


Topic Resources
")

Endocarditis usually refers to infection of the endocardium (ie, infective endocarditis). The term can also include noninfective endocarditis, in which sterile platelet and fibrin thrombi form on cardiac valves and adjacent endocardium. Noninfective endocarditis sometimes leads to infective endocarditis. Both can result in embolization and impaired cardiac function.
The diagnosis of infective endocarditis is usually based on a constellation of clinical findings rather than a single definitive test result.
Infective endocarditis can occur at any age. Male individuals are affected about twice as often as female individuals (1). Incidence of infection and mortality increase with increasing age. Patients who use illicit intravenous drugs, patients who are immunocompromised, and patients with prosthetic heart valves and other intracardiac devices are at highest risk. There is also an increased risk in patients with indwelling intravascular catheters.

Reference
1. Cabell CH, Abrutyn E. Progress toward a global understanding of infective endocarditis. Lessons from the International Collaboration on Endocarditis [published correction appears in Cardiol Clin 2003 Aug;21(3):483]. Cardiol Clin 2003;21(2):147-158. doi:10.1016/s0733-8651(03)00033-x
Etiology of Infective Endocarditis
The normal heart is relatively resistant to infection. Bacteria and fungi do not easily adhere to the endocardial surface, and constant blood flow helps prevent them from settling on endocardial structures. Thus, 2 factors are typically required for endocarditis:
A predisposing abnormality of the endocardium
Microorganisms in the bloodstream (eg, bacteremia)
Massive bacteremia or particularly virulent microorganisms (eg, Staphylococcus aureus) cause endocarditis on normal valves.
Endocardial factors
Endocarditis usually involves the heart valves. Major predisposing factors are congenital heart defects, rheumatic valvular disease, bicuspid aortic valves, calcific aortic valves, mitral valve prolapse, hypertrophic cardiomyopathy, and prior endocarditis. Prosthetic valves and other intracardiac devices are a particular risk. Occasionally, mural thrombi, ventricular septal defects, and patent ductus arteriosus sites become infected. The nidus for infection is usually a sterile fibrin-platelet vegetation formed when damaged endothelial cells release tissue factor.
Infective endocarditis occurs most often on the left side (eg, mitral or aortic valve). Approximately 5 to 10% of cases are right-sided (tricuspid or pulmonic valve) (1). Patients who use intravenous drugs have a much higher incidence of right-sided endocarditis.
Microorganisms
Microorganisms that infect the endocardium may originate from distant infected sites (eg, cutaneous abscess, inflamed or infected gums, urinary tract infection) or have obvious portals of entry such as a central venous catheter or a drug injection site. Almost any implanted foreign material (eg, ventricular or peritoneal shunt, prosthetic device) is at risk of bacterial colonization, thus becoming a source of bacteremia and hence endocarditis. Endocarditis also may result from asymptomatic bacteremia, such as typically occurs during invasive dental, medical, or surgical procedures. Even toothbrushing and chewing can cause bacteremia (usually due to viridans streptococci) in patients with gingivitis.
Causative microorganisms vary by site of infection, source of bacteremia, and host risk factors (eg, intravenous drug use), but overall, 80 to 90% of cases are caused by
Streptococci, or
Staphylococcus aureus
Most of the rest of endocarditis cases are caused by
Enterococci
Gram-negative bacilli
HACEK organisms (Haemophilus species, Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella kingae)
Fungi
However, the incidence of staphylococcal and enterococcal endocarditis has been increasing, and streptococcal endocarditis has been decreasing.
The disease develops in 3 stages:
Bacteremia: Microorganisms are present in the blood
Adhesion: The microorganism adheres to abnormal or damaged endothelium via surface adhesions
Colonization: Proliferation of the organism together with inflammation, leading to a mature vegetation
Many of the causative microorganisms produce polysaccharide biofilms that shield them from host immune defences and impede antibiotic penetration.
Etiology reference
1. Delgado V, Ajmone Marsan N, de Waha S, et al: 2023 ESC Guidelines for the management of endocarditis [published correction appears in Eur Heart J 2023 Sep 20] [published correction appears in Eur Heart J 2024 Jan 1;45(1):56]. Eur Heart J 44(39):3948–4042, 2023. doi:10.1093/eurheartj/ehad193
Pathophysiology of Infective Endocarditis
Endocarditis has local and systemic consequences.
Local consequences
Local consequences of infective endocarditis include
Myocardial abscesses with tissue destruction and sometimes conduction system abnormalities (usually with low septal abscesses)
Sudden, severe valvular regurgitation, causing heart failure and death (usually due to lesions of the mitral valve or the aortic valve)
Aortitis due to contiguous spread of infection
Prosthetic valve infections are particularly likely to involve valve ring abscesses, obstructing vegetations, myocardial abscesses, and mycotic aneurysms manifested by valve obstruction, dehiscence, and conduction disturbances.
Systemic consequences
Systemic consequences of endocarditis are primarily due to
Embolization of infected material from the heart valve
Immune-mediated phenomena (primarily in chronic infection)
Right-sided lesions typically produce septic pulmonary emboli, which may result in pulmonary infarction, pneumonia, or empyema. Left-sided lesions may embolize to any tissue, particularly the kidneys, spleen, and central nervous system. Mycotic aneurysms can form in any major artery. Cutaneous and retinal emboli are common. Diffuse glomerulonephritis may result from immune complex deposition.
Classification of Infective Endocarditis
Infective endocarditis may have an indolent, subacute course or a more acute, fulminant course with greater potential for rapid decompensation.
Subacute bacterial endocarditis (SBE), although aggressive, usually develops insidiously and progresses slowly (ie, over weeks to months). Often, no source of infection or portal of entry is evident. SBE is caused most commonly by streptococci (especially viridans, microaerophilic, anaerobic, and nonenterococcal group D streptococci and enterococci) and less commonly by S. aureus, Staphylococcus epidermidis, Gemella morbillorum, Abiotrophia defectiva (formerly, Streptococcus defectivus), Granulicatella species, and fastidious Haemophilus species. SBE often develops on abnormal valves after asymptomatic bacteremia due to periodontal, gastrointestinal, or genitourinary infections.
Acute bacterial endocarditis (ABE) usually develops abruptly and progresses rapidly (ie, over days). A source of infection or portal of entry is often evident. When bacteria are virulent or bacterial exposure is massive, ABE can affect normal valves. It is usually caused by S. aureus, group A hemolytic streptococci, pneumococci, or gonococci.
