



Acute hypoxemic respiratory failure is defined as severe hypoxemia (PaO2 < 60 mmHg) without hypercapnia. It is caused by intrapulmonary shunting of blood with resulting in ventilation-perfusion (V/Q) mismatch due to airspace filling or collapse (eg, cardiogenic or non-cardiogenic pulmonary edema, pneumonia, pulmonary hemorrhage) or possibly airway disease (eg, sometimes asthma, COPD); or by intracardiac shunting of blood from the right-sided to the left-sided circulation. Findings include dyspnea and tachypnea. Diagnosis is by arterial blood gas measurement and chest x-ray. Management includes various noninvasive oxygen strategies such as high-flow oxygen, continuous positive airway pressure, or other noninvasive oxygen strategies, or invasive mechanical ventilation, when necessary.

")
")




(See also Overview of Mechanical Ventilation.)

Etiology of AHRF
Airspace filling in acute hypoxemic respiratory failure (AHRF) may result from
Elevated alveolar capillary hydrostatic pressure, as occurs in left ventricular failure (causing pulmonary edema) or hypervolemia
Increased alveolar capillary permeability, as occurs in any of the conditions predisposing to acute respiratory distress syndrome (ARDS)
Blood (as occurs in diffuse alveolar hemorrhage) or inflammatory exudates (as occur in pneumonia or other inflammatory lung conditions)
Right-to-left intracardiac shunts, in which deoxygenated venous blood bypasses the lungs and enters the systemic circulation, usually occur as a long-term complication of large, untreated left-to-right shunts (eg, due to patent foramen ovale, atrial septal defect). This phenomenon is termed Eisenmenger syndrome. This discussion focuses on refractory hypoxemia due to pulmonary causes.
Pathophysiology of AHRF
ARDS
ARDS is a diffuse, inflammatory lung injury that is a cause of AHRF (1). ARDS is divided into 3 categories of severity: mild, moderate, and severe based on oxygenation defects and clinical criteria. The mild category corresponds to the previous category termed acute lung injury (ALI).
Berlin Definition of ARDS
ARDS Category | Oxygenation |
|---|---|
Level of severity | |
Mild | 200 mm Hg < PaO2/FIO2 ≤ 300 mm Hg* with PEEP or CPAP ≥ 5 cm H2O |
Moderate | 100 mm Hg < PaO2/FIO2 ≤ 200 mm Hg with PEEP ≥ 5 cm H2O |
Severe | PaO2/FIO2 ≤ 100 mm Hg with PEEP ≥ 5 cm H2O |
Clinical criteria | |
Timing | Onset within 1 week of known insult or of new or worsening respiratory symptoms |
Imaging (x-ray or CT of chest) | Bilateral opacities not fully explained by effusions, lobar or lung collapse, or nodules |
Origin of edema | Respiratory failure not fully explained by heart failure or fluid overload |
* PaO2 in mm Hg; FIO2 in decimal fraction (eg, 0.5). | |
ARDS = acute respiratory distress syndrome; CPAP = continuous positive airway pressure; FIO2 = fraction of inspired oxygen; PaO2 = partial pressure of arterial oxygen; PEEP = positive end-expiratory pressure. | |
Adapted from ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, et al: Acute respiratory distress syndrome: The Berlin definition. Journal of the American Medical Association 307:2526–2533, 2012. doi: 10.1001/jama.2012.5669 | |
Diagnosis of ARDS based on the Berlin definition is challenging in the setting of changing clinical practice (ie, increasing use of high-flow nasal cannula and ubiquitous use of pulse oximetry) and often cannot be applied in low-resource settings (due to lack of routine access to chest radiography, arterial blood gas sampling, and mechanical ventilation). Therefore, a consensus panel has proposed modifying the Berlin definition to include ultrasonography for confirmation of bilateral opacities; use of positive end-expiratory pressure (PEEP) and high flow oxygen (of at least 30 L/minute); and oxygen saturation/fraction of inspired oxygen (FiO2) ≤ 315 if the oxygen saturation is ≤ 97% (2). The new definitions for low-resource settings do not classify severity.
