



Topic Resources
(See also Overview of Tubulointerstitial Diseases.)
Several metabolic disturbances can cause tubulointerstitial nephritis.
Acute urate nephropathy
This disorder is not a true form of acute tubulointerstitial nephritis but rather an intraluminal obstructive uropathy caused by uric acid crystal deposition within the lumen of renal tubules; acute oliguric or anuric kidney injury results.
The most common cause of acute urate nephropathy is
Tumor lysis syndrome after treatment of lymphoma, leukemia, or other myeloproliferative disorders
Other causes of acute urate nephropathy include seizures, treatment of solid tumors, rare primary disorders of urate overproduction (hypoxanthine-guanine phosphoribosyltransferase deficiency), and disorders of urate overexcretion due to decreased proximal tubule reabsorption (Fanconi-like syndromes).
Disorders of urate overproduction and overexcretion are rare.
Typically, no symptoms are present.
Diagnosis is suspected when acute kidney injury occurs in patients with marked hyperuricemia (> 15 mg/dL). Urinalysis results may be normal or may show urate crystals.
Prognosis for complete recovery of renal function is excellent if treatment is initiated rapidly.
In patients with normal cardiac and renal function, treatment is usually with allopurinol plus aggressive IV hydration with normal saline. Allopurinol is given to help prevent urate nephropathy. In the event that acute urate nephropathy does occur, urate oxidase (rasburicase), which catalyzes urate to a much more soluble compound, is usually given. In patients with normal cardiac and renal function, treatment is usually with allopurinol plus aggressive IV hydration with normal saline. Allopurinol is given to help prevent urate nephropathy. In the event that acute urate nephropathy does occur, urate oxidase (rasburicase), which catalyzes urate to a much more soluble compound, is usually given.
Patients should be carefully monitored for adverse effects, including anaphylaxis and hemolysis. Hemodialysis may be recommended to remove excess circulating urate in severe cases where diuresis cannot be induced with a loop diuretic and IV saline. Alkalinization with a sodium bicarbonate infusion is no longer recommended because even though it increases solubility of urate, it risks tubular precipitation of calcium phosphate salts.may be recommended to remove excess circulating urate in severe cases where diuresis cannot be induced with a loop diuretic and IV saline. Alkalinization with a sodium bicarbonate infusion is no longer recommended because even though it increases solubility of urate, it risks tubular precipitation of calcium phosphate salts.
Prevention of acute urate nephropathy is indicated for patients at high risk (eg, those at risk of tumor lysis syndrome). Prevention is by use of allopurinol 2 to 3 times a day plus saline loading to maintain a urine output Prevention of acute urate nephropathy is indicated for patients at high risk (eg, those at risk of tumor lysis syndrome). Prevention is by use of allopurinol 2 to 3 times a day plus saline loading to maintain a urine output> 2.5 L/day before chemotherapy or radiation therapy. Urate oxidase is also indicated for the prevention of acute urate nephropathy secondary to tumor lysis syndrome in high-risk patients.
Chronic urate nephropathy
This condition is chronic tubulointerstitial nephritis caused by deposition of sodium urate crystals in the medullary interstitium in patients with chronic hyperuricemia. Sequelae are chronic inflammation and fibrosis, with ensuing chronic renal insufficiency and renal failure. Chronic urate nephropathy was once common in patients with tophaceous gout but is now rare because gout is more often effectively treated.
Suggestive but nonspecific findings include a bland urine sediment and hyperuricemia disproportionate to the degree of renal insufficiency:
Urate > 9 mg/dL (535.4 micromole/L) with serum creatinine < 1.5 mg/dL (132.6 micromole/L)
Urate > 10 mg/dL (594.9 micromole/L) with serum creatinine 1.5 to 2 mg/dL (132.6 micromole/L to 176.8 micromole/L)
Urate > 12 mg/dL (713.8 micromole/L) with serum creatinine> 2 mg/dL (176.8 micromole/L)
Many causes of tubulointerstitial diseases may have these findings, lead nephropathy being the most common.
Treatment of chronic urate nephropathy is that of hyperuricosuria.

