



- Overview of Fractures
- Pediatric Physeal (Growth Plate) Fractures
- Clavicle Fractures
- Proximal Humeral Fractures
- Distal Humeral Fractures
- Radial Head Fractures
- Ulnar and Radial Shaft Fractures
- Distal Radius Fractures
- Isolated Olecranon Fractures
- Scaphoid (Navicular) Fractures
- Metacarpal Neck Fractures
- Fingertip Fractures
- Vertebral Compression Fractures
- Pelvic Fractures
- Hip Fractures
- Femoral Shaft Fractures
- Ankle Fractures
- Calcaneal Fractures
- Fracture-Dislocation of the Midfoot (Lisfranc Injury)
- Fractures of the 5th Metatarsal Bone
- Toe Fractures
- Compartment Syndrome
Most bone fractures result from a single, significant force applied to normal bone.
Topic Resources





")
")

















In addition to fractures, musculoskeletal injuries include
Joint dislocations and subluxations (partial joint dislocations)
Musculoskeletal injuries are common and vary greatly in mechanism, severity, and treatment. The extremities, spine, and pelvis can all be affected.
Musculoskeletal injuries may occur in isolation or as part of multisystem trauma (see Approach to the Trauma Patient). Most musculoskeletal injuries result from blunt trauma, but penetrating trauma can also damage musculoskeletal structures.