In ARDS, pulmonary or systemic inflammation leads to release of cytokines and other proinflammatory molecules. The cytokines activate alveolar macrophages and recruit neutrophils to the lungs, which in turn release leukotrienes, oxidants, platelet-activating factor, and proteases, contributing to tissue damage in the lungs as well as other organs (biotrauma). These substances damage capillary endothelium and alveolar epithelium, disrupting the barriers between capillaries and airspaces. Edema fluid, protein, and cellular debris flood the airspaces and interstitium, causing disruption of surfactant, airspace collapse, ventilation-perfusion mismatch, shunting, and pulmonary hypertension. The airspace collapse more commonly occurs in dependent lung zones. This early phase of ARDS is termed exudative. Later, there is proliferation of alveolar epithelium and fibrosis, constituting the fibro-proliferative phase.
Causes of ARDS may involve direct or indirect lung injury.
Common causes of direct lung injury are
Less common causes of direct lung injury are
Common causes of indirect lung injury include
Trauma with prolonged hypovolemic shock
Less common causes of indirect lung injury include
Massive blood transfusion (eg, > 15 units)
Cardiopulmonary bypass
Drug overdose or toxicity (eg, aspirin, cocaine, opioids, phenothiazines, tricyclic antidepressants)
Neurogenic pulmonary edema due to stroke, seizure, head trauma, anoxia
Radiographic contrast (rare)
Sepsis and pneumonia account for about 60% of cases of ARDS.
Refractory hypoxemia
Whatever the cause of airspace filling in AHRF, flooded or collapsed airspaces allow no inspired gas to enter, so the blood perfusing those alveoli remains at the mixed venous oxygen content no matter how high the FIO2. This effect ensures constant admixture of deoxygenated blood into the pulmonary vein and hence arterial hypoxemia. In contrast, hypoxemia that results from ventilating alveoli that have less ventilation than perfusion (ie, low ventilation-to-perfusion ratios as occur in asthma or chronic obstructive pulmonary disease [COPD] and, to some extent, in ARDS) is readily corrected by supplemental oxygen; thus, respiratory failure caused by asthma or COPD is more often ventilatory than hypoxemic respiratory failure.
Pathophysiology references
1. Grasselli G, Calfee CS, Camporota L, et al: ESICM guidelines on acute respiratory distress syndrome: definition, phenotyping and respiratory support strategies. Intensive Care Med 49(7):727–759, 2023. doi:10.1007/s00134-023-07050-7
2. Matthay MA, Arabi Y, Arroliga AC, et al. A New Global Definition of Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med 2024;209(1):37-47. doi:10.1164/rccm.202303-0558WS
Symptoms and Signs of AHRF
Acute hypoxemia (see also Oxygen Desaturation) may cause dyspnea, restlessness, and anxiety. Signs include confusion or alteration of consciousness, cyanosis, tachypnea, tachycardia, and diaphoresis. Cardiac arrhythmia and coma can result.
Inspiratory opening of closed airways causes crackles, detected during chest auscultation; the crackles are typically diffuse but sometimes worse at the lung bases, particularly in the left lower lobe because the weight of the heart increases atelectasis. Jugular venous distention occurs with high levels of positive end-expiratory pressure (PEEP) or right ventricular failure.
Diagnosis of AHRF
Chest x-ray, pulse oximetry, and arterial blood gas (ABG) measurement
Clinical definition (see table Berlin Definition of ARDS)
Hypoxemia is usually first recognized using pulse oximetry. Patients with low oxygen saturation should have a chest x-ray and be treated with supplemental oxygen while awaiting test results. Not all patients with low oxygen saturation require ABG measurement.
If supplemental oxygen does not improve the oxygen saturation to > 90%, right-to-left shunting of blood should be suspected. An obvious alveolar infiltrate on chest x-ray implicates alveolar flooding as the cause, rather than an intracardiac shunt. However, at the onset of illness, hypoxemia can occur before changes are seen on x-ray.
