

Mitral valve prolapse (MVP) is a billowing of mitral valve leaflets into the left atrium during systole. The most common cause is idiopathic myxomatous degeneration. MVP is usually benign, but complications include mitral regurgitation, endocarditis, and chordal rupture. MVP is usually asymptomatic in the absence of significant regurgitation, although there are reports that some patients experience chest pain, dyspnea, dizziness, and palpitations. Signs include a crisp mid-systolic click, followed by a late systolic murmur if regurgitation is present. Diagnosis is by physical examination and echocardiography. Prognosis is excellent in the absence of significant regurgitation, but chordal rupture and endocarditis may occur. No specific treatment is necessary unless significant mitral regurgitation is present.
(See also Overview of Cardiac Valvular Disorders.)
Mitral valve prolapse is common; prevalence is 2.4% in otherwise normal populations, depending on the echocardiographic criteria used (1). Females and males are affected equally; onset usually follows the adolescent growth spurt.
Reference
1. Freed LA, Levy D, Levine RA, et al. Prevalence and clinical outcome of mitral-valve prolapse. N Engl J Med 1999;341(1):1-7. doi:10.1056/NEJM199907013410101
Etiology of Mitral Valve Prolapse
Mitral valve prolapse is most often caused by:
Myxomatous degeneration of the mitral valve leaflets and chordae tendineae
In myxomatous degeneration, the fibrous collagen layer of the valve thins and mucoid (myxomatous) material accumulates. The chordae become longer and thinner and the valve leaflets enlarge and become rubbery. These changes result in floppy valve leaflets that can balloon back (prolapse) into the left atrium when the left ventricle contracts. Rupture of a degenerate chorda can allow part of the valve leaflet to flail into the atrium, which typically causes severe regurgitation.
Degeneration is usually idiopathic, although it may be inherited in an autosomal dominant or, rarely, in an X-linked recessive fashion. Myxomatous degeneration may also be caused by connective tissue or systemic rheumatic diseases (eg, Marfan syndrome, Ehlers-Danlos syndrome, adult polycystic kidney disease, osteogenesis imperfecta, pseudoxanthoma elasticum, systemic lupus erythematosus, polyarteritis nodosa) and muscular dystrophies. MVP is more common among patients with Graves disease, hypomastia, von Willebrand disease, sickle cell disease, and rheumatic heart disease.
Myxomatous degeneration less commonly affects the aortic or tricuspid valve, resulting in aortic or tricuspid prolapse.
Mitral annular disjunction (MAD) is partial detachment of the mitral annulus from adjacent ventricular myocardium during systole, allowing for hypermobility of the mitral valve. MAD is strongly associated with mitral valve prolapse and ventricular arrhythmias. Identification of MAD can alter the surgical technique used for mitral valve repair.
Mitral regurgitation (MR) due to mitral valve prolapse may occur in patients with apparently normal mitral valve leaflets (ie, nonmyxomatous) due to ischemic papillary muscle dysfunction or rheumatic chordal rupture. Transient MVP may occur when intravascular volume decreases significantly, as occurs in severe dehydration or sometimes during pregnancy (when the woman is recumbent and the gravid uterus compresses the inferior vena cava, reducing venous return).
Complications
Mitral regurgitation is the most common complication of mitral valve prolapse. MR may be acute (due to ruptured chordae tendineae causing flail mitral valve leaflets) or chronic.
Sequelae of MVP with MR include heart failure, infective endocarditis, and atrial fibrillation with thromboembolism. Whether MVP causes stroke or endocarditis independent of MR and atrial fibrillation is unclear.
Ventricular ectopy commonly occurs in mitral valve prolapse. Severe ventricular arrhythmias or high ectopic burden occurs in < 10% of cases and is associated with sudden cardiac death (1). Features associated with severe arrhythmias include severe myxomatous change of the valve leaflets, severe mitral regurgitation, myocardial fibrosis, and MAD (2). MAD is repaired surgically, not by transcatheter edge-to-edge repair (TEER).
Etiology references
1. Essayagh B, Sabbag A, Antoine C, et al. Presentation and Outcome of Arrhythmic Mitral Valve Prolapse. J Am Coll Cardiol 2020;76(6):637-649. doi:10.1016/j.jacc.2020.06.029
2. Essayagh B, Sabbag A, El-Am E, Cavalcante JL, Michelena HI, Enriquez-Sarano M. Arrhythmic mitral valve prolapse and mitral annular disjunction: pathophysiology, risk stratification, and management. Eur Heart J 2023;44(33):3121-3135. doi:10.1093/eurheartj/ehad491
Symptoms and Signs of Mitral Valve Prolapse
Most patients with mitral valve prolapse are asymptomatic. Some experience nonspecific symptoms (eg, chest pain, dyspnea, palpitations, dizziness, near syncope, migraines, anxiety) thought to be due to associated abnormalities in adrenergic signaling and sensitivity rather than to mitral valve pathology. In some patients, emotional stress precipitates palpitations, which may be a symptom of benign arrhythmias (atrial premature beats, paroxysmal atrial tachycardia, ventricular premature beats, complex ventricular ectopy).