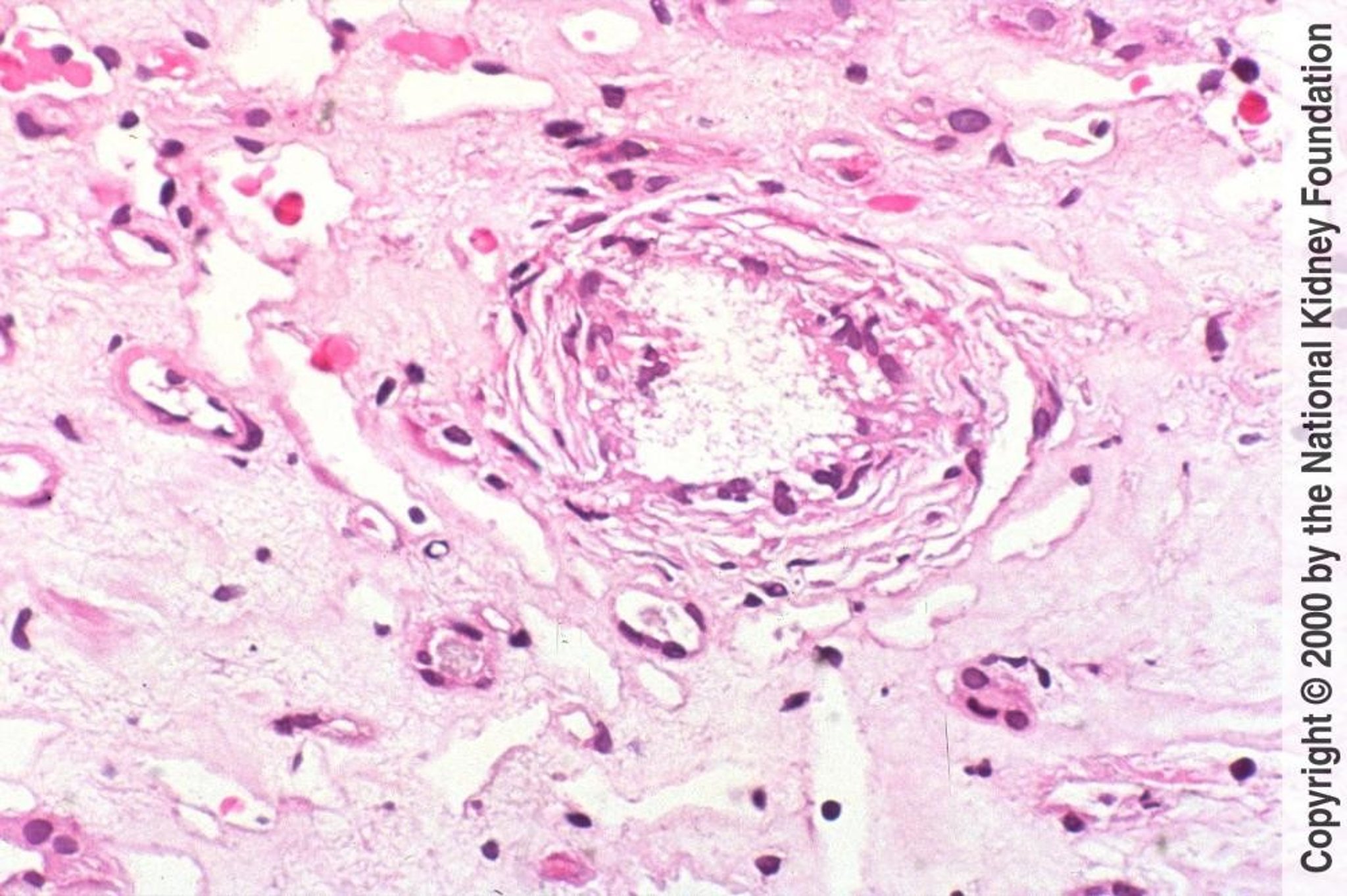
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Hyperoxaluria
Hyperoxaluria is a common cause of nephrolithiasis but an uncommon cause of acute and chronic tubulointerstitial nephritis. Causes and prevention of hyperoxaluria are discussed elsewhere.
