


Laryngeal mask airway (LMA) ventilation is a method for providing rescue ventilation to unconscious patients or patients without a gag reflex that is technically easier than use of most other effective ventilatory methods. It is used by anesthesiologists in many settings that previously required endotracheal intubation.
(See also Airway Establishment and Control and Airway and Respiratory Devices.)
The laryngeal mask airway (LMA) is a commonly used supraglottic airway. The LMA is an orally introduced supraglottic airway tube with a cuffed mask at one end that forms a low-pressure seal around the laryngeal inlet. LMA ventilation has several advantages over other methods.
Unlike endotracheal tubes, LMAs can be successfully inserted blindly and by operators with only basic training.
Unlike bag-valve-mask (BVM) ventilation, LMAs avoid the difficulties of attaining and maintaining an adequate face-mask seal. They bypass soft tissue obstruction of the upper airway, and they cause less gastric insufflation than BVM ventilation.
Some available types of LMAs allow passage of an endotracheal tube (intubating LMAs) or a gastric decompression tube. Some have a fixed, anatomically correct shape that further optimizes ease of insertion. Some newer mask designs replace the inflatable cuff with a gel–filled cuff that molds to the airway.
LMAs, like the other supraglottic airways (eg, King laryngeal tube and esophageal-tracheal double lumen tube [Combitube]), are temporary airways that must, after several hours, be removed or be replaced by a definitive airway, such as an endotracheal tube or surgical airway (cricothyrotomy or tracheostomy).
Indications for Laryngeal Mask Airway Insertion
Apnea, severe respiratory failure, or impending respiratory arrest in which endotracheal intubation cannot be accomplished
Certain elective anesthesia cases
LMAs are useful in situations where bag-valve-mask ventilation is difficult:
Patients with severe facial deformity (traumatic or natural), thick beard, or other factors that interfere with the face mask seal
Contraindications to Laryngeal Mask Airway Insertion
Absolute contraindications
There is no medical contraindication to providing ventilatory support to a patient; however, a legal contraindication (do-not-resuscitate order or specific advance directive) may be in force
Maximum mouth opening between incisors < 2 cm (nasotracheal intubation or a surgical airway would be indicated in this case)
Impassable upper airway obstruction (surgical airway would be indicated in this case)
Relative contraindications
Consciousness or presence of a gag reflex (patients should be unconscious or receive drugs to aid intubation, such as a sedative and a paralytic agent, prior to LMA insertion)
Increased risk of regurgitation in patients with prolonged prior BVM ventilation, obesity, pregnancy > 10 weeks, upper gastrointestinal issues (eg, previous surgery, bleeding, hiatal hernia, gastroesophageal reflux disease, peptic ulcer disease), and in patients who have not fasted. In emergencies, use of an LMA can proceed even with these relative contraindications.
Need for high pressure ventilation (the tighter seal of an endotracheal tube or a special LMA designed to form a tighter seal is needed for patients with excessive airflow resistance in the infraglottic airways or lungs)
Complications of Laryngeal Mask Airway Insertion
Complications include
Vomiting and aspiration
Tongue edema due to prolonged placement or balloon overinflation
Dental or oropharyngeal soft tissue trauma during insertion
Equipment for Laryngeal Mask Airway Insertion
Gloves, mask, gown, and eye protection (ie, universal precautions)
30- to 60-mL syringe
Sterile water-soluble lubricant or anesthetic jelly
Laryngeal mask airway
Bag-valve apparatus
Oxygen source (100% oxygen, 15 L/minute)
Suctioning apparatus to clear the pharynx as needed
Pulse oximeter, capnometer (end-tidal carbon dioxide monitor), and appropriate sensors
Equipment for alternate methods of airway control should LMA insertion fail (eg, equipment for bag-valve-mask ventilation, endotracheal intubation, cricothyrotomy)
Additional Considerations for Laryngeal Mask Airway Insertion
The inflatable cuff around the rim of the mask forms a low-pressure seal around the laryngeal inlet that allows positive pressure ventilation.
Use low-pressure ventilation with a LMA to prevent air from escaping the low-pressure seal and causing gastric insufflation.
If the seal is inadequate, lower the cuff pressure somewhat. If this approach does not work, a larger mask size should be tried. Overinflation of the cuff will make a poor seal worse.
LMAs do not protect the airway from aspiration. However, some types of LMA feature improved laryngeal seals as well as ports for insertion of gastric decompression tubes.