Once AHRF is diagnosed, the cause must be determined. Both pulmonary and extrapulmonary causes should be considered. Sometimes a known ongoing disorder (eg, acute myocardial infarction, pancreatitis, sepsis) is an obvious cause. In other cases, history is suggestive; pneumonia is suspected in a patient who is immunocompromised, and alveolar hemorrhage is suspected after bone marrow transplantation or in a patient with a systemic rheumatic disease. Frequently, however, patients who are critically ill have received a large volume of IV fluids for resuscitation, and high-pressure AHRF (eg, caused by ventricular failure or fluid overload) resulting from treatment must be distinguished from an underlying low-pressure AHRF (eg, caused by sepsis or pneumonia).


© 2017 Elliot K. Fishman, MD.
High-pressure pulmonary edema due to left ventricular failure is suggested by a third heart sound (S3), jugular venous distention, and peripheral edema on examination and by the presence of diffuse central infiltrates, cardiomegaly, and an abnormally wide vascular pedicle on chest x-ray. The diffuse, bilateral infiltrates of ARDS are generally more peripheral. Focal infiltrates are typically caused by lobar pneumonia, atelectasis, or lung contusion. Although echocardiography may show left ventricular dysfunction, implying a cardiac origin, this finding is not specific because sepsis can also reduce myocardial contractility.


This upright chest x-ray shows diffuse bilateral opacities characteristic of acute respiratory distress syndrome (ARDS).
By permission of the publisher. From Herdegen J, Bone R. In Atlas of Infectious Diseases: Pleuropulmonary and Bronchial Infections. Edited by G Mandell (series editor) and MS Simberkoff. Philadelphia, Current Medicine, 1996.

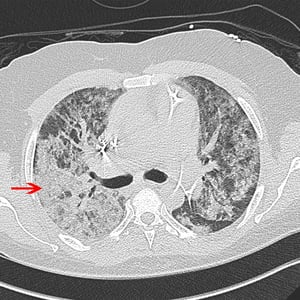
The red arrow points to the diffuse alveolar opacities in a patient with ARDS (acute respiratory distress syndrome). The patient also has cardiomegaly, a triple lead automated implantable cardioverter defibrillator with tips in the right ventricle, and a Swan Ganz catheter with tip in the pulmonary artery.
© 2017 Elliot K. Fishman, MD.

The arrow points to some of the diffuse alveolar opacities in a patient with ARDS (acute respiratory distress syndrome).
© 2017 Elliot K. Fishman, MD.
This upright chest x-ray shows diffuse bilateral opacities characteristic of acute respiratory distress syndrome (ARDS).
By permission of the publisher. From Herdegen J, Bone R. In Atlas of Infectious Diseases: Pleuropulmonary and Bronchial Infections. Edited by G Mandell (series editor) and MS Simberkoff. Philadelphia, Current Medicine, 1996.
The red arrow points to the diffuse alveolar opacities in a patient with ARDS (acute respiratory distress syndrome). The patient also has cardiomegaly, a triple lead automated implantable cardioverter defibrillator with tips in the right ventricle, and a Swan Ganz catheter with tip in the pulmonary artery.
© 2017 Elliot K. Fishman, MD.
The arrow points to some of the diffuse alveolar opacities in a patient with ARDS (acute respiratory distress syndrome).
© 2017 Elliot K. Fishman, MD.
When ARDS is diagnosed but the cause is not obvious (eg, trauma, sepsis, severe pulmonary infection, pancreatitis), a review of illicit drugs, medications, and recent diagnostic tests, procedures, and treatments may suggest an unrecognized cause, such as use of a radiographic contrast agent, air embolism, or transfusion. When no predisposing cause can be uncovered, some experts recommend doing bronchoscopy with bronchoalveolar lavage to exclude alveolar hemorrhage and eosinophilic pneumonia and, if this procedure is not revealing, a lung biopsy to exclude other disorders (eg, hypersensitivity pneumonitis, acute interstitial pneumonia).
