

Diffuse alveolar hemorrhage is persistent or recurrent pulmonary hemorrhage that originates from the lung parenchyma (ie, the alveoli) as opposed to the airways. There are numerous causes, but autoimmune disorders are the most common. Most patients acutely present with dyspnea, cough, hemoptysis, and new alveolar infiltrates on chest imaging. Diagnostic testing is usually directed at the suspected underlying disorder. Imaging studies and serologic tests are frequently obtained. Treatment is with immunosuppressants (eg, glucocorticoids) for patients with autoimmune causes and supportive measures (eg, supplemental oxygen) if needed.
Diffuse alveolar hemorrhage is usually defined as bleeding within the alveolar spaces originating from the pulmonary microvasculature, most commonly the alveolar capillaries. This process results in diffuse involvement of the lung parenchyma, as opposed to localized hemorrhage. Diffuse alveolar hemorrhage is not a specific disorder, but a syndrome that has a specific differential diagnosis and a specific sequence of testing. Some disorders that cause diffuse alveolar hemorrhage are associated with glomerulonephritis; then the disorder is defined as a pulmonary-renal syndrome.
Pathophysiology of Diffuse Alveolar Hemorrhage
Diffuse alveolar hemorrhage results from widespread damage to the small pulmonary vessels, due to disruption of the alveolar-capillary basement membrane, leading to blood collecting within the alveoli. If enough alveoli are affected, gas exchange is disrupted. The specific pathophysiology and manifestations vary depending on cause.
The 3 main pathologic types of diffuse alveolar hemorrhage are: pulmonary capillaritis, bland pulmonary hemorrhage, and diffuse alveolar damage. However, these patterns can overlap (ie, a single underlying disorder may show characteristics of more than one of these histologies) (1).
Pulmonary capillaritis is characterized by neutrophilic infiltration and destruction of the alveolar capillary walls. It most commonly occurs in systemic rheumatic diseases such as ANCA-associated vasculitis and systemic lupus erythematosus. Bland pulmonary hemorrhage refers to intra-alveolar bleeding without significant inflammation or capillaritis, typically associated with coagulopathies, anticoagulant use, or causes of elevated left-sided cardiac pressures (eg, mitral stenosis). Diffuse alveolar damage is the histopathologic pattern that occurs in acute respiratory distress syndrome (ARDS) and can be associated with alveolar hemorrhage, where hemorrhage occurs in the setting of widespread alveolar epithelial and endothelial injury without capillaritis or vasculitis.
Pathophysiology reference
1. Saha BK, Chong WH, Milman NT. Differentiation of idiopathic pulmonary hemosiderosis from rheumatologic and autoimmune diseases causing diffuse alveolar hemorrhage: establishing a diagnostic approach. Clin Rheumatol. 2022;41(2):325-336. doi:10.1007/s10067-021-05895-1
Etiology of Diffuse Alveolar Hemorrhage
Many disorders can cause alveolar hemorrhage; they include:
Autoimmune disorders (eg, systemic vasculitides, anti-glomerular basement membrane (anti-GBM) disease, antiphospholipid syndrome)
Cardiac disorders (eg, mitral stenosis)
Coagulation disorders caused by diseases or anticoagulant medications
Drug-induced (eg, propylthiouracil, amiodarone, methotrexate, nitrofurantoin, montelukast, infliximab, crack Drug-induced (eg, propylthiouracil, amiodarone, methotrexate, nitrofurantoin, montelukast, infliximab, crackcocaine)
Hematopoietic stem cell transplantation or solid organ transplantation
Isolated pauci-immune pulmonary capillaritis
Pulmonary infections (eg, hantavirus infection, other viral infections)
Toxic exposures (eg, trimellitic anhydride, isocyanates, certain pesticides, vaping)
Approximately 50% of patients who meet criteria for acute respiratory distress syndrome also have diffuse alveolar damage upon histopathologic examination (1).
Etiology reference
1. Cardinal-Fernández P, Lorente JA, Ballén-Barragán A, Matute-Bello G. Acute Respiratory Distress Syndrome and Diffuse Alveolar Damage. New Insights on a Complex Relationship. Ann Am Thorac Soc. 2017;14(6):844-850. doi:10.1513/AnnalsATS.201609-728PS
Symptoms and Signs of Diffuse Alveolar Hemorrhage
Symptoms and signs of milder diffuse alveolar hemorrhage are dyspnea, cough, and fever. Hemoptysis is common but may be absent in up to one-third of patients (1). Some patients can have anemia upon presentation, but ongoing bleeding will lead to a further reduction in the hematocrit. Many patients present with acute respiratory failure, sometimes leading to death.