Relevant Anatomy for Laryngeal Mask Airway Insertion
Aligning the ear with the sternal notch may help open the upper airway and establishes the best position to view the airway if endotracheal intubation becomes necessary.
The degree of head elevation that best aligns the ear and sternal notch varies (eg, none in children because in children the occiput is relatively large, but a large degree in patients with obesity).
Positioning for Laryngeal Mask Airway Insertion
Optimal patient position for LMA insertion is the sniffing position.
The operator may stand at the head of the stretcher while an assistant stands at the side.
The sniffing position is used only in the absence of cervical spine injury:
Position the patient supine on the stretcher.
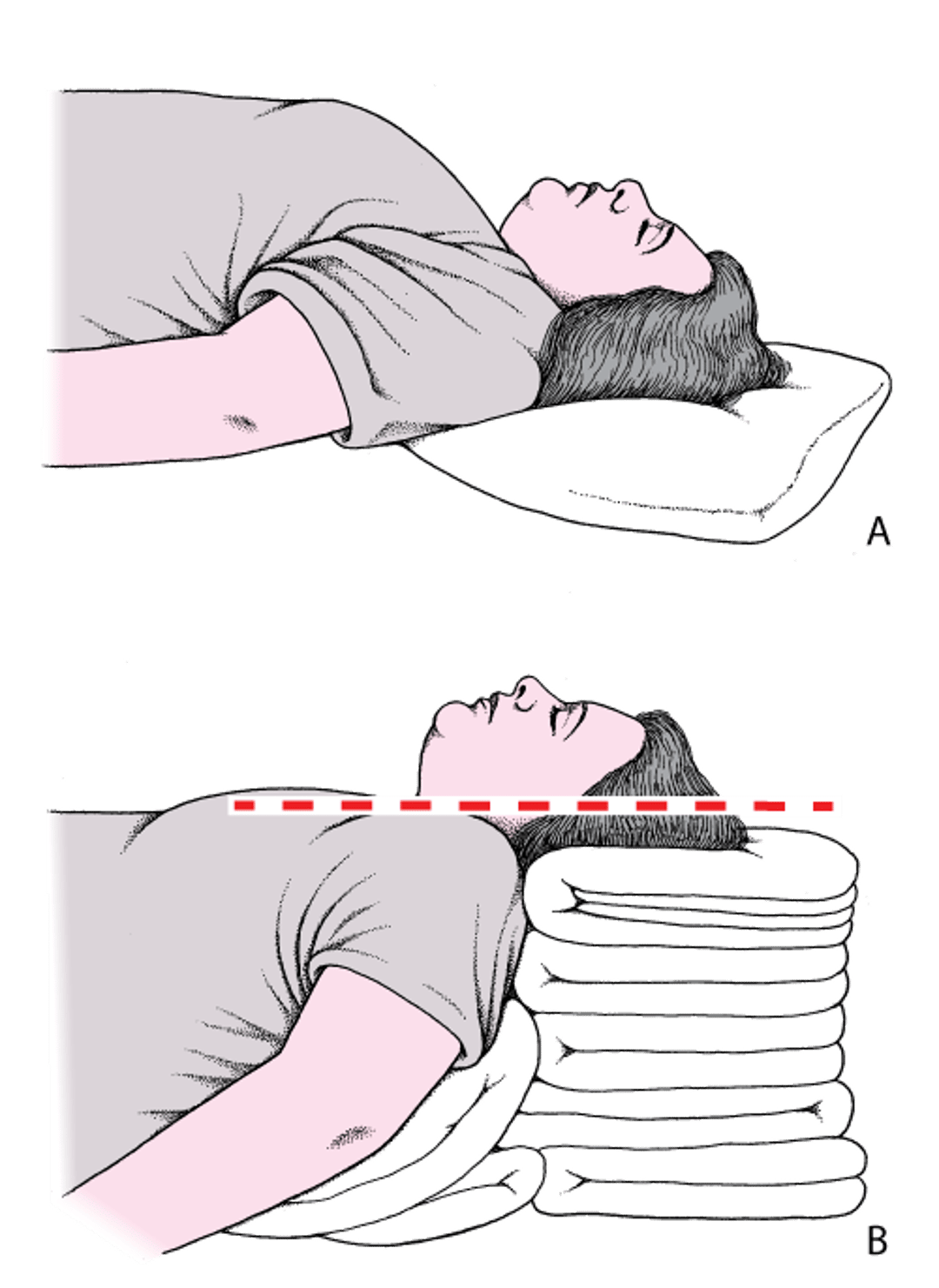
Place folded towels or other materials under the head, neck, and shoulders, flexing the neck to elevate the head until the external auditory meatus lies in the same horizontal plane as the sternal notch. Tilt the head so that the face aligns on a parallel horizontal plane; this second plane will be above the first. In patients with obesity, many folded towels or a commercial ramp device may be needed to sufficiently elevate the shoulders and neck (see figure head and neck positioning to open the airway).
