



(See also Overview of Allergic and Atopic Disorders and Hereditary and Acquired C1 Inhibitor Deficiency.)
Angioedema is swelling (usually localized) of the subcutaneous tissues due to increased vascular permeability and extravasation of intravascular fluid. Known mediators of increased vascular permeability include the following:
Mast cell–derived mediators (eg, histamine, leukotrienes, prostaglandins)
Bradykinin and complement-derived mediators
Mast cell–derived mediators tend to also affect layers superficial to subcutaneous tissue, including the dermal-epidermal junction. There, these mediators cause urticaria and pruritus, which thus usually accompany mast cell–mediated angioedema.
In bradykinin-mediated angioedema, the dermis is usually spared, so urticaria and pruritus are absent.
In some cases, the mechanism and cause of angioedema are unknown. Several causes (eg, calcium channel blockers, fibrinolytic agents) have no identified mechanism; sometimes a cause (eg, muscle relaxants) with a known mechanism is overlooked clinically.
Angioedema is usually acute or but can be chronic (> 6 weeks).
There are hereditary and acquired forms characterized by an abnormal complement response.
Acute angioedema
Acute angioedema is mast cell–mediated in > 90% of cases. Mast cell–mediated mechanisms include acute allergic, typically IgE-mediated reactions. IgE-mediated angioedema is usually accompanied by acute urticaria (local wheals and erythema in the skin) and itching. It may often be caused by the same allergens (eg, medication, venom, dietary, extracted allergens) that are responsible for acute IgE-mediated urticaria.
Acute angioedema can also result from agents that directly stimulate mast cells without involving IgE. Causes can include opioids, radiopaque contrast agents, aspirin, and nonsteroidal anti-inflammatory drugs (NSAIDs).Acute angioedema can also result from agents that directly stimulate mast cells without involving IgE. Causes can include opioids, radiopaque contrast agents, aspirin, and nonsteroidal anti-inflammatory drugs (NSAIDs).
Angiotensin-converting enzyme (ACE) inhibitors cause about 30% of cases of acute angioedema seen in emergency departments (1, 2). ACE inhibitors can directly increase levels of bradykinin. The face and upper airways are most commonly affected. The intestine may also be affected, often presenting with intermittent abdominal pain and bloating. Urticaria does not occur. Angioedema may occur soon or years after therapy begins.
Chronic angioedema
The cause of chronic (> 6 weeks) angioedema is usually unknown. IgE-mediated mechanisms are rare, but chronic ingestion of an unsuspected medication or chemical (eg, penicillin in milk, a nonprescription medication, preservatives, other food additives) is sometimes the cause. A few cases are due to hereditary or acquired C1 inhibitor deficiency.
Idiopathic angioedema is angioedema that occurs without urticaria, is chronic and recurrent, and has no identifiable cause.
Hereditary and acquired angioedema
Hereditary angioedema and acquired angioedema are disorders that are characterized by abnormal complement responses and caused by deficiency or dysfunction of C1 inhibitor. Symptoms are those of bradykinin-mediated angioedema.
References
1. Agah R, Bandi V, Guntupalli KK. Angioedema: the role of ACE inhibitors and factors associated with poor clinical outcome. Intensive Care Med 1997;23(7):793-796. doi:10.1007/s001340050413
2. Gandhi J, Jones R, Teubner D, Gabb G. Multicentre audit of ACE-inhibitor associated angioedema (MAAAA). Aust Fam Physician 2015;44(8):579-583.
Symptoms and Signs of Angioedema
In angioedema, edema is often asymmetric and mildly painful. It often involves the face, lips, and/or tongue and may also occur on the back of hands or feet, on the genitals, or in the abdomen. Edema of the upper airways may cause respiratory distress and stridor; the stridor may be mistaken for asthma. The airways may be completely obstructed. Edema of the intestine may cause nausea, vomiting, colicky abdominal pain, and/or diarrhea.

This photo shows acute swelling of the lips in a patient with hereditary C1 inhibitor deficiency.