Occasionally, patients present with mitral regurgitation. Rarely, patients present with endocarditis (eg, with fever, weight loss, thromboembolic phenomena) or stroke. Sudden death occurs in < 1%, most often in patients with ruptured or otherwise abnormal chordae tendineae and/or flail mitral valve leaflets. Death due to a ventricular arrhythmia is thought to be rare, but a significant fraction of patients with sudden cardiac death have no associated structural cardiac abnormality (1, 2).
Other physical findings associated with but not diagnostic of MVP include hypomastia, pectus excavatum, hypokyphosis (eg, straight back syndrome), and a narrow anteroposterior chest diameter.
Auscultation
Crisp mid-systolic click
Typically, mitral valve prolapse causes no visible or palpable cardiac signs.
MVP alone often causes a crisp mid-systolic click as the subvalvular apparatus abruptly tightens. The click is heard best with the diaphragm of the stethoscope over the left apex when the patient is in the left lateral decubitus position. MVP with MR causes a click with a late-systolic MR murmur. The click moves closer to the first heart sound (S1) with maneuvers that decrease left ventricle (LV) size (eg, sitting, standing, Valsalva maneuver); the same maneuvers cause an MR murmur to appear or become louder and last longer. These effects occur because decreasing LV size causes papillary muscles and chordae tendineae to pull together more centrally beneath the valve, resulting in quicker, more forceful prolapse with earlier, more severe regurgitation. Conversely, squatting or isometric handgrip delays the S1 click and shortens the MR murmur.
The systolic click may be confused with the click of congenital aortic stenosis; the latter may be distinguished because it occurs very early in systole and does not move with postural or LV volume changes. Other findings include a systolic honk or whoop, thought to be caused by valvular leaflet vibration; these findings are usually transient and may vary with respiratory phase. An early diastolic opening snap caused by return of the prolapsed valve to its normal position is rarely heard. In some patients, especially children, the findings of MVP may be more noticeable after exertion.

Symptoms and signs references
1. Han HC, Ha FJ, Teh AW, et al. Mitral Valve Prolapse and Sudden Cardiac Death: A Systematic Review. J Am Heart Assoc 2018;7(23):e010584. doi:10.1161/JAHA.118.010584
2. Nalliah CJ, Mahajan R, Elliott AD, et al. Mitral valve prolapse and sudden cardiac death: a systematic review and meta-analysis. Heart 2019;105(2):144-151. doi:10.1136/heartjnl-2017-312932
Diagnosis of Mitral Valve Prolapse
Echocardiography

© Springer Science+Business Media
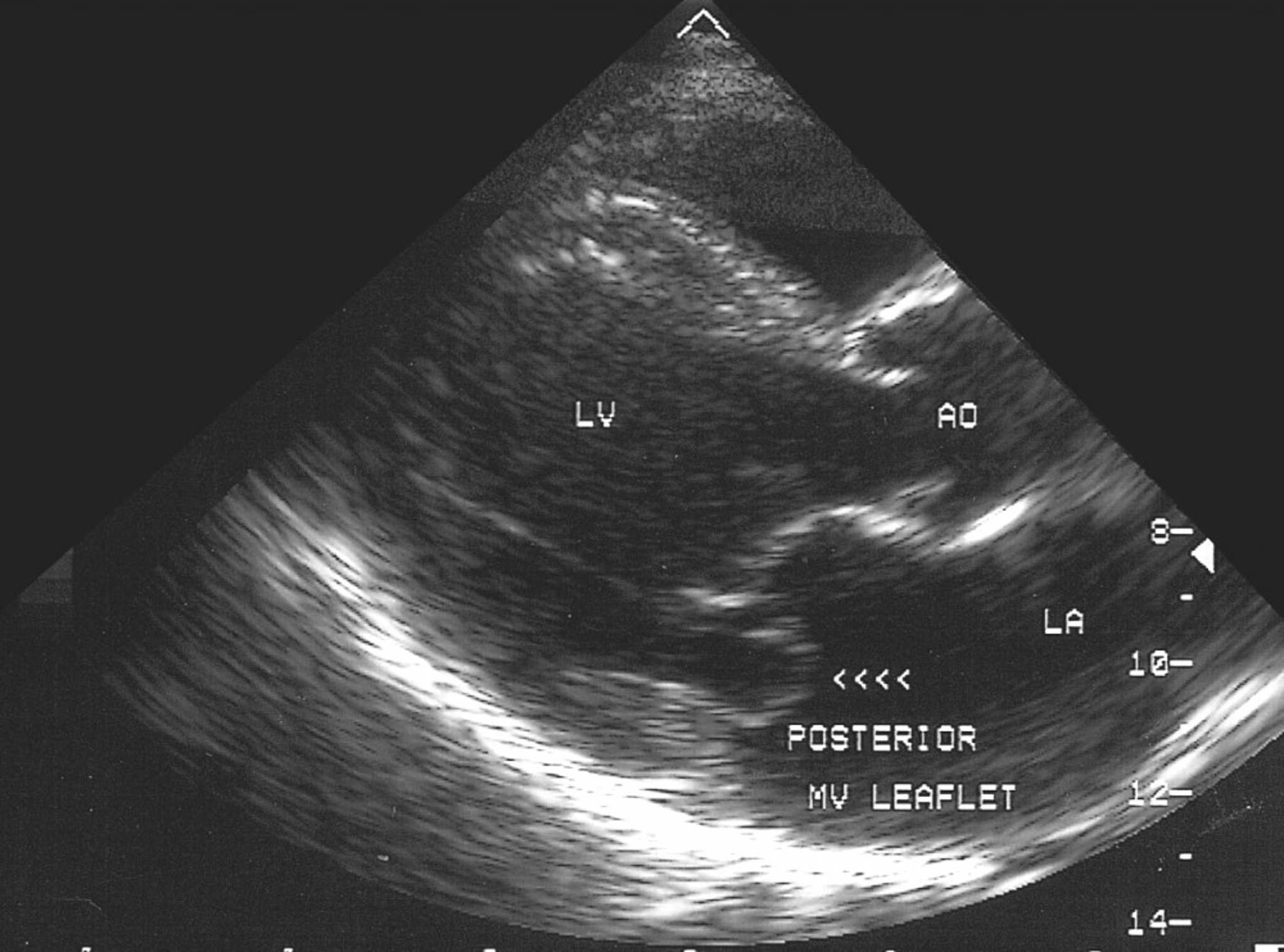
Diagnosis of mitral valve prolapse is suggested clinically and confirmed by echocardiography. Thickened (≥ 5 mm), redundant mitral valve leaflets are thought to indicate more extensive myxomatous degeneration and greater risk of endocarditis and mitral regurgitation.
Mitral annular disjunction is diagnosed echocardiographically when frame by frame analysis of the posterolateral annulus in the transthoracic parasternal long axis view reveals systolic separation of the annulus and ventricular myocardium by a few millimeters up to a centimeter.