Prosthetic valvular endocarditis (PVE) develops in 1 to 2% of patients within 1 year after valve replacement and in 0.5%/year thereafter (1). It is more common after aortic than after mitral valve replacement and affects mechanical and bioprosthetic valves equally. Early-onset infections (< 2 months after surgery) are caused mainly by contamination during surgery with antimicrobial-resistant bacteria (eg, S. epidermidis, diphtheroids, coliform bacilli) or by fungi (eg, Candida species, Aspergillus species). Late-onset infections are caused mainly by contamination with low-virulence organisms during surgery or by transient asymptomatic bacteremias, most often with streptococci; S. epidermidis; diphtheroids; and the fastidious gram-negative bacilli, Haemophilus species, Actinobacillus actinomycetemcomitans, and Cardiobacterium hominis.
Classification reference
1. Glaser N, Jackson V, Holzmann MJ, Franco-Cereceda A, Sartipy U. Prosthetic Valve Endocarditis After Surgical Aortic Valve Replacement. Circulation. 2017;136(3):329-331. doi:10.1161/CIRCULATIONAHA.117.028783
Symptoms and Signs of Infective Endocarditis
Symptoms and signs vary based on the classification but are nonspecific.
Subacute bacterial endocarditis
Initially, symptoms of subacute bacterial endocarditis are vague: low-grade fever (< 39° C), night sweats, fatigability, malaise, and weight loss. Chills and arthralgias may occur. Symptoms and signs of valvular insufficiency may be a first clue. Initially, ≤ 15% of patients have fever or a murmur, but eventually almost all develop both. Physical examination may be normal or include pallor, fever, change in a preexisting murmur or development of a new regurgitant murmur, and tachycardia.
Retinal emboli can cause round or oval hemorrhagic retinal lesions with small white centers (Roth spots).
Cutaneous manifestations include petechiae (on the upper trunk, conjunctivae, mucous membranes, and distal extremities), painful erythematous subcutaneous nodules on or near the tips of digits (Osler nodes), nontender hemorrhagic macules or papules on the palms or soles (Janeway lesions), and splinter hemorrhages under the nails.
About 35% of patients have central nervous system (CNS) effects, including transient ischemic attacks, stroke, toxic encephalopathy (due to infective microemboli), and, if a mycotic CNS aneurysm ruptures, brain abscess and subarachnoid hemorrhage.
Renal emboli may cause flank pain and, rarely, gross hematuria.
Splenic emboli may cause left upper quadrant pain.
Prolonged infection may cause splenomegaly or clubbing of fingers and toes.


This patient with infective endocarditis has multiple Osler nodes (tender, erythematous nodules on the toes).
© Springer Science+Business Media


This patient with infective endocarditis has multiple Janeway lesions (nontender, erythematous papules) on the palms. The patient also has some Osler nodes (tender, erythematous nodules on the fingers).
© Springer Science+Business Media


The image on the left shows an Osler node (tender and erythematous nodule) on the thumb. The image on the right shows Janeway lesions (nontender and erythematous macules on the palm).
© Springer Science+Business Media


Splinter hemorrhages are small linear hemorrhages under the fingernails.
Image courtesy of CDC/Dr. Thomas F. Sellers via the Centers for Disease Control and Prevention Public Health Image Library.
This patient with infective endocarditis has multiple Osler nodes (tender, erythematous nodules on the toes).
© Springer Science+Business Media
This patient with infective endocarditis has multiple Janeway lesions (nontender, erythematous papules) on the palms. The patient also has some Osler nodes (tender, erythematous nodules on the fingers).
© Springer Science+Business Media
The image on the left shows an Osler node (tender and erythematous nodule) on the thumb. The image on the right shows Janeway lesions (nontender and erythematous macules on the palm).
© Springer Science+Business Media
Splinter hemorrhages are small linear hemorrhages under the fingernails.
Image courtesy of CDC/Dr. Thomas F. Sellers via the Centers for Disease Control and Prevention Public Health Image Library.


This photo shows conjunctival petechiae in a patient with infective endocarditis.
© Springer Science+Business Media

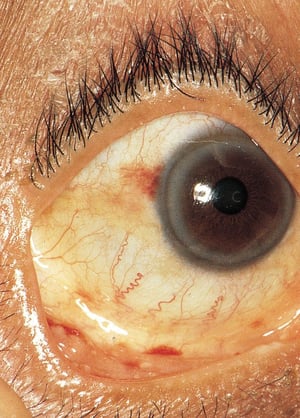
This photo shows conjunctival hemorrhages in a patient with infective endocarditis.
© Springer Science+Business Media

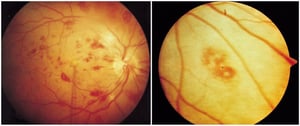
The image on the left shows multiple Roth spots or retinal hemorrhages. The image on the right shows a close up of a Roth spot with central clearing.
© Springer Science+Business Media
This photo shows conjunctival petechiae in a patient with infective endocarditis.
© Springer Science+Business Media
This photo shows conjunctival hemorrhages in a patient with infective endocarditis.
© Springer Science+Business Media
The image on the left shows multiple Roth spots or retinal hemorrhages. The image on the right shows a close up of a Roth spot with central clearing.
© Springer Science+Business Media
Acute bacterial endocarditis and prosthetic valvular endocarditis
Symptoms and signs of acute bacterial endocarditis and prosthetic valvular endocarditis are similar to those of subacute bacterial endocarditis, but the course is more rapid. Fever (78%), cardiac murmur (65%), and congestive heart failure (27%) are the most frequent symptoms at presentation (1). Rarely, purulent meningitis occurs.
Right-sided endocarditis
Septic pulmonary emboli may cause cough, pleuritic chest pain, and sometimes hemoptysis. A murmur of tricuspid regurgitation is typical.
Symptoms and signs reference
1. Delgado V, Ajmone Marsan N, de Waha S, et al: 2023 ESC Guidelines for the management of endocarditis [published correction appears in Eur Heart J 2023 Sep 20] [published correction appears in Eur Heart J 2024 Jan 1;45(1):56]. Eur Heart J 44(39):3948–4042, 2023. doi:10.1093/eurheartj/ehad193
Diagnosis of Infective Endocarditis
Blood cultures or serologic testing
Echocardiography and sometimes other imaging modalities
Clinical criteria
Because symptoms and signs are nonspecific, vary greatly, and may develop insidiously, diagnosis requires a high index of suspicion. Endocarditis should be suspected in patients with fever and no obvious source of infection, particularly if a heart murmur is present. Suspicion of endocarditis should be very high if blood cultures are positive in patients who have a history of a heart valve disorder, who have had certain recent invasive procedures, or who inject drugs. Patients with documented bacteremia should be examined thoroughly and repeatedly for new valvular murmurs and signs of emboli.