By permission of the publisher. From Joe E, Soter N. In Current Dermatologic Diagnosis and Treatment, edited by I Freedberg, IM Freedberg, and MR Sanchez. Philadelphia, Current Medicine, 2001.


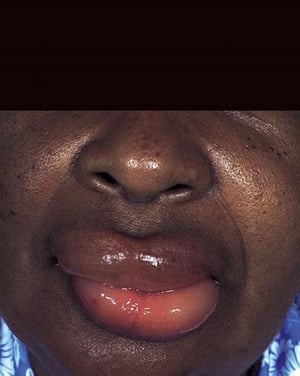
Angioedema of the lips can be asymmetric, as shown in this photo.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY


This patient has a swollen tongue due to angioedema.
SCIENCE PHOTO LIBRARY
This photo shows acute swelling of the lips in a patient with hereditary C1 inhibitor deficiency.
By permission of the publisher. From Joe E, Soter N. In Current Dermatologic Diagnosis and Treatment, edited by I Freedberg, IM Freedberg, and MR Sanchez. Philadelphia, Current Medicine, 2001.
Angioedema of the lips can be asymmetric, as shown in this photo.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
This patient has a swollen tongue due to angioedema.
SCIENCE PHOTO LIBRARY
Other manifestations of angioedema depend on the mediator.
Mast cell–mediated angioedema
Tends to develop over minutes to several hours
May be accompanied by other manifestations of acute allergic reactions (eg, pruritus, urticaria, flushing, bronchospasm, anaphylactic shock)
Bradykinin-mediated angioedema
Tends to develop over hours to a few days
Is not accompanied by other manifestations of allergic reactions
Diagnosis of Angioedema
History and physical examination
For diagnosis of urticaria, see Urticaria: Evaluation.
Patients with localized swelling but no urticaria are asked specifically about use of ACE inhibitors.
The cause of angioedema is often obvious, and diagnostic tests are seldom required because most reactions are self-limited and do not recur. When angioedema is acute, no test is particularly useful. When it is chronic, thorough medication and dietary evaluation is warranted.
If no cause is obvious or if family members have urticaria, clinicians should consider measuring C1 inhibitor levels to check for C1 inhibitor deficiency and C4 levels to check for hereditary or acquired angioedema. Low levels of C4, even between episodes, may help confirm a diagnosis of hereditary angioedema (types 1 and 2) or acquired C1 inhibitor deficiency.
Erythropoietic protoporphyria may mimic allergic forms of angioedema; both can cause edema and erythema after exposure to sunlight. The two can be distinguished by measuring blood and fecal porphyrins.
Pearls & Pitfalls
|
Treatment of Angioedema
Airway management
For mast cell–mediated angioedema, an antihistamine and sometimes a systemic corticosteroid and epinephrineFor mast cell–mediated angioedema, an antihistamine and sometimes a systemic corticosteroid and epinephrine
For ACE inhibitor–related angioedema, occasionally fresh frozen plasma and C1 inhibitor concentrateFor ACE inhibitor–related angioedema, occasionally fresh frozen plasma and C1 inhibitor concentrate
For recurrent idiopathic angioedema, an oral antihistamine
Securing an airway is the highest priority. If angioedema involves the airways, epinephrine is given subcutaneously or IM as for anaphylaxis unless the mechanism is obviously bradykinin-mediated (eg, due to use of an ACE inhibitor or to known hereditary or acquired angioedema). In mast cell–mediated angioedema, treatment usually rapidly reduces airway edema; however, in bradykinin-mediated angioedema, edema usually takes > 30 minutes to decrease after treatment begins. Thus, endotracheal intubation is more likely to be needed in bradykinin-mediated angioedema.
Treatment of angioedema also includes removing or avoiding the allergen and using medications that relieve symptoms. If a cause is not obvious, all nonessential medications should be stopped.