Pearls & Pitfalls
|
Physical examination findings may include tachypnea, hypoxemia, and crackles on auscultation.
Other manifestations depend on the underlying disorder (eg, diastolic murmur in patients with mitral stenosis, purpura in patients with ANCA-associated vasculitis).
Symptoms and signs reference
1. Nasser M, Cottin V. Alveolar Hemorrhage in Vasculitis (Primary and Secondary). Semin Respir Crit Care Med. 2018;39(4):482-493. doi:10.1055/s-0038-1668533
Diagnosis of Diffuse Alveolar Hemorrhage
Chest imaging
Bronchoalveolar lavage
Serologic and other tests to diagnose the underlying disorder
Sometimes lung biopsy
The diagnosis is suggested by clinical findings of dyspnea, cough, and hemoptysis accompanied by chest imaging (eg, radiographs, CT scan) findings of patchy or diffuse, bilateral alveolar infiltrates and a suspicion of diffuse alveolar hemorrhage. Typical findings on chest CT imaging include diffuse, bilateral ground glass opacities that tend to be more centrally located than peripheral, often with subpleural sparing.
Bronchoscopy with bronchoalveolar lavage (BAL) is strongly recommended to support the diagnosis, particularly when manifestations are atypical or an airway source of hemorrhage has not been excluded. Specimens show blood with numerous erythrocytes and siderophages and hemosiderin-laden macrophages; lavage fluid typically becomes increasingly hemorrhagic after sequential sampling.


This chest radiograph shows bilateral alveolar opacities in a patient with alveolar hemorrhage.
By permission of the publisher. From Cohen A, Glassock R. In Atlas of Diseases of the Kidney: Glomerulonephritis and Vasculitis. Edited by R Schrier (series editor), RJ Glassock, and AH Cohen. Philadelphia, Current Medicine, 1999.

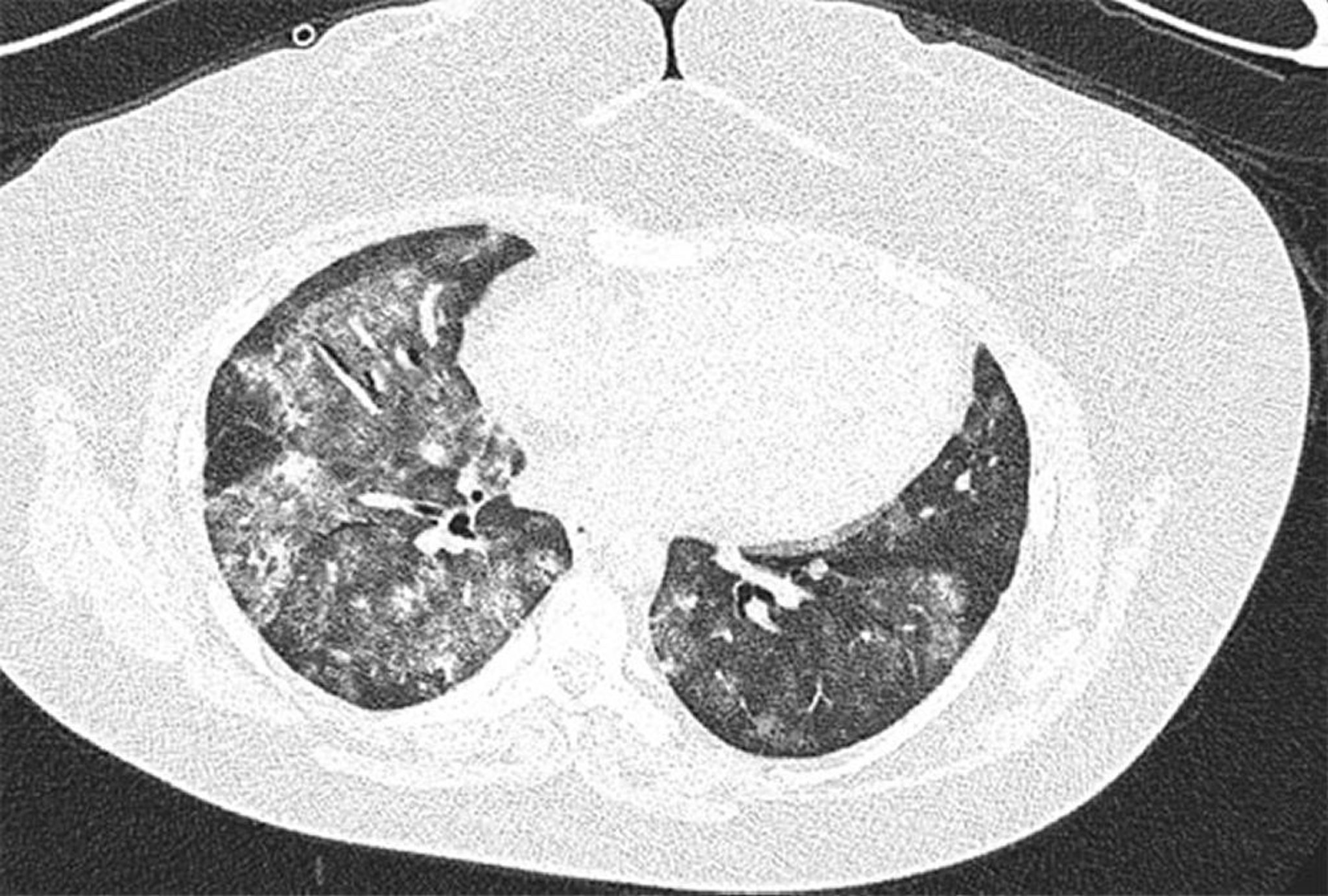
High- resolution CT image of 28-year-old female with antiphospholipid syndrome with recurrent diffuse alveolar hemorrhage. Image shows bilateral and patchy alveolar ground glass opacities with subpleural sparing. Bronchoalveolar lavage confirmed alveolar hemorrhage.
Image courtesy of Joyce Lee, MD.
Evaluation of the cause