Other than positive blood cultures, there are no specific laboratory findings. Established infections often cause a normocytic-normochromic anemia, elevated white blood cell count, increased erythrocyte sedimentation rate, increased immunoglobulin levels, and the presence of circulating immune complexes and rheumatoid factor, but these findings are not diagnostically helpful. Urinalysis often shows microscopic hematuria and, occasionally, red blood cell casts, pyuria, or bacteriuria.
Identification of organisms
Identification of the organism and its antimicrobial susceptibility is vital to guide treatment.
If endocarditis is suspected, at least 2 (ideally 3) sets of blood cultures should be obtained under strict aseptic technique, with one aerobic and one anaerobic culture in each set. Samples should contain 8 to10 mL of blood per bottle and, ideally, are obtained > 6 hours apart (if presentation suggests acute bacterial endocarditis, 2 culture samples are obtained within the first 1 to 2 hours). Each set of cultures should be obtained from a separate, fresh venipuncture site (ie, not from preexisting vascular catheters). Blood cultures do not need to be restricted to times during chills or fever because most patients have continuous bacteremia. When endocarditis is present and no prior antibiotic therapy was given, at least one culture is positive in 90% of patients if more than 2 peripheral blood samples were taken at different times, ideally more than 6 hours apart (1). Premature use of empiric antibiotic therapy should be avoided in patients with acquired or congenital valvular or shunt lesions to avoid inability to isolate causative organisms (culture-negative) endocarditis (2). If prior antimicrobial therapy was given, blood cultures should still be obtained, but results may be negative.
Blood cultures may require 3 to 4 weeks of incubation for certain organisms; however, automated culture monitoring systems available in most clinical laboratories can identify positive cultures within a week. Other organisms (eg, Aspergillus) may not produce positive cultures. Some organisms (eg, Coxiella burnetii, Bartonella species, Chlamydia psittaci, Brucella species) require serodiagnosis; others (eg, Legionella pneumophila) require special culture media or polymerase chain reaction (eg, Tropheryma whippelii). Metagenomic sequencing testing (cell-free DNA testing) may be helpful in selected cases when no pathogen is detected by culture or PCR testing (2). Negative blood culture results may indicate suppression due to
Prior antimicrobial therapy
Infection with organisms that do not grow in standard culture media
Another diagnosis (eg, noninfective endocarditis, atrial myxoma with embolic phenomena, vasculitis)
Imaging studies
Transthoracic echocardiography (TTE) should be done initially. It has sensitivity of 50 to 90% and specificity > 90% (3). Transesophageal echocardiography (TEE) can reveal vegetations too small to be seen on TTE. It has sensitivity of 90 to 100% (4).
Transesophageal echocardiography (TEE) should be done when
Patients have a prosthetic valve (where TTE sensitivity is limited)
Transthoracic echocardiography is nondiagnostic
Diagnosis of infective endocarditis has been established clinically (done to detect perforations, abscesses, and fistulas)
Serial TEE enables diagnosis of complications that evolve during treatment, such as increasing vegetation size or abscess formation.
CT is used as needed to fully define paravalvular abscesses and for detection of mycotic aneurysms.
Positron emission tomography (PET) scanning improves the sensitivity of the modified Duke criteria (see table Clinical Criteria for Infective Endocarditis According to the 2023 Duke-International Society for Cardiovascular Infectious Disease) without compromising specificity. It is especially useful for infection associated with implanted devices, where imaging is hampered by metallic shadowing and postoperative changes (5, 6). PET scanning also detects extracardiac infection, such as septic emboli, and is an emerging tool for the diagnosis of endocarditis originating in prosthetic and intracardiac devices. CT and PET abnormalities are included as major criteria in the Duke criteria and European guidelines (5).
Routine brain imaging has been proposed because up to approximately 70% of patients have clinically silent lesions (7). Its utility for prognosis and management is yet to be defined.
Diagnostic criteria
Infective endocarditis is definitively diagnosed when microorganisms are seen histologically in (or cultured from) endocardial vegetations obtained during cardiac surgery, embolectomy, or autopsy. Because vegetations are not usually available for examination, there are various clinical criteria for establishing a diagnosis. These include the latest iteration of the Duke criteria (2023 Duke-International Society for Cardiovascular Infectious Disease Criteria) (8), which has a sensitivity of 84% and a specificity of 94% (9) (see tables Definitions of Infective Endocarditis and Clinical Criteria for Infective Endocarditis) and the European Society of Cardiology (ESC) 2023 modified criteria (5).