Treatment of AHRF
Noninvasive oxygenation support
Mechanical ventilation if oxygen saturation is < 90% on high-flow oxygen
AHRF is usually initially treated with 70 to 100% oxygen delivered noninvasively (eg, with a non-rebreather face mask) (1). However, the use of noninvasive oxygen support, such as high-flow nasal cannula (HFNC) and noninvasive positive pressure ventilation (NIPPV), for the initial management of acute hypoxemic respiratory failure increased during the COVID-19 pandemic due to the potential ventilator sparing effects.
Noninvasive oxygen support may avoid endotracheal intubation and its complications; however, spontaneous breathing with excessive effort may induce lung damage (known as patient self-inflicted lung injury). One clinical trial comparing the efficacy of HFNC, face mask NIPPV, and standard oxygen for the prevention of endotracheal intubation suggested that HFNC may prevent endotracheal intubation in patients with a PaO2/FiO2 ratio < 200 (2). There was increased 90-day mortality noted in patients randomized to face mask NIPPV and standard oxygen compared to HFNC. One explanation for this excess mortality in the face mask NIPPV group may be that excessive tidal volumes worsen lung injury.
Another small clinical trial comparing oxygen delivery by helmet with face mask found lower rates of endotracheal intubation and mortality when the helmet was used (3). There are limited data comparing the use of helmet NIPPV to HFNC in patients with COVID-19–related acute hypoxemic respiratory failure, suggesting that helmet NIPPV may reduce endotracheal intubation rates but does not improve days free of respiratory support (4). Thus, there is no conclusive evidence indicating superiority of either approach for the initial management of hypoxemia. Given concerns regarding increased mortality possibly due to delayed intubation in patients with a PaO2/FiO2 ratio ≤ 150, noninvasive oxygen support in moderate-to-severe hypoxemia should be used with caution (5).
If noninvasive oxygenation support does not result in oxygen saturation > 90%, mechanical ventilation probably should be considered. Specific management varies by underlying condition.
Mechanical ventilation in cardiogenic pulmonary edema
Mechanical ventilation (see also Overview of Mechanical Ventilation) benefits the failing left ventricle in several ways. Positive inspiratory pressure reduces left and right ventricular preload and left ventricular afterload and reduces the work of breathing. Reducing the work of breathing may allow redistribution of a limited cardiac output away from overworked respiratory muscles. Expiratory pressure (expiratory positive airway pressure [EPAP] or PEEP) redistributes pulmonary edema from alveoli to the interstitium, allowing more alveoli to participate in gas exchange. (However, in liberating patients with low cardiac output from mechanical ventilation to noninvasive ventilation, the transition from positive to negative airway pressure can increase afterload and result in acute pulmonary edema or worsening hypotension.)
Noninvasive positive pressure ventilation (NIPPV), whether continuous positive pressure ventilation or bilevel ventilation, is useful in averting endotracheal intubation in many patients in whom pharmacotherapy often leads to rapid improvement. Typical settings are inspiratory positive airway pressure (IPAP) of 10 to 15 cm H2O and EPAP of 5 to 8 cm H2O.
Conventional mechanical ventilation can use several ventilator modes. Most often, assist-control (A/C) is used in the acute setting, when full ventilatory support is desired. Initial settings are tidal volume of 6 to 8 mL/kg ideal body weight, respiratory rate of 25/minute, FIO2 of 1.0, and PEEP of 5 to 8 cm H2O. PEEP may then be titrated upward in 2.5-cm H2O increments while the FIO2 is decreased to nontoxic levels.
Pressure support ventilation can also be used (with similar levels of PEEP). The initial inspiratory airway pressure delivered should be sufficient to rest the respiratory muscles as judged by subjective patient assessment, respiratory rate, and accessory muscle use. Typically, a pressure support level of 10 to 20 cm H2O over PEEP is required.
