




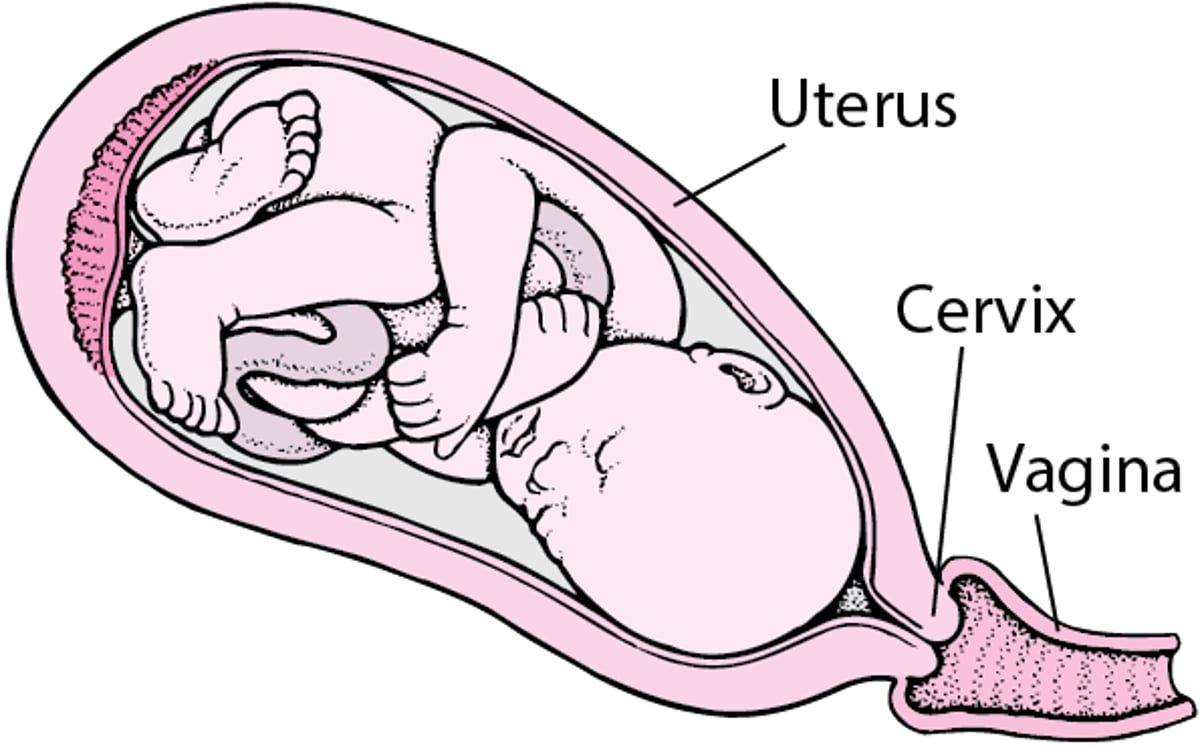
Labor is a series of rhythmic, progressive contractions of the uterus that gradually move the fetus through the lower part of the uterus (cervix) and birth canal (vagina).

(See also Overview of Labor and Delivery.)