Definitions of Infective Endocarditis According to the 2023 Duke-International Society for Cardiovascular Infectious Disease Criteria
Clinical Diagnosis Status | Criteria |
|---|---|
Definite endocarditis | Pathologic criteria: 1. Histopathologic findings of endocarditis OR 2. Microorganisms identified in patients with clinical signs of active endocarditis or Clinical criteria (one of the following):
|
Possible endocarditis | One of the following:
|
Rejected endocarditis | One of the following:
|
Data from Table 1, page 520. Fowler VG, Durack DT, Selton-Suty C, et al: The 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: Updating the Modified Duke Criteria [published correction appears in Clin Infect Dis 2023 Oct 13;77(8):1222]. Clin Infect Dis 77(4):518–526, 2023. doi:10.1093/cid/ciad271 | |
Clinical Criteria for Infective Endocarditis According to the 2023 Duke-International Society for Cardiovascular Infectious Disease
Major criteria Microbiology: 1. Two or more positive separate sets of blood cultures for organisms typical of endocarditis OR Three or more positive separate sets of blood cultures for organisms that rarely or occasionally cause endocarditis 2. PCR or other nucleic acid technique that identifies Coxiella burnetii, Bartonella species, or Tropheryma whipplei from blood OR Serologic evidence of Coxiella burnetii (IgG titer > 1:800) or 1 positive blood culture for Coxiella burnetii OR Indirect immunofluorescence assays for detection of IgM and IgG antibodies to Bartonella henselae or Bartonella quintana (IgG titer> 1:800) Imaging (eg, echocardiographic, CT, [18F]-FDG-PET/CT(A):
Surgical: Evidence of infective endocarditis observed on direct inspection during cardiac surgery. |
Minor criteria Predisposition: ,
Fever ≥ 38.0° C (≥ 100.4°F) Vascular phenomena (confirmed by clinical or imaging evidence):
Immunologic phenomena:
Microbiologic evidence of infection consistent with but not meeting major criteria: 1. Blood culture showing an organism consistent with infective endocarditis OR 2. Positive culture, PCR, or other nucleic acid–based test for an organism consistent with infective endocarditis from a sterile body site other than cardiac tissue, cardiac prosthesis, or arterial embolus; or a single finding of a skin bacterium by PCR on a valve or wire without additional clinical or microbiological supporting evidence Imaging criteria: [18F]-FDG-PET/CT imaging with abnormal metabolic activity involving a native or prosthetic valve (within 3 months after valve implantation), ascending aortic graft (with concomitant evidence of valve involvement), intracardiac device leads, or other prosthetic material Physical examination criteria: If echocardiography is not available, auscultatory evidence of new valvular regurgitation. Worsening or changing of preexisting regurgitation is not sufficient. |
Data from Table 2, page 521. Fowler VG, Durack DT, Selton-Suty C, et al: The 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: Updating the Modified Duke Criteria [published correction appears in Clin Infect Dis 2023 Oct 13;77(8):1222]. Clin Infect Dis 77(4):518–526, 2023. doi:10.1093/cid/ciad271 |
Diagnosis references
1. Otto CM, Nishimura RA, Bonow RO, et al: 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [published correction appears in Circulation. 2021 Feb 2;143(5):e229. doi: 10.1161/CIR.0000000000000955] [published correction appears in Circulation. 2023 Aug 22;148(8):e8. doi: 10.1161/CIR.0000000000001177] [published correction appears in Circulation. 2023 Nov 14;148(20):e185. doi: 10.1161/CIR.0000000000001190]. Circulation 143(5):e72–e227, 2021. doi:10.1161/CIR.0000000000000923
2. DeSimone DC, Garrigos ZE, Marx GE, et al: Blood Culture-Negative Endocarditis: A Scientific Statement From the American Heart Association: Endorsed by the International Society for Cardiovascular Infectious Diseases [published correction appears in J Am Heart Assoc 2025 Apr 23:e10928. doi: 10.1161/JAHA.124.035178]. J Am Heart Assoc 2025;14(8):e040218. doi:10.1161/JAHA.124.040218
3. Bai AD, Steinberg M, Showler A, et al: Diagnostic Accuracy of Transthoracic Echocardiography for Infective Endocarditis Findings Using Transesophageal Echocardiography as the Reference Standard: A Meta-Analysis. J Am Soc Echocardiogr 30(7):639–646.e8, 2017. doi:10.1016/j.echo.2017.03.007
4. Shapiro SM, Young E, De Guzman S, et al: Transesophageal echocardiography in diagnosis of infective endocarditis. Chest 105(2):377–382, 1994. doi:10.1378/chest.105.2.377
5. Delgado V, Ajmone Marsan N, de Waha S, et al: 2023 ESC Guidelines for the management of endocarditis [published correction appears in Eur Heart J 2023 Sep 20] [published correction appears in Eur Heart J 45(1):56, 2024]. Eur Heart J 44(39):3948–4042, 2023. doi:10.1093/eurheartj/ehad193
6. Dilsizian V, Budde RPJ, Chen W, et al: Best practices for imaging cardiac device-related infections and endocarditis: A JACC: Cardiovascular Imaging Expert Panel Statement. JACC Cardiovasc Imaging 15(5):891–911, 2022. doi: 10.1016/j.jcmg.2021.09.029
7. Hess A, Klein I, Iung B, et al: Brain MRI findings in neurologically asymptomatic patients with infective endocarditis. AJNR Am J Neuroradiol 34(8):1579–1584, 2013. doi:10.3174/ajnr.A3582
8. Fowler VG, Durack DT, Selton-Suty C, et al: The 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: Updating the Modified Duke Criteria [published correction appears in Clin Infect Dis 2023 Oct 13;77(8):1222]. Clin Infect Dis 77(4):518–526, 2023. doi:10.1093/cid/ciad271
9. van der Vaart TW, Bossuyt PMM, Durack DT, et al: External Validation of the 2023 Duke-International Society for Cardiovascular Infectious Diseases Diagnostic Criteria for Infective Endocarditis. Clin Infect Dis 78(4):922–929, 2024. doi:10.1093/cid/ciae033
Treatment of Infective Endocarditis
IV antibiotics (based on the organism and its susceptibility)
Sometimes valve debridement, repair, or replacement
Dental evaluation and treatment (to minimize oral sources of bacteremia)
Removal of potential source of bacteremia (eg, internal catheters, devices)
Withholding anticoagulation in patients with cerebral embolism
Treatment consists of a prolonged course of antimicrobial therapy (1). Surgery may be needed for mechanical complications or resistant organisms. Typically, antimicrobials are given IV. Because they must be given for 2 to 8 weeks, home IV therapy is often used.
Any apparent source of bacteremia must be managed: necrotic tissue debrided, abscesses drained, and foreign material and infected devices removed. Patients with infective endocarditis should be evaluated by a dentist and treated for oral diseases that could cause bacteremia and subsequent endocarditis. Existing IV catheters (particularly central venous ones) should be changed. If endocarditis persists in a patient with a newly inserted central venous catheter, that catheter should also be removed. If continuous infusions are used instead of intermittent boluses, infusions should not be interrupted for long periods.
Organisms within biofilms adherent to catheters and other devices may not respond to antimicrobial therapy, leading to treatment failure or relapse.
Antibiotic regimens
Medications and dosages depend on the microorganism and its antimicrobial susceptibility.
Although most patients are stable enough to wait for culture results, empiric antibiotic therapy before organism identification may be necessary in seriously ill patients. Antibiotics should not be given until adequate blood cultures (minimally 2, but ideally 3, samples from different sites over 1 hour) have been obtained. An empiric regimen should cover typical pathogens (ie, Staphylococci and Streptococci species), take into account local resistance pattern, such as MRSA prevalence, and include an agent highly effective at killing (eg, a beta-lactam antibiotic). A typical regimen in the United States may be vancomycin and ceftriaxone. Certain risk factors for having endocarditis with a less common pathogen or having a more difficult to eradicate infection include a recently placed prosthetic valve, prolonged healthcare exposure, and critical illness. Combination therapy is commonly started in these scenarios and often includes broader spectrum of antibacterial activity and consideration of synergistic agents like aminoglycosides. An empiric regimen should cover typical pathogens (ie, Staphylococci and Streptococci species), take into account local resistance pattern, such as MRSA prevalence, and include an agent highly effective at killing (eg, a beta-lactam antibiotic). A typical regimen in the United States may be vancomycin and ceftriaxone. Certain risk factors for having endocarditis with a less common pathogen or having a more difficult to eradicate infection include a recently placed prosthetic valve, prolonged healthcare exposure, and critical illness. Combination therapy is commonly started in these scenarios and often includes broader spectrum of antibacterial activity and consideration of synergistic agents like aminoglycosides.