Mitral annular disjunction is associated with increased risk of sudden death from arrhythmia, and ambulatory cardiac rhythm monitoring is recommended.
Treatment of Mitral Valve Prolapse
Usually none
Sometimes beta-blockers
Mitral valve prolapse does not usually require treatment.
Beta-blockers (eg, atenolol, propranolol) and calcium channel blockers (eg, verapamil) decrease symptoms due to associated ectopy but there is no evidence that they improve prognosis.Beta-blockers (eg, atenolol, propranolol) and calcium channel blockers (eg, verapamil) decrease symptoms due to associated ectopy but there is no evidence that they improve prognosis.
Treatment of atrial fibrillation may be required.
Treatment of mitral regurgitation depends on severity and associated left atrial and LV changes.
Antibiotic prophylaxis against endocarditis is not recommended, except after valve replacement.
Anticoagulants to prevent thromboembolism are recommended only for patients with atrial fibrillation or prior transient ischemic attack or stroke. (See also Anticoagulation for patients with a prosthetic cardiac valve or native valve disease.)
Prognosis for Mitral Valve Prolapse
Mitral valve prolapse is usually benign, but severe myxomatous degeneration of the valve can lead to MR. The risk of progression to severe MR is related both to severity at initial diagnosis and specific anatomic factors of the mitral valve itself (1, 2). The incidence of cardiac events (endocarditis, stroke, cardioembolic event) in patients with significant MR due to mitral valve prolapse may be as high as 4% annually (3). The prevalence of mitral valve prolapse is also higher in patients experiencing sudden cardiac death than in the general population, suggesting an association (4).
Prognosis references
1. Delling FN, Rong J, Larson MG, et al. Evolution of Mitral Valve Prolapse: Insights From the Framingham Heart Study. Circulation 2016;133(17):1688-1695. doi:10.1161/CIRCULATIONAHA.115.020621
2. Ma JI, Igata S, Strachan M, et al. Predictive Factors for Progression of Mitral Regurgitation in Asymptomatic Patients With Mitral Valve Prolapse. Am J Cardiol 2019;123(8):1309-1313. doi:10.1016/j.amjcard.2019.01.026
3. Mecarocci V, Mori F. P210Long- term outcome of primary mitral valve prolapse: results from a population of 250 patients referred to a tertiary cardiovascular center. Eur Heart J Cardiovasc Imaging 2016;17(suppl_2):ii29-ii37. doi:10.1093/ehjci/jew236.001
4. Nalliah CJ, Mahajan R, Elliott AD, et al. Mitral valve prolapse and sudden cardiac death: a systematic review and meta-analysis. Heart 2019;105(2):144-151. doi:10.1136/heartjnl-2017-312932
Key Points
Mitral valve prolapse is most often caused by idiopathic myxomatous degeneration of the mitral valve and chordae tendineae.
Mitral regurgitation (MR) is the most common complication.
Heart sounds often include a sharp, mid-systolic click that occurs earlier with the Valsalva maneuver.
Prognosis is usually benign unless MR develops, in which case there is increased risk of heart failure, atrial fibrillation, stroke, and infective endocarditis.
Treatment is not needed unless significant MR develops.
Drugs Mentioned In This Article