Labor occurs in three main stages:
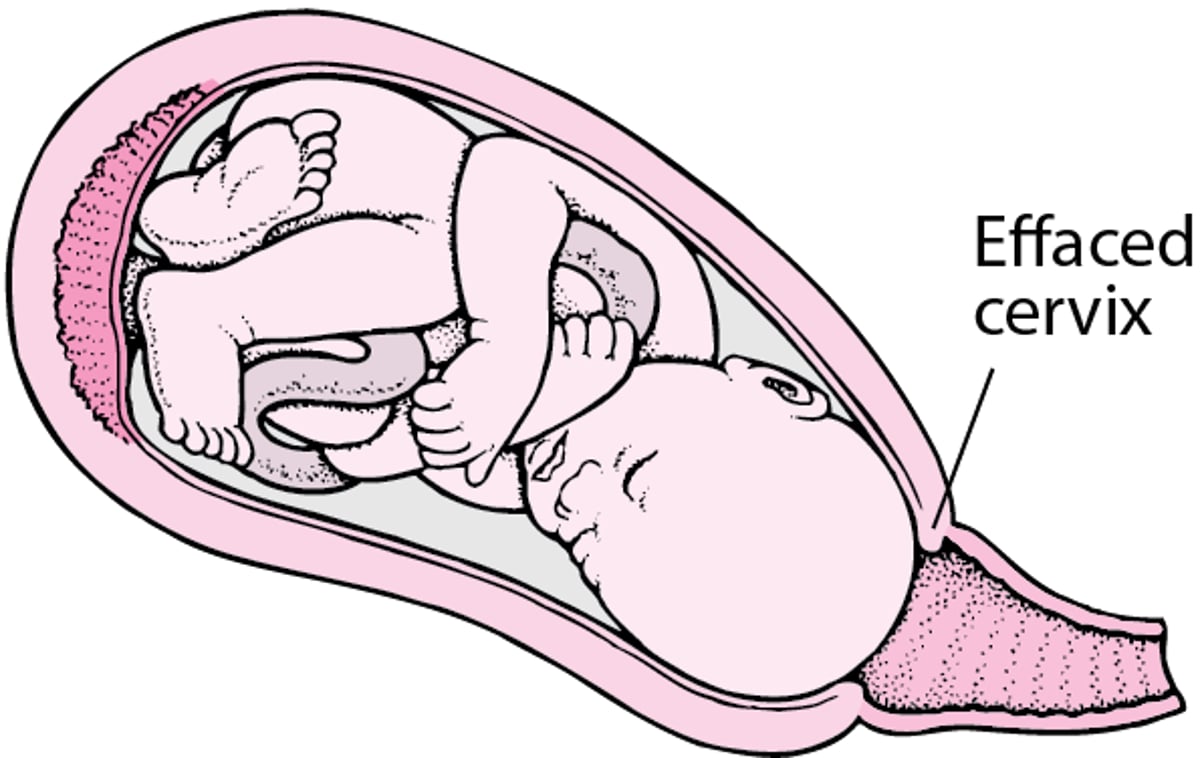
First stage: This stage (which has two phases: latent and active) is usually the longest stage. Labor officially begins when there are strong and regular uterine contractions that cause the cervix to open gradually (dilate) and to thin and pull back (efface) until it is fully dilated, and the baby is able to pass into the vagina.
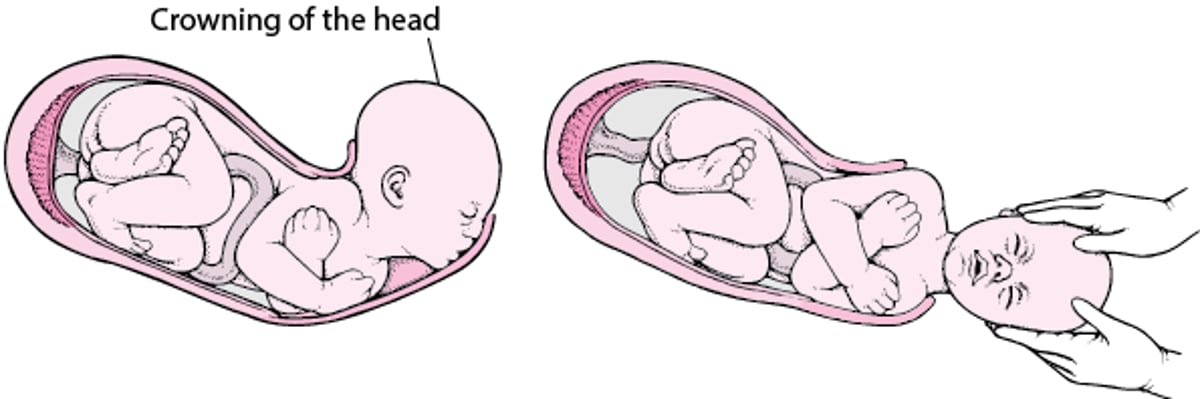
Second stage: The mother pushes and the baby is delivered.