As soon as possible, the empiric antimicrobial regimen should be adjusted based on culture results.
Some Antibiotic Regimens for Endocarditis in the United States*
Type | Medication And Dosage for Adults | Medication and Dosage for Adults Allergic to Penicillin |
|---|---|---|
Streptococci susceptible to penicillin (penicillin G MIC Streptococci susceptible to penicillin (penicillin G MIC≤ 0.1 mcg/mL) | For NVE: Penicillin G 12–18 million units a day IV continuously or 2–3 million units every 4 hours for 4 weeks or, if gentamicin 3 mg/kg† IV or IM once a day is given concurrently, for 2 weeks: Penicillin G 12–18 million units a day IV continuously or 2–3 million units every 4 hours for 4 weeks or, if gentamicin 3 mg/kg† IV or IM once a day is given concurrently, for 2 weeks For PVE: Penicillin G 24 million units a day IV continuously or 4 million units every 4 hours for 6 weeks or, if gentamicin 3 mg/kg† IV or IM (up to 80 mg) is given concurrently, for 2 weeks: Penicillin G 24 million units a day IV continuously or 4 million units every 4 hours for 6 weeks or, if gentamicin 3 mg/kg† IV or IM (up to 80 mg) is given concurrently, for 2 weeks | Ceftriaxone 2 g IV or IM once a day for 4 weeks for NVE (6 weeks for PVE) or, if gentamicin 3 mg/kg† IV or IM once a day is given concurrently, for 2 weeks if there is no history of penicillin anaphylaxisCeftriaxone 2 g IV or IM once a day for 4 weeks for NVE (6 weeks for PVE) or, if gentamicin 3 mg/kg† IV or IM once a day is given concurrently, for 2 weeks if there is no history of penicillin anaphylaxis or Vancomycin‡ 15 mg/kg IV every 12 hours for 4 weeks for NVE (6 weeks for PVE)Vancomycin‡ 15 mg/kg IV every 12 hours for 4 weeks for NVE (6 weeks for PVE) |
Streptococci resistant to penicillin (penicillin G MIC Streptococci resistant to penicillin (penicillin G MIC> 0.1 mcg/mL) | For NVE: Gentamicin 3 mg/kg† IV or IM once a day for 2 weeks plus penicillin G 24 million units/ a day IV continuously or 4 million units every 4 hours for 4 weeksFor NVE: Gentamicin 3 mg/kg† IV or IM once a day for 2 weeks plus penicillin G 24 million units/ a day IV continuously or 4 million units every 4 hours for 4 weeks For PVE: Gentamicin 3 mg/kg† IV or IM once a day for 2 weeks plus penicillin G 24 million units a day IV continuously or 4 million units every 4 hours or ceftriaxone 2 g once a day IV or IM for 6 weeksFor PVE: Gentamicin 3 mg/kg† IV or IM once a day for 2 weeks plus penicillin G 24 million units a day IV continuously or 4 million units every 4 hours or ceftriaxone 2 g once a day IV or IM for 6 weeks | Vancomycin‡ 15 mg/kg IV every 12 hours for 4 weeks for NVE (6 weeks for PVE)Vancomycin‡ 15 mg/kg IV every 12 hours for 4 weeks for NVE (6 weeks for PVE) |
Enterococci | For NVE and PVE: Ampicillin 2 g IV every 4 hours plus ceftriaxone 2 g IV every 12 hours for 6 weeksFor NVE and PVE: Ampicillin 2 g IV every 4 hours plus ceftriaxone 2 g IV every 12 hours for 6 weeks | For NVE and PVE: Vancomycin 15 mg/kg IV every 12 hours plus gentamicin 3 mg/kg IV or IM once a day or gentamicin 1 mg/kg IV or IM every 8 hours for 6 weeksFor NVE and PVE: Vancomycin 15 mg/kg IV every 12 hours plus gentamicin 3 mg/kg IV or IM once a day or gentamicin 1 mg/kg IV or IM every 8 hours for 6 weeks or For NVE and PVE: Linezolid 600 mg orally or IV every 12 hours for 6–8 weeksFor NVE and PVE: Linezolid 600 mg orally or IV every 12 hours for 6–8 weeks or For NVE and PVE: Daptomycin 10–12 mg/kg IV once a day for 6–8 weeksFor NVE and PVE: Daptomycin 10–12 mg/kg IV once a day for 6–8 weeks |
Staphylococci susceptible to oxacillinStaphylococci susceptible to oxacillin | For NVE: Oxacillin or nafcillin 2 g IV every 4 hours for 6 weeksFor NVE: Oxacillin or nafcillin 2 g IV every 4 hours for 6 weeks For PVE: Oxacillin or nafcillin 2 g IV every 4 hours for 6–8 weeks plus gentamicin 1 mg/kg† IV every 8 hours for 2 weeks plus rifampin 300 mg IV or orally every 8 hours for 6–8 weeksFor PVE: Oxacillin or nafcillin 2 g IV every 4 hours for 6–8 weeks plus gentamicin 1 mg/kg† IV every 8 hours for 2 weeks plus rifampin 300 mg IV or orally every 8 hours for 6–8 weeks | NVE: Cefazolin 2 g IV every 8 hours for 6 weeks if there is no history of penicillin anaphylaxis (6–8 weeks for PVE)NVE: Cefazolin 2 g IV every 8 hours for 6 weeks if there is no history of penicillin anaphylaxis (6–8 weeks for PVE) or Vancomycin‡ 15 mg/kg IV every 12 hours for 4 weeks for NVE (6–8 weeks for PVE)Vancomycin‡ 15 mg/kg IV every 12 hours for 4 weeks for NVE (6–8 weeks for PVE) or For right-sided NVE: Daptomycin 6 mg/kg IV once a day for 6 weeksFor right-sided NVE: Daptomycin 6 mg/kg IV once a day for 6 weeks |
Staphylococci resistant to oxacillin Staphylococci resistant to oxacillin | For NVE: Vancomycin† 15 mg/kg IV every 12 hours alone for 6 weeksFor NVE: Vancomycin† 15 mg/kg IV every 12 hours alone for 6 weeks For PVE: Vancomycin‡ 15 mg/kg IV every 12 hours for 6–8 weeks, plus gentamicin 1 mg/kg IV† every 8 hours for 2 weeks plus rifampin 300 mg orally every 8 hours for 6–8 weeks for PVEFor PVE: Vancomycin‡ 15 mg/kg IV every 12 hours for 6–8 weeks, plus gentamicin 1 mg/kg IV† every 8 hours for 2 weeks plus rifampin 300 mg orally every 8 hours for 6–8 weeks for PVE or For right-sided NVE: Daptomycin 6 mg/kg IV once a day for 6 weeksFor right-sided NVE: Daptomycin 6 mg/kg IV once a day for 6 weeks | — |