Head and neck positioning to open the airway
A: The head is flat on the stretcher; the airway is constricted. B: Establishing the sniffing position, the ear and sternal notch are aligned, with the face parallel to the ceiling, opening the airway. Adapted from Levitan RM, Kinkle WC: The Airway Cam Pocket Guide to Intubation, ed. 2. Wayne (PA), Airway Cam Technologies, 2007. |

If cervical spine injury is a possibility:
Position the patient supine or at a slight incline on the stretcher. Avoid moving the neck and use only the jaw thrust maneuver or chin lift without head tilt to manually facilitate opening the upper airway.
LMAs that are anatomically contoured can be inserted without any neck manipulation or need for finger insertion into the mouth. They may cause posterior pressure on the cervical spine; however, they are generally considered safe for patients with unstable cervical spine injury.
Step-by-Step Description of Laryngeal Mask Airway Insertion
Do not allow a patient to awaken during insertion or ventilation with a laryngeal mask airway. If necessary, prevent the patient from waking up or gagging by using sedatives and/or paralytic medications or remove the airway as clinically indicated.
Select the appropriately sized LMA and note the maximum cuff inflation volume. The size and maximum inflation volume are usually printed on the side of the tube. Generally, size #4 is suitable for adults weighing 50 to70 kg and size #5 is suitable for adults weighing 70 to 100 kg.
Inflate and deflate the cuff to check its volume and ensure there are no leaks.
With the cuff completely deflated, apply a small amount of sterile, water-soluble lubricant to the posterior surface of the distal mask and cuff.
Pre-oxygenate the patient with bag-valve-mask ventilation if possible.
Flex the patient’s neck, lift the chin, and maintain manual counter-pressure on the occiput as needed when you insert the tube.
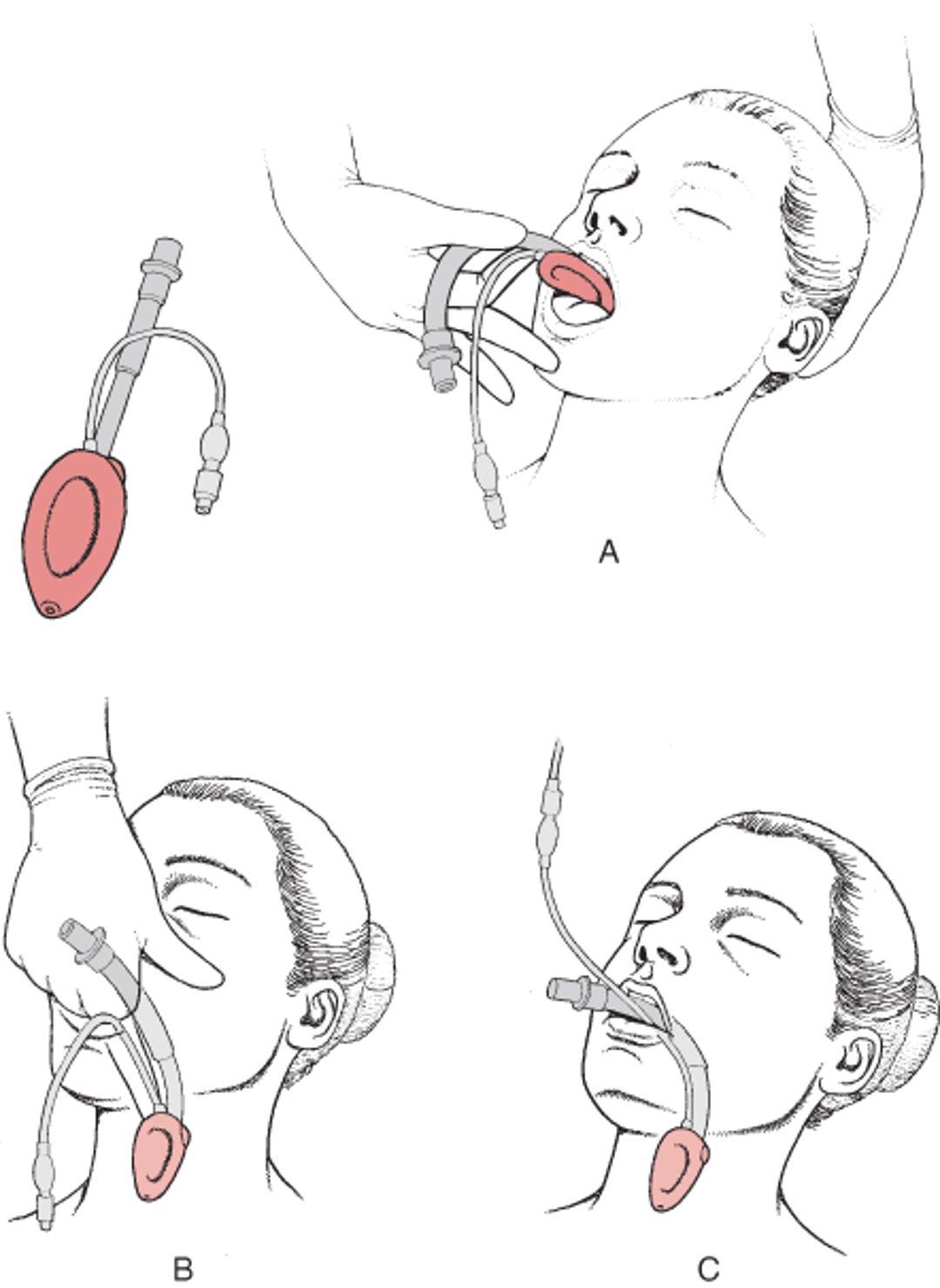
Insert the LMA (see figure Laryngeal mask airway) into the mouth, manually guiding it along the hard and soft palates and into the throat by pushing with the index or long finger in the v-shaped notch where the tube attaches to the mask. Push the tube cephalad, so the lubricated posterior surface of the mask follows the curve of the hard and soft palates. The mask should enter the hypopharynx along the posterior wall, to avoid deflecting and possibly causing a tube obstruction by the epiglottis. At the proper distance of insertion (as confirmed by markings on the tube), the mask will overlie the laryngeal opening, and the tip of the mask will meet definitive resistance to further insertion (at the top of the esophageal opening) .