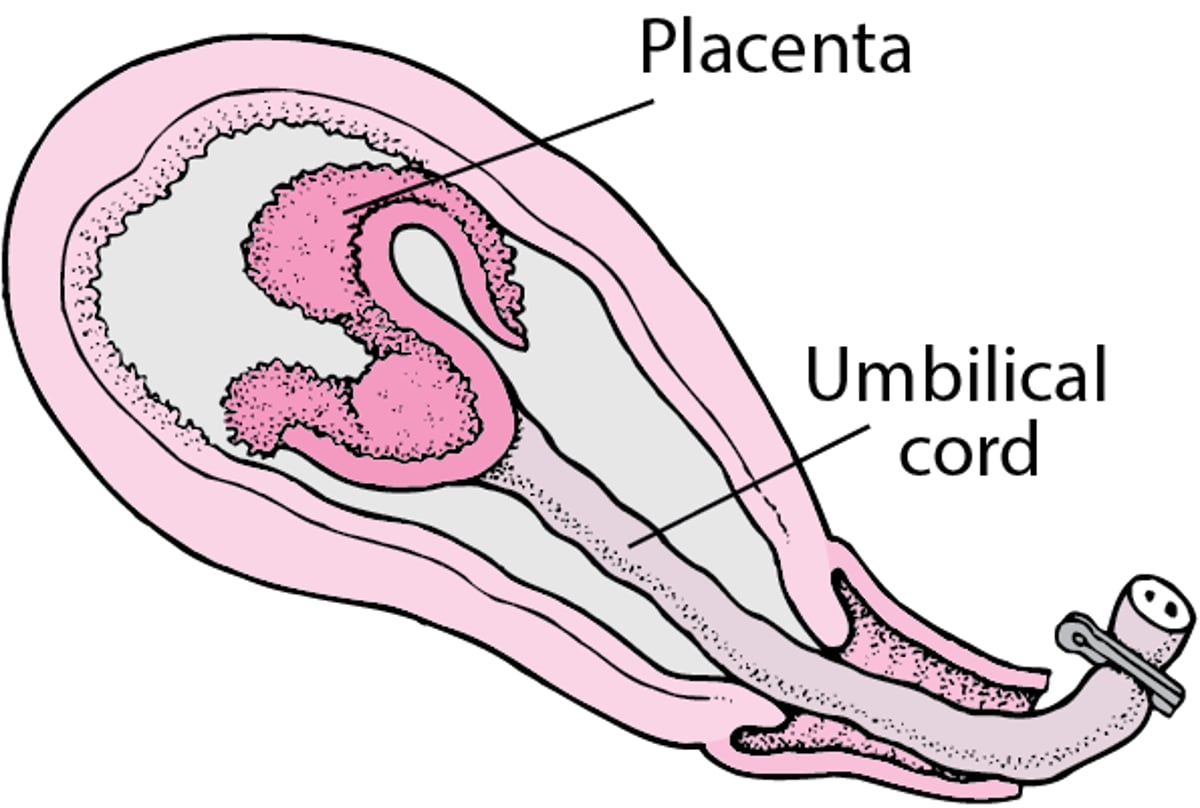
Third stage: The placenta (an organ that develops inside the uterus to provide oxygen and nutrients to the baby) is delivered. This stage is also called "the afterbirth."
Labor usually starts within 2 weeks of (before or after) the estimated date of delivery. Exactly what causes labor to start is unknown. Toward the end of pregnancy (after 37 weeks), a doctor examines the cervix to try to predict when labor will start.
On average, labor lasts 12 to 18 hours in a woman’s first pregnancy and tends to be shorter, averaging 6 to 8 hours, in subsequent pregnancies. Standing and walking during the first stage of labor can help manage pain and can potentially shorten labor by more than 1 hour.