HACEK microorganisms§ | Ceftriaxone 2 g once/day IV or IM for 4 weeks for NVE (6 weeks for PVE)Ceftriaxone 2 g once/day IV or IM for 4 weeks for NVE (6 weeks for PVE) or Ampicillin 2 g IV every 4 hours for 4 weeks for NVE (6 weeks for PVE)Ampicillin 2 g IV every 4 hours for 4 weeks for NVE (6 weeks for PVE) or Ciprofloxacin 1000 mg orally once a day or 400 mg IV every 12 hours for 4 weeks for NVE (6 weeks for PVE)Ciprofloxacin 1000 mg orally once a day or 400 mg IV every 12 hours for 4 weeks for NVE (6 weeks for PVE) | Ceftriaxone 2 g IV once a day for 4 weeks for NVE (6 weeks for PVE) if there is no history of penicillin anaphylaxisCeftriaxone 2 g IV once a day for 4 weeks for NVE (6 weeks for PVE) if there is no history of penicillin anaphylaxis |
Noncoliform bacilli | Sensitivity-proven beta-lactam antimicrobial (eg, ceftriaxone 2 g IV every 12–24 hours or ceftazidime 2 g IV every 8 hours) plus an aminoglycoside (eg, gentamicin 2 mg/kg† IV every 8 hours) for 6 weeksSensitivity-proven beta-lactam antimicrobial (eg, ceftriaxone 2 g IV every 12–24 hours or ceftazidime 2 g IV every 8 hours) plus an aminoglycoside (eg, gentamicin 2 mg/kg† IV every 8 hours) for 6 weeks | — |
* Antimicrobial sensitivity changes over time, and there are site-specific differences in antimicrobial susceptibility. Advice from a consultant familiar with these patterns is imperative. | ||
† Based on ideal rather than actual weight in patients with obesity. | ||
‡ With vancomycin, serum levels must be monitored if doses ‡ With vancomycin, serum levels must be monitored if doses> 2 g/24 hours are administered. | ||
§ HACEK microorganisms: Haemophilus parainfluenzae, H. aphrophilus, Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella kingae. | ||
MIC = minimum inhibitory concentration; NVE = native valve endocarditis; PVE = prosthetic valve endocarditis. | ||
Adapted from Baddour LM, Wilson WR, Bayer AS, et al: Infective endocarditis in adults: Diagnosis, antimicrobial therapy, and management of complications; A scientific statement for healthcare professionals from the American Heart Association. Circulation 132 (15):1435–1486, 2015. doi: 10.1161/CIR.0000000000000296 | ||
Pearls & Pitfalls
|
Native valve right-sided endocarditis can often be treated with 4 weeks of therapy or even as short as 2 weeks for certain typical pathogens (eg,methicillin-sensitive S. aureus) if combination therapy with gentamicin is used. For left-sided endocarditis, guidelines recommend 6 weeks of parenteral antibiotic therapy. However, a multicenter, randomized, non-blinded study of uncomplicated left-sided endocarditis found switching to oral antibiotics (after a minimum of 10 days of parenteral therapy) to be non-inferior to continued parenteral therapy. In addition, length of hospital stay was shortened in the patients switched to oral therapy. This approach has the potential to reduce the psychologic stress and some of the risks inherent to prolonged inpatient parenteral therapy () if combination therapy with gentamicin is used. For left-sided endocarditis, guidelines recommend 6 weeks of parenteral antibiotic therapy. However, a multicenter, randomized, non-blinded study of uncomplicated left-sided endocarditis found switching to oral antibiotics (after a minimum of 10 days of parenteral therapy) to be non-inferior to continued parenteral therapy. In addition, length of hospital stay was shortened in the patients switched to oral therapy. This approach has the potential to reduce the psychologic stress and some of the risks inherent to prolonged inpatient parenteral therapy (2). Long-acting lipoglycopeptide antibiotics, such as dalbavancin, have also been used successfully as part of sequential therapy for Gram positive endocarditis (). Long-acting lipoglycopeptide antibiotics, such as dalbavancin, have also been used successfully as part of sequential therapy for Gram positive endocarditis (3). These options may be particularly useful for patients in whom home parenteral therapy is not feasible.
Cardiac valve surgery
Surgery (debridement, valve repair, or valve replacement) is sometimes required for treatment of infectious endocarditis (4). Surgery is typically indicated in
Patients with heart failure (particularly those with prosthetic, aortic, or native mitral valve endocarditis and those with pulmonary edema or cardiogenic shock)
Patients with uncontrolled infection (those with persistent infection, infection with fungal or resistant organisms, recurrent prosthetic valve endocarditis, or endocarditis complicated by heart block, abscess, aneurysm, fistula, or enlarging vegetation)
Patients at risk for embolism (particularly those with prosthetic, aortic, or native mitral valve endocarditis, and large vegetations [defined as > 10 mm] or those with recurrent emboli). Early surgery in these patients decreases the risk of embolic events.
Timing of surgery requires experienced clinical judgment. If heart failure caused by a correctable lesion is worsening (particularly when the organism is S. aureus, a gram-negative bacillus, or a fungus), surgery may be required after only 24 to 72 hours of antimicrobial therapy.
Endocarditis involving an implanted cardiac electronic device requires complete removal of the pacemaker or defibrillator, including all leads and the generator.
Right-sided endocarditis is usually managed medically. If surgery is necessary (due to heart failure or lack of therapeutic response), then valve repair is preferred over replacement to avoid future prosthetic valve infection due to any continued IV drug use. Prophylactic placement of an epicardial pacing lead is recommended at time of tricuspid valve surgery (5). Prophylactic placement avoids any future need for an endovascular pacing lead to traverse the (native or prosthetic) tricuspid valve and potentially cause tricuspid regurgitation.
Surgery is usually delayed for a month after intracranial hemorrhage or major ischemic stroke.