Further testing for the cause should be done. Urinalysis is indicated to exclude glomerulonephritis and the pulmonary-renal syndrome; serum blood urea nitrogen (BUN) and creatinine also should be measured. Testing for infectious causes with microbiologic studies of BAL fluid, blood cultures, or other serologic studies for specific pathogens (eg, for Aspergillus) should be considered, particularly in immunocompromised patients.
Other routine tests include:
Complete blood count (CBC)
Coagulation studies
Platelet count
Serologic tests
Serologic tests, including antinuclear antibodies (ANA), anti–double-stranded DNA [anti-dsDNA], antiglomerular basement membrane [anti-GBM] antibodies, antineutrophil cytoplasmic antibodies [ANCA], antiphospholipid antibody, and complement levels (C3, C4), are performed to evaluate for underlying disorders. Perinuclear-ANCA (p-ANCA) titers are elevated in some cases of isolated pauci-immune pulmonary capillaritis.
Other tests depend on clinical context. When patients are stable, pulmonary function tests may be done to document lung function. They may show increased diffusing capacity for carbon monoxide (DLCO) due to increased uptake of carbon monoxide by intra-alveolar hemoglobin; however, this finding, which is consistent with hemorrhage, does not assist with establishing a specific diagnosis.
Echocardiography may be indicated to exclude mitral stenosis.
Lung biopsy with immunohistochemistry or kidney biopsy (if urinalysis is abnormal) may be needed when a cause remains unclear or the progression of disease is too rapid to await the results of serologic testing. Findings on histopathologic examination of biopsied tissues can help identify the cause of diffuse alveolar hemorrhage. For example, in anti-GBM disease, linear IgG deposition is seen along the pulmonary capillary basement membranes. In contrast, in cases of systemic autoimmune conditions leading to diffuse alveolar hemorrhage, granular immune complex deposition can be observed along the pulmonary capillary basement membrane. When diffuse alveolar hemorrhage is due to a vasculitis like granulomatosis with polyangiitis (GPA) or microscopic polyangiitis (MPA), neutrophilic infiltration of the capillary wall is seen.