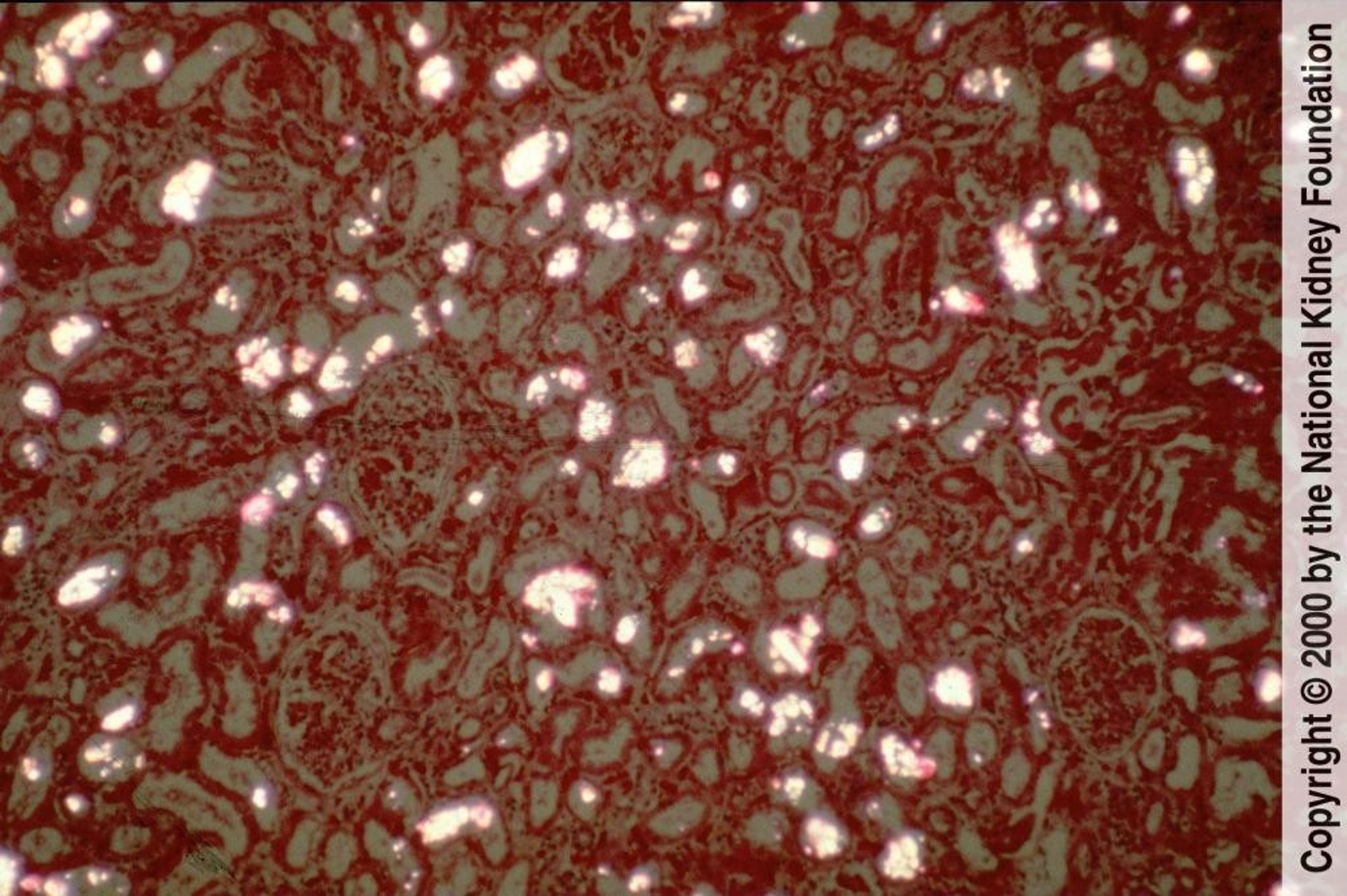
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Hypercalcemia
Hypercalcemia causes nephropathy by 2 mechanisms.
Severe (> 12 mg/dL) temporary hypercalcemia may cause reversible renal insufficiency by renal vasoconstriction and natriuresis-induced volume depletion.
Long-standing hypercalcemia and hypercalciuria lead to chronic tubulointerstitial nephritis with calcification and necrosis of tubular cells, interstitial fibrosis, and calcification (nephrocalcinosis). Common associated findings include
Arginine vasopressin resistance (previously called nephrogenic diabetes insipidus)
Diagnosis is based on presence of hypercalcemia and unexplained renal insufficiency; nephrocalcinosis can be detected by ultrasonography or noncontrast CT.
Treatment is management of hypercalcemia.
Chronic hypokalemia
Chronic hypokalemia of a moderate to severe degree may cause nephropathy with impaired urinary concentration and vacuolation of proximal tubular cells and occasionally of distal tubular cells. Diagnosis is suggested by history of prolonged severe hypokalemia. Renal biopsy is not usually required in the diagnostic evaluation of these patients; however, chronic interstitial inflammatory changes, fibrosis, and renal cysts have been found in renal biopsies of patients with hypokalemia of ≥ 1 month.
Treatment consists of correction of the underlying disorder and oral potassium supplements. Although the hypokalemia as well as the number and size of the cysts are reversible, the chronic tubulointerstitial nephropathy and renal insufficiency may be irreversible.
Drugs Mentioned In This Article