Anticoagulation
Patients taking anticoagulants are at increased risk for hemorrhagic stroke and for bleeding resulting from urgent invasive procedures. Anticoagulation should be withheld in patients with cerebral emboli, because it increases the risk of hemorrhagic transformation. The decision to withhold anticoagulation in other patients should be based on the relative risks of hemorrhagic stroke and thromboembolism (6).
Response to treatment
After starting therapy, patients with penicillin-susceptible streptococcal endocarditis usually feel better, and fever is reduced within 3 to 7 days. Fever may continue for reasons other than persistent infection (eg, medication allergy, phlebitis, infarction due to emboli). Patients with staphylococcal endocarditis tend to respond more slowly. Diminution of vegetation size can be followed by serial echocardiography. Echocardiography should be done at the completion of therapy to establish a new baseline for valvular appearance (including sterile vegetations) and insufficiency.
Relapse usually occurs within 4 weeks. Antibiotic retreatment may be effective, but surgery may also be required. In patients without prosthetic valves, recrudescence of endocarditis after 6 weeks usually results from a new infection rather than a relapse. Even after successful antimicrobial therapy, sterile emboli and valve rupture may occur up to 1 year later. Risk of recurrence is significant, so ongoing life-long dental and cutaneous hygiene is advised. Patients who require antibiotic therapy for any reason should have at least 3 sets of blood cultures drawn before antibiotics are started.
Treatment references
1. Baddour LM, Wilson WR, Bayer AS, et al: Infective endocarditis in adults: Diagnosis, antimicrobial therapy, and management of complications: A scientific statement for healthcare professionals from the American Heart Association. Circulation 132:1435–1486, 2015.
2. Iversen K, Ihlemann N, Gill SU, et al: Partial oral versus intravenous antibiotic treatment of endocarditis. N Engl J Med 380:415–424, 2019. DOI: 10.1056/NEJMoa1808312
3. Fazili T, Bansal E, Garner D, Gomez M, Stornelli N: Dalbavancin as sequential therapy for infective endocarditis due to Gram-positive organisms: a review. Int J Antimicrob Agents 61(4):106749, 2023. doi:10.1016/j.ijantimicag.2023.106749
4. Cahill TJ, Baddour LM, Habib G, et al: Challenges in infective endocarditis. J Am Coll Cardiol 69(3):325–344, 2017.
5. Delgado V, Ajmone Marsan N, de Waha S, et al: 2023 ESC Guidelines for the management of endocarditis [published correction appears in Eur Heart J 2023 Sep 20] [published correction appears in Eur Heart J 45(1):56, 2024]. Eur Heart J 44(39):3948–4042, 2023. doi:10.1093/eurheartj/ehad193
6. Otto CM, Nishimura RA, Bonow RO, et al: 2020 ACC/AHA Guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 77(4):e25–e197, 2021. doi: 10.1016/j.jacc.2020.11.018
Prognosis for Infective Endocarditis
Overall, the in-hospital mortality rate for endocarditis is 15 to 20%, with a 1-year mortality rate approaching 40% (1). Untreated, infective endocarditis is always fatal. Even with treatment, death is more likely and the prognosis is generally poorer for older patients and patients who have
Infection with resistant organisms
An underlying disorder
A long delay in treatment
Aortic valve or multiple valve involvement
Large vegetations
Polymicrobial bacteremia
Prosthetic valve infections
Mycotic aneurysms
Valve ring abscess
Major embolic events
Septic shock is more likely in patients with diabetes, acute kidney injury, S. aureus infection, vegetation size > 15 mm, or signs of persistent infection. The mortality rate for viridans streptococcal endocarditis without major complications is < 10% (2) but is greater than 90% for Aspergillus endocarditis after prosthetic valve surgery (3).
The prognosis is better with right-sided than left-sided endocarditis because tricuspid valve dysfunction is tolerated better, systemic emboli are absent, and right-sided S. aureus endocarditis responds better to antimicrobial therapy.
Prognosis references
1. Otto CM, Nishimura RA, Bonow RO, et al: 2020 ACC/AHA Guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 77(4):e25–e197, 2021. doi: 10.1016/j.jacc.2020.11.018
2. Hill EE, Herijgers P, Claus P, et al: Infective endocarditis: changing epidemiology and predictors of 6-month mortality: a prospective cohort study. Eur Heart J 28(2):196–203, 2007. doi:10.1093/eurheartj/ehl427
3. Gumbo T, Taege AJ, Mawhorter S, et al. Aspergillus valve endocarditis in patients without prior cardiac surgery. Medicine (Baltimore). 2000;79(4):261-268. doi:10.1097/00005792-200007000-00007
Prevention of Infective Endocarditis
Preventive dental examination and therapy before surgery to repair heart valves or congenital heart lesions is recommended.
Measures to reduce health care–acquired bacteremia aim to curb the rising incidence of iatrogenic bacteremia and subsequent endocarditis are also recommended (1).
Endocarditis prophylaxis during implantation of prosthetic devices has changed to accommodate the rise in endocarditis due to enterococci. Prophylaxis often involves the addition of vancomycin or use of amoxicillin/clavulanic acid instead of a cephalosporin (Endocarditis prophylaxis during implantation of prosthetic devices has changed to accommodate the rise in endocarditis due to enterococci. Prophylaxis often involves the addition of vancomycin or use of amoxicillin/clavulanic acid instead of a cephalosporin (2).
Dental and cutaneous hygiene is recommended for the general population but particularly for patients at intermediate risk (those with native valve disease) and high risk.
Patients at high risk
The American Heart Association (AHA) recommends antimicrobial prophylaxis for patients at high risk of an adverse outcome as a result of infective endocarditis (3). Such patients include those with
Prosthetic heart valves, including transcatheter implanted prostheses
Prosthetic material used for heart valve repair (eg, annuloplasty rings, chords)
Previous infective endocarditis
Certain congenital heart diseases (CHD): Unrepaired cyanotic CHD (including palliative shunts and conduits), completely repaired CHD during the first 6 months after surgery if prosthetic material or device was used, repaired CHD that has residual defects at or adjacent to the site of repair
Heart transplant recipients with valvulopathy
Procedures requiring antibiotic prophylaxis
Most procedures for which prophylaxis is required for patients at high risk are oral-dental procedures that manipulate the gingiva or the periapical region of teeth or perforate the oral mucosa (see table Procedures Requiring Antimicrobial Endocarditis Prophylaxis). Other procedures include
Respiratory tract procedures in which mucosa is incised
Vaginal or cesarean delivery in selected patients at high risk (patients with a prosthetic cardiac valve or prosthetic material used for cardiac valve repair and for patients with unrepaired and palliated cyanotic congenital heart disease)
Gastrointestinal procedures that involve an area with an established infection
Genitourinary procedures that involve an area with an established infection
Musculoskeletal procedures that involve an area with an established infection
Recognition that other non-dental procedures may cause endocarditis may result in expansion of this list in future guidelines (4, 5).
