



Cystoisosporiasis is infection with the protozoan Cystoisospora belli (previously known as Isospora belli). Symptoms include watery diarrhea with gastrointestinal and systemic symptoms. Diagnosis is by detection of characteristic oocysts in stool or intestinal biopsy specimens. Treatment is usually with trimethoprim/sulfamethoxazole (TMP/SMX).
Topic Resources

(See also Overview of Intestinal Protozoan and Microsporidia Infections.)
Cystoisosporiasis is caused by obligate intracellular protozoa that infect intestinal epithelial cells. Transmission is by the fecal-oral route via food or water contaminated with feces from an infected person. Cystoisosporiasis occurs worldwide and is most common in tropical and subtropical climates. Residents of and travelers to endemic areas are at risk.

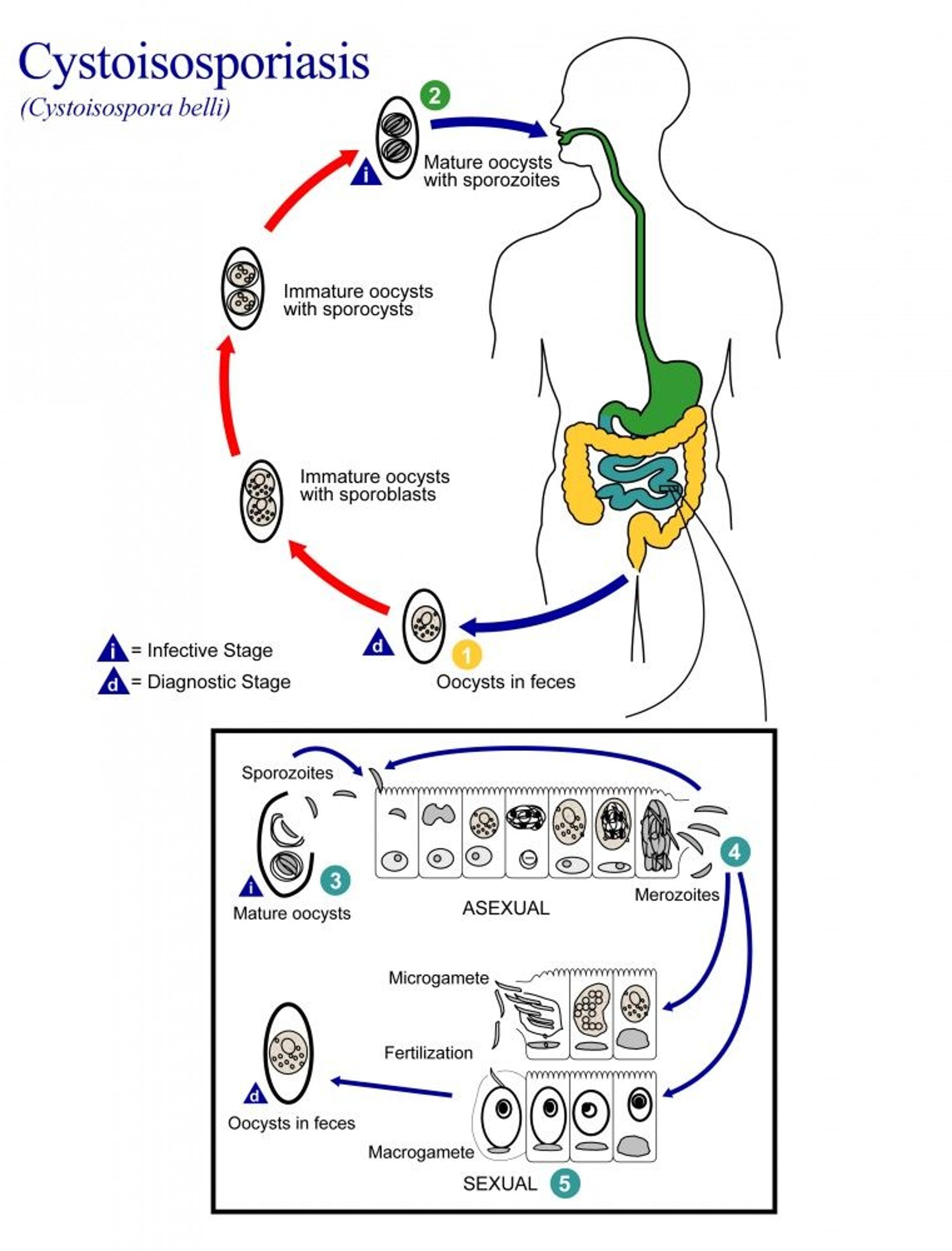
Image from the Centers for Disease Control and Prevention Image Library.
The life cycle of C. belli is similar to that of Cryptosporidium, except that oocysts passed in stool are not sporulated. Thus, when freshly passed in stools, the oocysts are not infective, and direct fecal-oral transmission cannot occur. The oocysts require days to weeks in the environment to sporulate and, therefore, direct person-to-person transmission is unlikely. The sporulated oocysts are ingested in contaminated food or water and excyst in the gastrointestinal tract, releasing sporozoites. The sporozoites invade the epithelial cells of the small intestine, replicate, and mature into oocysts, which are shed in stool.
Symptoms and Signs of Cystoisosporiasis
The primary symptom of cystoisosporiasis is sudden, nonbloody, watery diarrhea, with fever, abdominal cramps, nausea, anorexia, and malaise. In immunocompetent patients, the illness usually resolves spontaneously but can last weeks.
In hosts with depressed cell-mediated immunity as occurs in end-stage HIV, cystoisosporiasis may cause a prolonged illness with severe, intractable, voluminous diarrhea, and weight loss resembling that of cryptosporidiosis.
Diagnosis of Cystoisosporiasis
Microscopic examination of stool
Diagnosis of cystoisosporiasis is by detection of oocysts via microscopic examination of the stool. A modified Ziehl-Neelsen or Kinyoun acid-fast staining technique can help identify Cystoisospora oocysts. Oocysts of Cystoisospora are autofluorescent. Cystoisospora oocysts are larger than Cyclospora and Cryptosporidium oocysts, are ellipsoidal, and may contain one or two sporoblasts.