Treatment of Diffuse Alveolar Hemorrhage
Immunosuppressants (eg, glucocorticoids, rituximab, cyclophosphamide,avacopan)Immunosuppressants (eg, glucocorticoids, rituximab, cyclophosphamide,avacopan)
Sometimes plasma exchange (eg, for anti-glomerular basement membrane [anti-GBM] disease)
Supportive measures (eg, supplemental oxygen therapy, mechanical ventilation)
Treatment involves correcting the cause. Treatment recommendations are based on the type and severity of disease (1).
Immunosuppressants are used in many patients with diffuse alveolar hemorrhage, particularly when due to pulmonary capillaritis (eg, ANCA-associated vasculitis). High-dose glucocorticoids are most commonly used, often in combination with a disease-specific adjunctive therapy. For example, cyclophosphamide or rituximab may be added to glucocorticoids to treat diffuse alveolar hemorrhage due to Immunosuppressants are used in many patients with diffuse alveolar hemorrhage, particularly when due to pulmonary capillaritis (eg, ANCA-associated vasculitis). High-dose glucocorticoids are most commonly used, often in combination with a disease-specific adjunctive therapy. For example, cyclophosphamide or rituximab may be added to glucocorticoids to treat diffuse alveolar hemorrhage due toANCA-associated vasculitis or systemic lupus erythematosus. Rituximab may also be used to treat alveolar hemorrhage due to anti-GBM disease and antiphospholipid syndrome. For patients with ANCA-associated vasculitis, the addition of avacopan, a complement C5a receptor antagonist, can also be considered to help reduce glucocorticoid exposure.. For patients with ANCA-associated vasculitis, the addition of avacopan, a complement C5a receptor antagonist, can also be considered to help reduce glucocorticoid exposure.
Plasma exchange is also used to treat anti-GBM disease.
Several studies have reported successful use of recombinant activated human factor VII in treating severe unresponsive alveolar hemorrhage (2), but such therapy is controversial because of possible thrombotic complications.
Supportive management measures include supplemental oxygen, bronchodilators, reversal of any coagulopathy, and intubation with protective strategies as for acute respiratory distress syndrome (ARDS) and mechanical ventilation.
Treatment references
1. Chung SA, Langford CA, Maz M, et al. 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Arthritis Rheumatol. 2021;73(8):1366–1383. doi:10.1002/art.41773
2. Pathak V, Kuhn J, Gabriel D, Barrow J, Jennette JC, Henke DC. Use of Activated Factor VII in Patients with Diffuse Alveolar Hemorrhage: A 10 Years Institutional Experience. Lung. 2015;193(3):375-379. doi:10.1007/s00408-015-9720-z
Prognosis for Diffuse Alveolar Hemorrhage
The prognosis of diffuse alveolar hemorrhage depends on the underlying cause and severity of organ involvement. Immune-mediated causes of diffuse alveolar hemorrhage are usually associated with a better long-term prognosis (1). For example, one retrospective observational study over a 12-year period found that, while the overall mortality of diffuse alveolar hemorrhage was high (37.5%), patients with immune-mediated etiologies had a lower mortality compared to those with non-immune causes (15.1% vs 50.9%) (1).
Recurrent alveolar hemorrhage can cause pulmonary hemosiderosis and fibrosis, both of which develop when ferritin aggregates within alveoli and exerts toxic effects. Emphysema can occur in some patients with recurrent diffuse alveolar hemorrhage secondary to microscopic polyangiitis or granulomatosis with polyangiitis.
Prognosis reference
1. Bhushan A, Choi D, Maresh G, Deodhar A. Risk factors and outcomes of immune and non-immune causes of diffuse alveolar hemorrhage: a tertiary-care academic single-center experience. Rheumatol Int. 2022;42(3):485-492. doi:10.1007/s00296-021-04842-2
Key Points
Although diffuse alveolar hemorrhage can have various causes (eg, infection, toxins, drugs, hematologic or cardiac disorders), autoimmune disorders are the most common causes.
Symptoms, signs, and chest-imaging findings are not specific.
Confirm diffuse alveolar hemorrhage by doing bronchoalveolar lavage to show persistent hemorrhage with sequential lavage samples.
Testing is obtained to determine the underlying disorder, including routine laboratory markers, serologic testing, and sometimes other studies.
Treat the cause (eg, with glucocorticoids, cyclophosphamide, rituximab, avacopan, plasma exchange).Treat the cause (eg, with glucocorticoids, cyclophosphamide, rituximab, avacopan, plasma exchange).
Drug Information for the Topic





