overview of the Respiratory System). Severe scarring and loss of lung tissue can ultimately strain the right side of the heart as it tries to pump blood through the altered lung tissue. The right-sided heart strain can lead to a form of heart failure called cor pulmonale.
Very severe (advanced) cases of bronchiectasis occur more commonly in people who have advanced cystic fibrosis and, in areas where people live in crowded conditions and/or lack access to medical care, those with tuberculosis. Very severe bronchiectasis may impair breathing enough to cause abnormally low levels of oxygen and/or high levels of carbon dioxide in the blood, a condition called chronic respiratory failure.
Causes of Bronchiectasis
The most common cause of bronchiectasis is severe or repeated respiratory infections, which are particularly likely to occur in people who have one or more of the following:
Other hereditary disorders, such as primary ciliary dyskinesia, in which the ability to clear the airways is impaired
Certain autoimmune disorders, such as rheumatoid arthritis, ulcerative colitis, or Sjögren syndrome
Mechanical factors, such as airway blockage caused by an inhaled object, chronically enlarged lymph nodes, changes after lung surgery, or a lung tumor
Inhaling toxic substances that injure the airways, such as noxious fumes, gases, smoke (including tobacco smoke), and injurious dust (for example, silica and coal dust)
Allergic bronchopulmonary aspergillosis, which affects the larger airways, can cause plugs of mucus that block the airways and lead to bronchiectasis. It is an allergic reaction to the fungus Aspergillus and occurs most commonly in people with asthma or cystic fibrosis.
Bronchiectasis may also accompany common conditions such as chronic obstructive pulmonary disease (COPD) or result from chronic aspiration, which refers to the possibility of inhaling things that normally go down the food pipe (esophagus) through the windpipe (trachea and bronchus), both of which cause chronic inflammation.
In places where tuberculosis is common, tuberculosis is often the cause of severe or repeated infections that cause bronchiectasis. Poor nutrition and unavailability of vaccines to prevent various respiratory infections can also contribute.
In many people with bronchiectasis, a cause cannot be determined despite a thorough evaluation.
Symptoms of Bronchiectasis
Bronchiectasis can develop at any age. In most people, symptoms begin gradually, usually after a respiratory infection, and tend to worsen over the years. Most people develop a chronic cough that produces thick sputum. The amount and type of sputum depend on the extent of the disease and whether there is a complicating infection (often called a disease flare or exacerbation). Often, people have coughing spells only early in the morning and late in the day.
Coughing up of blood (hemoptysis) is common because the damaged airway walls are fragile and have increased numbers of blood vessels. Hemoptysis may be the first or only symptom.
Recurrent fever or chest pain, with or without frequent bouts of pneumonia, may also occur. People with widespread bronchiectasis may develop wheezing or shortness of breath. People whose bronchiectasis progresses to cor pulmonale or chronic respiratory failure also have fatigue, lethargy, and worsening shortness of breath, particularly during exertion. If bronchiectasis is severe and chronic, people commonly lose weight.
People may have flares (exacerbations) of disease, sometimes with pneumonia. Exacerbations may result from a new or worsening infection. When an exacerbation occurs, people may have more severe cough, increased sputum production, or worsening of breathing difficulties.
Diagnosis of Bronchiectasis
Chest x-ray
Computed tomography
Pulmonary function tests
Specific tests for suspected causes
Doctors may suspect bronchiectasis because of a person’s symptoms or the presence (currently or in the past) of a condition thought to cause bronchiectasis.
Tests are done to:
Confirm the diagnosis
Assess the extent of the disease
Identify the cause of the disease
Chest x-rays can often detect the lung changes caused by bronchiectasis. However, occasionally, x-ray results can be normal. Computed tomography (CT) is the most accurate test to identify and confirm the diagnosis and to determine the extent and severity of the disease.
Pulmonary function tests are done to assess how well the lungs are working. These tests measure how well the lungs are able to hold air, to move air in and out, and to exchange oxygen and carbon dioxide. Pulmonary function tests do not diagnose bronchiectasis but can help doctors determine how severe the lung disorder is and are useful for monitoring its progression over time.
After bronchiectasis is diagnosed, tests are often done to check for disorders that may be causing or contributing to it. Such tests may include the following:
Testing for human immunodeficiency virus (HIV) infection, immunoglobulin (antibody levels), and other immune system and autoimmune disorders
Measuring the salt level in sweat (which is abnormal in people with cystic fibrosis)
Testing nasal, bronchial, or sputum specimens for evidence of infectious organisms
Doing other tests to determine if the cilia are structurally or functionally defective
Testing for allergic bronchopulmonary aspergillosis, tuberculosis, and alpha-1 antitrypsin deficiency
When bronchiectasis is limited to one area—for example, a lung lobe or segment—doctors may do a bronchoscopy to determine whether an inhaled foreign object or lung tumor is the cause.
Sweat chloride tests and genetic testing for cystic fibrosis may be needed when there is a family history, repeated respiratory infections, or other unusual findings in a child or adult, even when other typical features of cystic fibrosis are absent.

Doctors will take a sputum sample and send it to a laboratory to grow (culture) the bacteria to determine which bacteria are present and what antibiotics are most effective against these bacteria. This testing can help determine the best antibiotics to use during flares.