Release your hand from the tube before inflating the cuff.
Inflate the cuff. Use half the recommended maximum cuff volume. As the mask seats over the glottic area, the tube will protrude 1 to 2 cm out of the mouth.
Connect a bag-valve apparatus to the tube.
Begin ventilation (8 to 10 breaths/minute, each about 500 mL and lasting about 1 second).
Assess lung ventilation by auscultation and chest rise.
Check end-tidal carbon dioxide to confirm placement.
Fix the tube in place as appropriate.
Laryngeal Mask Airway (LMA)
The LMA is a tube with an inflatable cuff that is inserted into the oropharynx. A: The deflated cuff is inserted into the mouth. B: With the index finger, the cuff is guided into place above the larynx. C: Once in place, the cuff is inflated. Some cuffs use a gel that molds to the airway rather than an inflatable cuff. |

Warnings and Common Errors for Laryngeal Mask Airway Insertion
Do not allow a patient to awaken during insertion or ventilation with a supraglottic or endotracheal airway. If necessary, prevent the patient from waking up or gagging (using sedative and/or paralytic medications) or remove the airway as clinically indicated.
Do not over-inflate the cuff. Generally, start with half the maximal cuff volume and adjust as necessary.
Tips and Tricks for Laryngeal Mask Airway Insertion
To improve difficult or inadequate LMA ventilation:
Adjust the cuff volume. Try both lower and higher volumes (a poor cuff seal may be caused by either too low or too high cuff volumes).
Adjust patient positioning while doing bag-valve ventilation to help make ventilation easier.
Try a better configured sniffing position, a chin-to chest position, jaw thrust, or chin-lift maneuvers.
Do the up-down maneuver. Withdraw the LMA 5 to 6 cm, without deflating the cuff, and then reinsert it to release an epiglottis trapped under the cuff or inside the mask.
Rotate the LMA deeper into the hypopharynx and elevate the handle toward the ceiling.
Deflate the cuff and remove the LMA. Then repeat LMA insertion, using the same LMA or one of a larger size.
Consider using another airway, such as an intubating laryngeal mask airway, King laryngeal tube, endotracheal intubation, or a surgical airway.