Procedures Requiring Antimicrobial Endocarditis Prophylaxis in Patients at High Risk for Endocarditis
Type | Examples |
Oral-dental* | Dental extraction Dental implant placement or reimplantation of avulsed teeth Periodontal procedures, including surgery, scaling, root planing, and probing Prophylactic cleaning of teeth or implants when bleeding is anticipated Root canal instrumentation or surgery beyond the apex |
Respiratory tract | Bronchoscopy if mucosa is to be incised Procedures done during an established infection Tonsillectomy, adenoidectomy, or both |
Gastrointestinal tract | None, unless procedure is done during an established infection |
Genitourinary tract | None, unless procedure is done during an established infection (eg, cystoscopy during known enterococcal urinary tract infection) |
Musculoskeletal | None, unless procedure involves infected tissue |
Skin | None, unless procedure involves infected tissue |
* Examples of oral-dental procedures that do not require prophylaxis are anesthetic injection through uninfected mucosa and placement of orthodontic brackets. | |
Data from Wilson W, Taubert KS, Gewitz M, et al: Prevention of infective endocarditis. Circulation 116 (15):1736–1754, 2007 and Warnes CA, Williams RG, Bashore TM, et al: ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 118(23):e714, 2008. | |
Prophylactic antibiotic regimens
For most patients and procedures, a single dose shortly before the procedure is effective. For oral-dental and respiratory procedures, a medication effective against viridans group streptococci is used (see table Recommended Endocarditis Prophylaxis During Oral-Dental or Respiratory Tract Procedures).
For vaginal delivery, give ampicillin 2 g IV or IM plus gentamicin 1.5 mg/kg (maximum 120 mg) IV administered within 30 minutes before delivery, followed by ampicillin 1 g IV or IM (or amoxicillin 1 g [as the trihydrate] orally) 6 hours later.For vaginal delivery, give ampicillin 2 g IV or IM plus gentamicin 1.5 mg/kg (maximum 120 mg) IV administered within 30 minutes before delivery, followed by ampicillin 1 g IV or IM (or amoxicillin 1 g [as the trihydrate] orally) 6 hours later.
For gastrointestinal, genitourinary, and musculoskeletal procedures on areas involving infected tissue, antibiotics should be selected based on the known organism and its sensitivities. If infection is present but the infecting organism has not been identified, antibiotics for gastrointestinal and genitourinary prophylaxis should be effective against enterococci (eg, amoxicillin or ampicillin, or vancomycin for patients who are allergic to penicillin). For gastrointestinal, genitourinary, and musculoskeletal procedures on areas involving infected tissue, antibiotics should be selected based on the known organism and its sensitivities. If infection is present but the infecting organism has not been identified, antibiotics for gastrointestinal and genitourinary prophylaxis should be effective against enterococci (eg, amoxicillin or ampicillin, or vancomycin for patients who are allergic to penicillin).
Antibiotics for skin and musculoskeletal prophylaxis should be effective against staphylococci and beta-hemolytic streptococci (eg, a cephalosporin or vancomycin or clindamycin if infection with methicillin-resistant staphylococci is possible).Antibiotics for skin and musculoskeletal prophylaxis should be effective against staphylococci and beta-hemolytic streptococci (eg, a cephalosporin or vancomycin or clindamycin if infection with methicillin-resistant staphylococci is possible).
Guidelines for endocarditis prophylaxis vary geographically.
Additional information regarding prophylactic regimens is provided by guidelines from the American Heart Association and the European Society of Cardiology (3, 4).
Prevention references
1. García-Rodríguez JF, Mariño-Callejo A: The factors associated with the trend in incidence of Bacteraemia and associated mortality over 30 years. BMC Infect Dis 23(1):69, 2023. doi:10.1186/s12879-023-08018-0
2. Cuervo G, Quintana E, Regueiro A, et al: The Clinical Challenge of Prosthetic Valve Endocarditis: JACC Focus Seminar 3/4. J Am Coll Cardiol 83(15):1418–1430, 2024. doi:10.1016/j.jacc.2024.01.037
3. Wilson WR, Gewitz M, Lockhart PB, et al: Prevention of Viridans Group Streptococcal Infective Endocarditis: A Scientific Statement From the American Heart Association [published correction appears in Circulation 2021 Aug 31;144(9):e192] [published correction appears in Circulation 2022 Apr 26;145(17):e868]. Circulation 143(20):e963–e978, 2021. doi:10.1161/CIR.0000000000000969
4. Delgado V, Ajmone Marsan N, de Waha S, et al: 2023 ESC Guidelines for the management of endocarditis [published correction appears in Eur Heart J 2023 Sep 20] [published correction appears in Eur Heart J 45(1):56, 2024]. Eur Heart J 44(39):3948–4042, 2023. doi:10.1093/eurheartj/ehad193
5. Baddour LM, Janszky I, Thornhill MH, et al: Nondental Invasive Procedures and Risk of Infective Endocarditis: Time for a Revisit: A Science Advisory From the American Heart Association. Circulation 148(19):1529–1541, 2023. doi:10.1161/CIR.0000000000001180
Key Points
Because the normal heart is relatively resistant to infection, endocarditis occurs mainly when there is a predisposing abnormality of the endocardium.
Predisposing cardiac abnormalities include congenital heart defects, rheumatic valvular disease, bicuspid or calcific aortic valves, mitral valve prolapse, hypertrophic cardiomyopathy, prior endocarditis, and intracardiac devices.
Local cardiac consequences include myocardial abscess, conduction system abnormalities, and sudden, severe valvular regurgitation.
Systemic consequences include immune phenomena (eg, glomerulonephritis) and septic emboli, which may affect any organ put particularly the lungs (with right sided endocarditis), kidneys, spleen, central nervous system, skin, and retina (with left-sided endocarditis).
Obtain blood cultures and diagnose using modified Duke or European Society of Cardiology clinical criteria.
Treat with a prolonged course of antimicrobial therapy; surgery may be needed for mechanical complications or resistant organisms.
Give antimicrobial prophylaxis for patients at high risk of an adverse outcome from infective endocarditis, including those with prosthetic heart valves or heart valve repair, previous infective endocarditis, certain congenital heart diseases, or who are heart transplant recipients with valvulopathy.
Drugs Mentioned In This Article