Treatment of Bronchiectasis
Vaccination to prevent infections that cause or worsen bronchiectasis
Antibiotics to treat infections that cause or worsen bronchiectasis
Drainage of airway secretions with therapies that promote cough (such as, chest physical therapy, regular exercise, other techniques)
Inhaled medications that help thin or loosen thick mucus so it can be more easily coughed out
Inhaled bronchodilators and very rarely, inhaled corticosteroids
Sometimes, oral or inhaled antibiotics to suppress certain bacteria and prevent recurring infections
Rarely, surgical removal of part of lung
Oxygen therapy, if needed
Treatment of bronchiectasis is directed toward reducing the frequency of infections when possible, preventing certain infections with vaccines and sometimes antibiotics, decreasing the buildup of mucus, decreasing inflammation, and relieving airway blockage. Early, effective treatment can reduce complications such as hemoptysis, low oxygen levels in the blood, respiratory failure, and cor pulmonale. Treatment of underlying conditions that cause or contribute to flares is also needed.
Flares (exacerbations) are treated with antibiotics, bronchodilators, and chest physiotherapy to promote drainage of secretions and mucus. Chest physiotherapy includes such techniques as postural drainage and chest percussion. Sometimes antibiotics are given for a long period to prevent recurring infections, especially in people who have frequent flares or cystic fibrosis. Most people with cystic fibrosis benefit from treatment with a cystic fibrosis transmembrane regulator (CFTR) modulator, which can decrease exacerbations.
Did You Know...
|
Inflammation and the buildup of mucus may be helped by humidification of the air and inhaling an aerosolized salt water solution. Medications that thin the thick sputum (mucolytics) may also be given to people who have cystic fibrosis. In other people, the effectiveness of mucolytics is uncertain.
Bronchial blockage can be detected and treated by bronchoscopy before severe damage occurs.
Significant bleeding with cough is sometimes treated with a technique called embolization instead of surgery. In embolization, doctors use a catheter to inject a substance that blocks the vessel that is bleeding.
Low blood oxygen levels are treated with oxygen therapy. Appropriate use of oxygen may help prevent complications such as cor pulmonale. If people have wheezing or shortness of breath, bronchodilators and sometimes inhaled corticosteroids often help. If a person has a flare, usually these medications and an antibiotic are given, and oral corticosteroids are added in some cases. Respiratory failure, if present, should be treated.
Rarely, part of a lung needs to be surgically removed. Such surgery usually is an option only if the disease is confined to one lung or, preferably, to one lung lobe or segment. Surgery may be considered for people who have recurrent infections despite treatment or who cough up large amounts of blood.
Advanced bronchiectasis in some people—mostly those who also have advanced cystic fibrosis—can be treated with lung transplantation. Pulmonary function (as measured by the amount of air in the lungs and the rate and amount of air moving in and out of the lungs with each breath) usually improves within 6 months, and the improvement may be sustained for at least 5 years.
Prognosis for people with bronchiectasis depends on its cause and on how well infections and other complications are prevented or controlled. People with coexisting conditions, such as chronic bronchitis or emphysema, and people who have complications, such as pulmonary hypertension or cor pulmonale, tend to have a worse prognosis.
Prevention of Bronchiectasis
Early identification and treatment of conditions that tend to cause bronchiectasis may prevent its development or reduce its severity.
Childhood immunizations against measles and pertussis (whooping cough), improved living conditions, and better nutrition have markedly reduced the number of people who develop bronchiectasis. Pneumococcal vaccination, COVID-19 vaccination, respiratory syncytial virus (RSV) vaccination in some people, annual influenza vaccination, and use of appropriate antibiotics early in the course of lung infections help to prevent bronchiectasis or reduce its severity.
Other specific steps that can be taken include the following:
Receiving immunoglobulin for an immunoglobulin deficiency syndrome may prevent recurring infections.
In people who have allergic bronchopulmonary aspergillosis, using corticosteroids appropriately—and sometimes an antifungal medication (such as itraconazole)—may reduce the bronchial damage that results in bronchiectasis. In people who have allergic bronchopulmonary aspergillosis, using corticosteroids appropriately—and sometimes an antifungal medication (such as itraconazole)—may reduce the bronchial damage that results in bronchiectasis.
Giving the enzyme alpha-1 antitrypsin to people with alpha-1 antitrypsin deficiency may help prevent the disorder from becoming more severe.
Avoiding toxic fumes, gases, cigarette and other smoke, and injurious dusts also helps prevent bronchiectasis or reduce its severity.
Watching what children put in their mouth can help prevent them from inhaling foreign objects into the airways.
Avoiding oversedation due to medication, illicit drugs, or alcohol and seeking medical care for neurologic symptoms (such as impaired consciousness) or gastrointestinal symptoms (such as difficulty in swallowing and regurgitation or coughing after eating) may help to prevent aspiration.
Avoiding use of mineral oil or petroleum jelly in the nose may prevent accidental inhalation of these substances into the lungs.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
American Lung Association: Bronchiectasis: Complete discussion of symptoms, diagnosis, and treatment, and tips on questions to discuss with the doctor
National Heart. Lung, and Blood Institute: Bronchiectasis: Complete discussion of symptoms, diagnosis, and treatment, and tips on questions to discuss with the doctor