Mechanical ventilation in ARDS
Nearly all patients with ARDS require mechanical ventilation (1), which, in addition to improving oxygenation, reduces oxygen demand by resting respiratory muscles. Targets include
Plateau alveolar pressures < 30 cm H2O (factors that potentially decrease chest wall and abdominal compliance considered)
Tidal volume of 6 mL/kg ideal body weight to minimize further lung injury
FIO2 as low as is possible to maintain adequate oxygen saturation to minimize possible oxygen toxicity
PEEP should be high enough to maintain open alveoli and minimize FIO2 until a plateau pressure of 28 to 30 cm H2O is reached. Patients with moderate to severe ARDS are the most likely to have mortality reduced by use of higher PEEP.
Noninvasive positive pressure ventilation (NIPPV) is occasionally useful in ARDS. However, compared with treatment of cardiogenic pulmonary edema, higher levels of support for a longer duration are often required, and EPAP of 8 to 12 cm H2O is often necessary to maintain adequate oxygenation. Achieving this expiratory pressure requires inspiratory pressures > 18 to 20 cm H2O, which are poorly tolerated; maintaining an adequate seal becomes difficult, the mask becomes more uncomfortable, and skin necrosis and gastric insufflation may occur. Also, patients treated with NIPPV who subsequently need intubation have generally progressed to a more advanced condition than if they had been intubated earlier; thus, critical desaturation is possible at the time of intubation. Intensive monitoring and careful selection of patients for NIPPV are required.
Conventional mechanical ventilation in ARDS previously focused on normalizing arterial blood gas values. It is clear that ventilating with lower tidal volumes reduces mortality. Accordingly, in most patients, tidal volume should be set at 6 mL/kg ideal body weight (see sidebar Initial Ventilator Management in ARDS). This setting necessitates an increase in respiratory rate, even up to 35/minute, to produce sufficient alveolar ventilation to allow for adequate carbon dioxide removal. On occasion, however, respiratory acidosis develops, some degree of which is accepted for the greater good of limiting ventilator-associated lung injury and is generally well tolerated, particularly when pH is ≥ 7.15. If pH drops below 7.15, bicarbonate infusion may be helpful. Similarly, oxygen saturation below "normal" levels may be accepted; target saturation of 88 to 95% limits exposure to excessive toxic levels of FiO2 and still has survival benefit.
Because hypercapnia or low tidal volume alone may cause dyspnea and cause the patient to breathe in a fashion that is not coordinated with the ventilator, analgesics (fentanyl or morphine) and sedatives (eg, propofol initiated at 5 mcg/kg/minute and increasing to effect up to 50 mcg/kg/minute; because of the risk of hypertriglyceridemia, triglyceride levels should be checked every 48 hours) may be needed (see also Because hypercapnia or low tidal volume alone may cause dyspnea and cause the patient to breathe in a fashion that is not coordinated with the ventilator, analgesics (fentanyl or morphine) and sedatives (eg, propofol initiated at 5 mcg/kg/minute and increasing to effect up to 50 mcg/kg/minute; because of the risk of hypertriglyceridemia, triglyceride levels should be checked every 48 hours) may be needed (see alsoSedation and Comfort). Sedation is preferred to neuromuscular blockade because blockade still requires sedation and may cause residual weakness.
PEEP improves oxygenation in ARDS by increasing the volume of aerated lung through alveolar recruitment, permitting the use of a lower FIO2. The optimal level of PEEP and the way to identify it have been debated. Routine use of recruitment maneuvers (eg, titration of PEEP to maximal pressure of 35 to 40 cm H2O and held for 1 minute) followed by decremental PEEP titration was found to be associated with an increased 28-day mortality (6). Therefore, many clinicians simply use the least amount of PEEP that results in an adequate arterial oxygen saturation on a nontoxic FIO2. In most patients, this level is a PEEP of 8 to 15 cm H2O, although, occasionally, patients with severe ARDS require levels > 20 cm H2O. In these cases, close attention must be paid to other means of optimizing oxygen delivery and minimizing oxygen consumption.