Multiple (≥ 3) stool specimens may be needed because cyst secretion may be intermittent.
Diagnosis is sometimes made only when intracellular parasite stages are detected in biopsies of intestinal tissue.
In cystoisosporiasis, the stool may contain Charcot-Leyden crystals (hexagonal, double-pointed, and often needlelike crystals) derived from eosinophils.
Cystoisosporiasis may result in peripheral blood eosinophilia.
Treatment of Cystoisosporiasis
Trimethoprim/sulfamethoxazole (TMP/SMX)
Treatment of choice for cystoisosporiasis is double-strength TMP/SMX for 7 to 10 days (see Centers for Disease Control and Prevention: Treatment for Cyclosporiasis).
In patients with end-stage HIV, higher doses and longer duration may be needed, and treatment of acute infection is usually followed by long-term suppressive therapy (one double-strength 160 mg/800 mg TMP/SMX tablet 3 times weekly) to prevent relapse. Institution or optimization of antiretroviral therapy (ART) is important.
For cystoisosporiasis, patients who are allergic to (or intolerant of) TMP/SMX can be treated with pyrimethamine for 3 to 4 weeks. To help prevent bone marrow suppression, patients treated with pyrimethamine are given leucovorin, also known as folinic acid. The daily dose for adults is 10 to 25 mg orally.For cystoisosporiasis, patients who are allergic to (or intolerant of) TMP/SMX can be treated with pyrimethamine for 3 to 4 weeks. To help prevent bone marrow suppression, patients treated with pyrimethamine are given leucovorin, also known as folinic acid. The daily dose for adults is 10 to 25 mg orally.
Ciprofloxacin for 7 to 10 days has been used to treat cystoisosporiasis, but it is less effective than TMP/SMX.Ciprofloxacin for 7 to 10 days has been used to treat cystoisosporiasis, but it is less effective than TMP/SMX.
Prevention of Cystoisosporiasis
Prevention is by hand washing and food and water precautions.
In endemic regions, drinking water should be boiled or chlorinated, unpeeled fruit should be avoided, and vegetables cooked thoroughly. Detailed recommendations for international travelers are available in the Centers for Disease Control and Prevention (CDC) Yellow Book: Food & Water Precautions.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.