For mast cell–mediated angioedema, medications that may relieve symptoms include H1 blockers. Prednisone 30 to 40 mg orally once a day is indicated for more severe reactions. Topical corticosteroids are useless. If symptoms are severe, a corticosteroid and antihistamine can be given IV (eg, methylprednisolone 125 mg and diphenhydramine 50 mg). Long-term treatment may involve H1 and H2 blockers and occasionally corticosteroids.. Prednisone 30 to 40 mg orally once a day is indicated for more severe reactions. Topical corticosteroids are useless. If symptoms are severe, a corticosteroid and antihistamine can be given IV (eg, methylprednisolone 125 mg and diphenhydramine 50 mg). Long-term treatment may involve H1 and H2 blockers and occasionally corticosteroids.
Patients who have severe mast cell–mediated reactions should be advised to always carry a prefilled, self-injecting syringe of epinephrine and oral antihistamines and, if a severe reaction occurs, to use these treatments as quickly as possible and then go to the emergency department. There, they can be closely monitored and treatment can be repeated or adjusted as needed.Patients who have severe mast cell–mediated reactions should be advised to always carry a prefilled, self-injecting syringe of epinephrine and oral antihistamines and, if a severe reaction occurs, to use these treatments as quickly as possible and then go to the emergency department. There, they can be closely monitored and treatment can be repeated or adjusted as needed.
For bradykinin-mediated angioedema, epinephrine, corticosteroids, and antihistamines have not been shown to be effective. Angioedema due to ACE inhibitor use usually resolves about 24 to 48 hours after stopping the medication. If symptoms are severe, progressing, or refractory, epinephrine, corticosteroids, and antihistamines have not been shown to be effective. Angioedema due to ACE inhibitor use usually resolves about 24 to 48 hours after stopping the medication. If symptoms are severe, progressing, or refractory,treatments used for hereditary or acquired angioedema can be tried. They include fresh frozen plasma, C1 inhibitor concentrate, and possibly ecallantide (which inhibits plasma kallikrein, required for the generation of bradykinin) and icatibant (which blocks bradykinin). can be tried. They include fresh frozen plasma, C1 inhibitor concentrate, and possibly ecallantide (which inhibits plasma kallikrein, required for the generation of bradykinin) and icatibant (which blocks bradykinin).
For idiopathic angioedema, a high dose of a nonsedating oral antihistamine can be tried.
Key Points
In the emergency department, about 30% of cases of acute angioedema are caused by angiotensin-converting enzyme (ACE) inhibitors (bradykinin-mediated), although overall, > 90% of cases are mast cell–mediated.
For acute angioedema, first make sure the airway is secure; if the airway is affected, give epinephrine subcutaneously or IM unless the cause is obviously bradykinin-mediated angioedema, which is more likely to require endotracheal intubation.For acute angioedema, first make sure the airway is secure; if the airway is affected, give epinephrine subcutaneously or IM unless the cause is obviously bradykinin-mediated angioedema, which is more likely to require endotracheal intubation.
The cause of chronic angioedema is usually unknown.
Swelling always develops; bradykinin-mediated angioedema tends to develop more slowly and to cause fewer symptoms of an acute allergic reaction (eg, pruritus, urticaria, anaphylactic shock) than does mast cell–mediated angioedema.
For chronic angioedema, take a thorough drug and dietary history, and consider testing for C1 inhibitor deficiency and measuring C4 levels; testing is rarely necessary for recurrent acute episodes if initial screening was done.
Eliminating or avoiding the allergen is key.
For symptomatic and adjunctive treatment, an antihistamine (eg, H1 blocker) and a systemic corticosteroid can relieve symptoms of mast cell–mediated angioedema; frozen plasma, C1 inhibitor concentrate, and/or ecallantide or icatibant may be tried if bradykinin-mediated angioedema is severe or refractory.For symptomatic and adjunctive treatment, an antihistamine (eg, H1 blocker) and a systemic corticosteroid can relieve symptoms of mast cell–mediated angioedema; frozen plasma, C1 inhibitor concentrate, and/or ecallantide or icatibant may be tried if bradykinin-mediated angioedema is severe or refractory.
Drugs Mentioned In This Article