The best indicator of alveolar overdistention is measurement of a plateau pressure through an end-inspiratory hold maneuver; plateau pressure should be checked every 4 hours and after each change in PEEP or tidal volume. The target plateau pressure is < 30 cm H2O in patients with normal chest wall compliance. To avoid hypoventilation, the plateau pressure target may need to be higher in patients with abnormal chest wall compliance (eg, ascites, pleural effusion, acute abdominal distension, chest trauma). In contrast, if the plateau pressure exceeds 30 cm H2O and there is no problem with the chest wall that could be contributing, the physician should reduce the tidal volume in increments of 0.5 mL/kg to 1.0 mL/kg as tolerated to a minimum of 4 mL/kg, raising the respiratory rate to compensate for the reduction in minute ventilation and inspecting the ventilator waveform display to ensure that full exhalation occurs. The respiratory rate may often be raised as high as 35/minute before overt gas trapping due to incomplete exhalation results. If plateau pressure is < 25 cm H2O and tidal volume is < 6 mL/kg, tidal volume may be increased to 6 mL/kg or until plateau pressure is > 25 cm H2O.
Some investigators believe pressure control ventilation protects the lungs better than volume control, but supportive data are lacking, and it is the peak pressure rather than the plateau pressure that is being controlled. With pressure control ventilation, because the tidal volume will vary as the patient's lung compliance evolves, it is necessary to continually monitor the tidal volume and adjust the inspiratory pressure to ensure that the patient is not receiving too high or too low a tidal volume.
Prone positioning improves oxygenation in some patients by allowing recruitment of nonventilating lung regions. Some evidence suggests this positioning substantially improves survival (7, 8). Interestingly, the mortality benefit from prone positioning is not related to the degree of hypoxemia or the extent of gas exchange abnormality but possibly to mitigating ventilator-associated lung injury.
Optimal fluid management in patients with ARDS balances the requirement for an adequate circulating volume to preserve end-organ perfusion with the goal of lowering preload and thereby limiting transudation of fluid in the lungs. A large multicenter trial has shown that a conservative approach to fluid management, in which less fluid is given, shortens the duration of mechanical ventilation and length of stay in the intensive care unit when compared with a more liberal strategy. However, there was no difference in survival between the 2 approaches, and use of a pulmonary artery catheter also did not improve outcome (9). Patients who are not in shock are candidates for such an approach but should be monitored closely for evidence of decreased end-organ perfusion, such as hypotension, oliguria, thready pulses, or cool extremities.
A definitive pharmacologic treatment for ARDS that reduces morbidity and mortality remains elusive. Inhaled nitric oxide, surfactant replacement, activated protein C (drotrecogin alfa), and many other agents directed at modulating the inflammatory response have been studied and found not to reduce morbidity or mortality (10). Data on the efficacy for corticosteroid efficacy in ARDS are inconclusive (11). A recent unblinded clinical trial of dexamethasone administered early in moderate to severe ARDS suggested improvements in ventilator-free days and mortality, but the trial was stopped early due to slow enrollment, which may magnify the treatment effects (). A recent unblinded clinical trial of dexamethasone administered early in moderate to severe ARDS suggested improvements in ventilator-free days and mortality, but the trial was stopped early due to slow enrollment, which may magnify the treatment effects (12). Thus, the role of corticosteroids in ARDS remains uncertain, and more data are needed.