Stages of Labor
FIRST STAGE | |
From the beginning of labor to the full opening (dilation) of the cervix—to about 10 centimeters. | |
Initial (Latent) Phase
| |
Active Phase
| |
SECOND STAGE | |
From the complete opening of the cervix to birth of the baby: This stage usually lasts about 2 hours in a first pregnancy and about 1 hour in subsequent pregnancies. It may last another hour or more if the woman has been given an epidural injection to relieve pain. During this stage, the woman pushes. | |
THIRD STAGE | |
From birth of the baby to delivery of the placenta: This stage usually lasts only a few minutes but may last up to 30 minutes. | |




Start of labor
Labor usually begins with
Contractions in the lower abdomen at regular intervals
Sometimes back pain
A woman who has had rapid deliveries in previous pregnancies should notify her doctor as soon as she thinks she is going into labor. When contractions in the lower abdomen first start, they may be weak, irregular, and far apart. They may feel like menstrual cramps. As time passes, uterine contractions become longer, stronger, and closer together. Contractions and back pain may be preceded or accompanied by other signs of labor, such as the following:
Bloody show: A small discharge of blood mixed with mucus (passing the "mucus plug") from the vagina may be an early sign that labor is about to start. However, bloody show may also occur as a result of sexual intercourse. The bloody show may appear as early as 72 hours before contractions start. Pregnant women should contact their healthcare professional if any vaginal bleeding occurs, because an evaluation at a doctor's office or hospital may be needed.
Rupture of membranes: Usually, the fluid-filled membranes that contain the fetus (amniotic sac) rupture during labor, and the amniotic fluid flows out through the vagina. This event is commonly described as “the water breaks.” Occasionally, the membranes rupture before labor starts. Rupture of membranes before labor begins is called prelabor rupture of membranes. Some women feel a gush of fluid from the vagina, followed by steady leaking. Sometimes it is difficult to know if the leaking fluid is amniotic fluid, urine, or vaginal discharge.
If a woman’s membranes rupture, she should contact her doctor or midwife immediately. About 80 to 90% of women whose membranes rupture at or near their due date go into labor spontaneously within 24 hours. If labor has not started after several hours and the baby is due, women are usually admitted to the hospital, where labor is artificially started (induced) to reduce the risk of infection. After the membranes rupture, bacteria from the vagina can enter the uterus more easily and cause an infection in the woman, the fetus, or both.
After a woman with prelabor rupture of membranes is admitted to a birthing center, oxytocin (which causes the uterus to contract) or a similar medication, such as a prostaglandin, is used to induce labor. However, if the membranes rupture more than 6 weeks before the due date (preterm, or before the 34th week), doctors do not typically induce labor until the fetus is more mature.After a woman with prelabor rupture of membranes is admitted to a birthing center, oxytocin (which causes the uterus to contract) or a similar medication, such as a prostaglandin, is used to induce labor. However, if the membranes rupture more than 6 weeks before the due date (preterm, or before the 34th week), doctors do not typically induce labor until the fetus is more mature.
Admission to a hospital or birthing center
A woman should call her healthcare professional to determine if she should go to a hospital or birthing center when one of the following occurs:
The membranes rupture ("water broke").
For 1 hour, contractions last at least 30 seconds and occur regularly at intervals of about 6 minutes or less.
At the facility, a healthcare professional will evaluate the mother and fetus. If a pregnant woman is in active labor or membranes have ruptured, the woman is admitted to the labor and delivery unit. If the doctor or midwife is not sure whether labor has started, the woman is usually observed and the fetus is monitored for an hour or so. If labor is not confirmed during that time, she may be sent home.

When a woman is admitted to the labor and delivery unit, her vital signs are measured and blood is drawn for analysis.
The presence and rate of fetal heart sounds are recorded, and a physical examination is done. The woman's abdomen is examined to estimate how big the fetus is, whether the fetus is facing rearward or forward (position), and whether the head, face, buttocks, or shoulder is leading the way out (presentation). Sometimes, an ultrasound is done.