Treatment references
1. Grasselli G, Calfee CS, Camporota L, et al: ESICM guidelines on acute respiratory distress syndrome: definition, phenotyping and respiratory support strategies. Intensive Care Med 49(7):727–759, 2023. doi:10.1007/s00134-023-07050-7
2. Frat JP, Thille AW, Mercat A, et al: High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med 372:2185–2196, 2015. doi: 10.1056/NEJMoa1503326
3. Patel BK, Wolfe KS, Pohlman AS, et al: Effect of noninvasive ventilation delivered by helmet vs face mask on the rate of endotracheal intubation in patients with acute respiratory distress syndrome: A randomized clinical trial. J AMA 315(22):2435–2441, 2016. doi: 10.1001/jama.2016.6338
4. Grieco DL, Menga LS, Cesarano M, et al: Effect of helmet noninvasive ventilation vs high-flow nasal oxygen on days free of respiratory support in patients With COVID-19 and moderate to severe hypoxemic respiratory failure: The HENIVOT randomized clinical trial. JAMA 325(17):1731–1743, 2021. doi: 10.1001/jama.2021.4682
5. Bellani G, Laffey JG, Pham T, et al: Noninvasive ventilation of patients with acute respiratory distress syndrome. Insights from the LUNG SAFE study. Am J Respir Crit Care Med 195(1):67–77, 2017. doi: 10.1164/rccm.201606-1306OC
Demiselle J, Calzia E, Hartmann C, et al: Target arterial PO2 according to the underlying pathology: a mini-review of the available data in mechanically ventilated patients. Ann Intensive Care 11(1):88, 2021. doi:10.1186/s13613-021-00872-y
6. Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators, Cavalcanti AB, Suzumura ÉA, et al: Effect of lung recruitment and titrated positive end-expiratory pressure (PEEP) vs low PEEP on mortality in patients with acute respiratory distress syndrome: A randomized clinical trial. JAMA 318(14):1335–1345, 2017. doi: 10.1001/jama.2017.14171
7. Guérin C, Reignier J, Richard JC, et al: Prone positioning in severe acute respiratory distress syndrome. N Engl J Med 368(23):2159–2168, 2013. doi: 10.1056/NEJMoa1214103
8. Scholten EL, Beitler JR, Prisk GK, et al: Treatment of ARDS with prone positioning. Chest 151:215–224, 2017. doi: 10.1016/j.chest.2016.06.032. Epub 2016 Jul 8
9. National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network, Wiedemann HP, Wheeler AP, et al: Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 354(24):2564–2575, 2006. doi: 10.1056/NEJMoa062200
10. Qadir N, Chang SY: Pharmacologic Treatments for Acute Respiratory Distress Syndrome. Crit Care Clin 37(4):877–893, 2021. doi:10.1016/j.ccc.2021.05.009
11. Lewis SR, Pritchard MW, Thomas CM, Smith AF: Pharmacological agents for adults with acute respiratory distress syndrome. Cochrane Database Syst Rev 7(7):CD004477, 2019. doi:10.1002/14651858.CD004477.pub3
12. Villar J, Ferrando C, Martinez D, et al: Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respir Med 8: 267–276, 2020. doi: 10.1016/S2213-2600(19)30417-5
Prognosis for AHRF
Prognosis is highly variable and depends on a variety of factors, including
Etiology of respiratory failure
Severity of disease
Age
Chronic health status
Overall, mortality in ARDS was very high (40 to 60%) but has declined in recent years to 25 to 40% (1), probably because of improvements in mechanical ventilation and in treatment of sepsis. However, mortality remains very high (> 40%) for patients with severe ARDS (ie, those with a PaO2:FIO2 < 100 mm Hg).
Most often, death is not caused by respiratory dysfunction but by sepsis and multiorgan failure. Persistence of neutrophils and high cytokine levels in bronchoalveolar lavage fluid predict a poor prognosis. Mortality otherwise increases with age, presence of sepsis, and severity of preexisting organ insufficiency or coexisting organ dysfunction.
Pulmonary function returns to close to normal in 6 to 12 months in most patients who survive ARDS; however, patients with a protracted clinical course or severe disease may have residual pulmonary symptoms, and many have persistent neuromuscular weakness, exercise limitation, and cognitive impairment.
Prognosis reference
1. Bellani G, Laffey JG, Pham T, et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries [published correction appears in JAMA 2016 Jul 19;316(3):350] [published correction appears in JAMA 2016 Jul 19;316(3):350]. JAMA 2016;315(8):788-800. doi:10.1001/jama.2016.0291