Position and presentation of the fetus affect how the fetus passes through the vagina. The most common and safest combination consists of the following:
Head first
Facing rearward (facing down when the woman lies on her back)
Neck bent forward
Chin tucked in
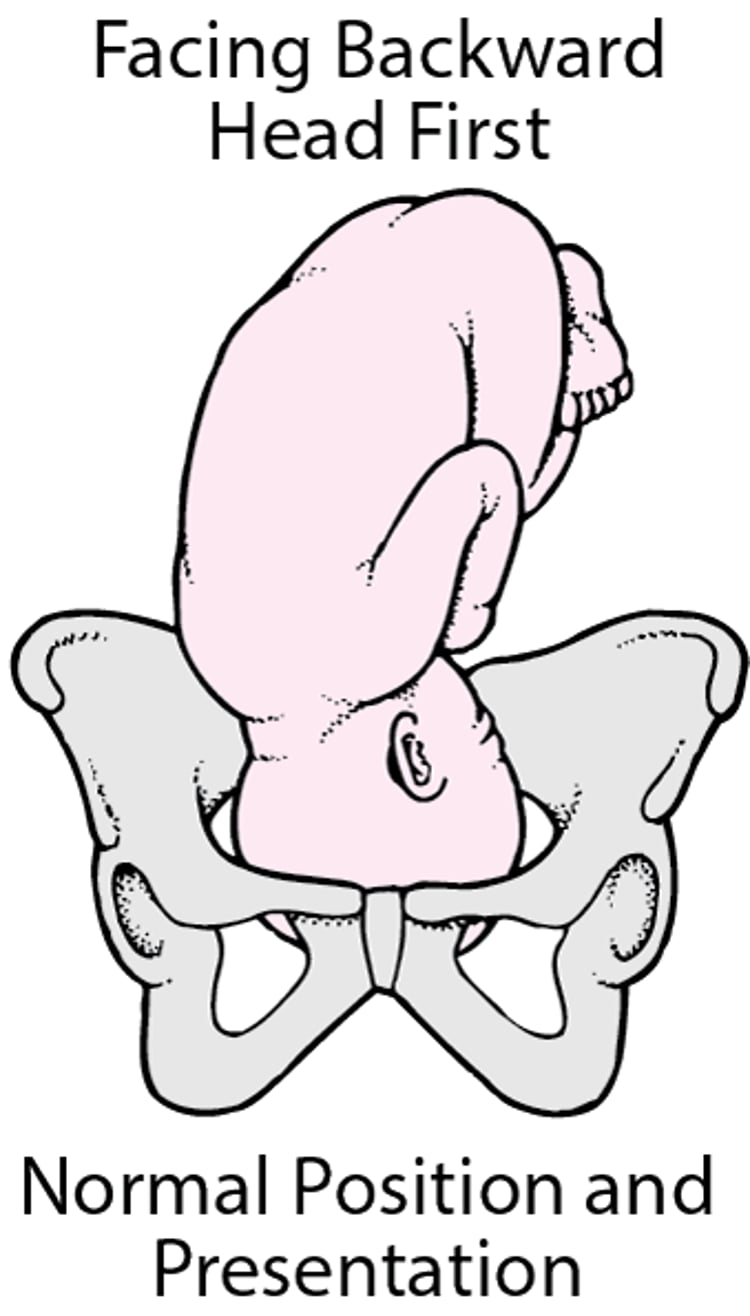
Head first is called a vertex or cephalic presentation. During the last week or two before birth, most fetuses turn so that the back of the head presents first. An abnormal position or presentation—such as buttocks first (breech) or shoulder first or the fetus is facing forward—makes delivery considerably more difficult for the woman, fetus, and doctor. Cesarean delivery is recommended.
Normal Position and Presentation of the Fetus
Toward the end of pregnancy, the fetus moves into position for birth. Normally, the position of a fetus is facing rearward (toward the woman’s back) with the face and body angled to one side and the neck flexed, and presentation is head first. |

A vaginal examination using a speculum may be done to determine whether the membranes have ruptured. (A speculum is a metal or plastic instrument that spreads the walls of the vagina apart). The color of the amniotic fluid is noted. The fluid should be clear and have no significant odor. If the membranes rupture and the amniotic fluid is green, the discoloration results from the fetus’s first stool (fetal meconium).
Then the doctor or midwife examines the cervix with their fingers to determine how dilated (noted in centimeters) and how pulled back (effaced) the cervix is (noted as a percentage or in centimeters). This examination may be omitted if the woman is bleeding or if the membranes have ruptured spontaneously.
If there are concerns about complications after the initial examination, fetal monitoring, and laboratory tests, additional testing or monitoring is done.
An intravenous line is usually inserted into the woman’s arm during labor in a hospital. This line is used to give the woman fluids to prevent dehydration and, if needed, to give medications.
When fluids are given intravenously, the woman does not have to eat or drink during labor, although she may choose to drink some fluids and eat some light food early in labor. An empty stomach during delivery makes the woman less likely to vomit. Very rarely, vomit is inhaled, usually after general anesthesia, which can cause severe pneumonia.