Pathophysiology of Fractures
Fractures may be either
Open: The overlying skin is disrupted, and the broken bone is in communication with the environment via a skin wound.
Closed: The overlying skin is intact.
Pathologic fractures occur when mild or minimal force causes a fracture of an area of bone weakened by a disorder (eg, osteoporosis, cancer, infection, bone cyst). When the disorder is osteoporosis, these fractures are often called insufficiency or fragility fractures.
Stress fractures result from repetitive application of moderate force, as may occur in long-distance runners or in soldiers marching while carrying a heavy load. Normally, bone damaged by microtrauma from moderate force self-repairs during periods of rest, but repeated application of force to the same location predisposes to further injury and causes the microtrauma to propagate.
Healing
The rate at which a fracture heals varies depending on the patient's age and coexisting disorders. For example, children heal much faster than adults; disorders that impair peripheral circulation (eg, diabetes, peripheral vascular disease) slow healing.
Fractures heal in 3 overlapping stages:
Inflammatory
Reparative
Remodeling
The inflammatory stage occurs first. A hematoma forms at the fracture site, and a small amount of bone in the distal fracture fragments is resorbed. If a fracture line is not initially visible on radiograph (eg, in some nondisplaced fractures), it typically can be detected about 1 week after the injury as this small amount of bone is resorbed.
During the reparative stage, a callus is formed. New blood vessels develop, enabling cartilage to form across the fracture line. Immobilization (eg, casting) is needed during the first 2 stages to allow new blood vessels to grow. The reparative phase ends with clinical union of the fracture (ie, when there is no pain at fracture site, the injured extremity can be used without pain, and clinical examination detects no bone movement).
In the remodeling stage, the callus, which was originally cartilaginous, becomes ossified, and the bone is broken down and rebuilt (remodeled). During this stage, patients should be instructed to gradually resume moving the injured part normally, including putting load-bearing stress on it.
Complications
Serious complications of fractures are unusual but may affect limb viability or cause permanent limb dysfunction. Risk of complications is high with open fractures (which predispose to infection) and with fractures that disrupt blood vessels, tissue perfusion, and/or nerves. Closed fractures that do not involve blood vessels or nerves, particularly those that are quickly reduced, are least likely to result in serious complications.
Acute complications (associated injuries) include the following:
Bleeding: Bleeding accompanies all fractures (and soft-tissue injuries). Rarely, internal or external bleeding is severe enough to cause hemorrhagic shock (eg, in pelvic, femoral, and some open fractures).
Vascular injuries: Some open fractures disrupt blood vessels. Posteriorly displaced supracondylar humeral fractures may disrupt the vascular supply sufficiently to cause distal limb ischemia; this vascular disruption may be clinically occult for hours after the injury.
Nerve injuries: Nerves may be injured when stretched by displaced pieces of a fractured bone, bruised by a blunt blow, crushed in a severe crush injury, or torn by sharp bone fragments. When nerves are bruised (called neurapraxia), nerve conduction is blocked, but the nerve is physically injured. Neurapraxia causes temporary motor and/or sensory deficits; neurologic function returns completely in about 6 to 8 weeks. When nerves are crushed (called axonotmesis), the axon is injured, but the myelin sheath is not. This injury is more severe than neurapraxia. Depending on the extent of the damage, the nerve can regenerate over weeks to years. Usually, nerves are torn (called neurotmesis) in open fractures. Torn nerves do not heal spontaneously and may have to be repaired surgically.
Pulmonary embolism: In patients with a hip or pelvic fracture, risk of pulmonary embolism is high due to vascular injury and immobilization. Pulmonary embolism is the most common fatal complication of serious fractures of the hip or pelvis.
Fat embolism: Fractures of long bones (most commonly, femoral fractures) may release fat (and other marrow contents) that embolizes to the lungs and causes fat embolism syndrome (FES), which is characterized by respiratory distress, neurological impairment, and petechial rash (1).
Compartment syndrome: Tissue pressure increases in a closed fascial space, disrupting the vascular supply and reducing tissue perfusion. Crush injuries or markedly comminuted fractures are a common cause, increasing tissue pressure as edema develops. Risk is high with forearm fractures that involve both the radius and ulna, tibial plateau fractures (proximal tibial fractures that extend into the joint space), or tibial shaft fractures (2). Untreated compartment syndrome can lead to rhabdomyolysis, hyperkalemia, and infection. Over the long term, it can cause contractures, sensory deficits, and paralysis. Compartment syndrome threatens limb viability (possibly requiring amputation) and survival.
Infection: Any fracture can become infected, but risk is highest with those that are open or surgically treated. Acute infection can lead to osteomyelitis, which can be difficult to cure.
Long-term complications of fractures include the following:
Instability: Various fractures can lead to joint instability. Instability can be disabling and increases the risk of osteoarthritis.
Stiffness and impaired range of motion: Fractures that extend into joints usually disrupt articular cartilage; misaligned articular cartilage tends to scar, causing osteoarthritis and impairing joint motion. Stiffness is more likely if a joint needs prolonged immobilization. The knee, elbow, and shoulder are particularly prone to posttraumatic stiffness, especially in older people.
Nonunion or delayed union: Occasionally, fractures do not heal (called nonunion), or union is delayed. Major contributing factors include incomplete immobilization, partial disruption of the vascular supply, and patient factors that impair healing (eg, use of corticosteroids or thyroid hormone).
Malunion: Malunion is healing with residual deformity. It is more likely if a fracture is not adequately reduced and stabilized.
Osteonecrosis: Part of a fracture fragment can become necrotic, primarily when the vascular supply is damaged. Closed fractures prone to osteonecrosis include scaphoid fractures, displaced femoral neck fractures, and displaced talar neck fractures.
Osteoarthritis: Fractures that disrupt the weight-bearing surfaces of joints or that result in joint malalignment and instability predispose to joint cartilage degeneration and osteoarthritis.
Limb length discrepancy: If a fracture in children involves a growth plate, growth can be affected, resulting in one limb that is shorter than the other. In adults, surgical repair of a fracture, especially femoral fractures, can result in leg length discrepancy (3), which can lead to difficulty walking and the need for a lift in the shoe for the shorter leg.
Complications references
1. Rothberg DL, Makarewich CA. Fat Embolism and Fat Embolism Syndrome. J Am Acad Orthop Surg. 2019;27(8):e346-e355. doi:10.5435/JAAOS-D-17-00571
2. McQueen MM, Gaston P, Court-Brown CM. Acute compartment syndrome. Who is at risk? J Bone Joint Surg Br. 82 (2):200–203, 2000. PMID: 10755426
3. Vaidya R, Anderson B, Elbanna A, et al. CT scanogram for limb length discrepancy in comminuted femoral shaft fractures following IM nailing. Injury. 43 (7):1176–1181, 2012. doi: 10.1016/j.injury.2012.03.022
Evaluation of Fractures
History and physical examination
Radiographs
Sometimes MRI or CT
In the emergency department, if the mechanism of injury suggests potentially severe or multiple injuries (eg, a high-speed motor vehicle crash or fall from a height), patients are first evaluated from head to toe for serious injuries to all organ systems and, if needed, are resuscitated (see Approach to the Trauma Patient). Patients, especially those with pelvic or femoral fractures, are evaluated for hemorrhagic shock due to occult blood loss. If a limb is injured, it is immediately evaluated for open wounds and symptoms or signs of neurovascular injury (numbness, paresis, poor perfusion) and compartment syndrome (eg, pain out of proportion to injuries, pallor, paresthesias, coolness, pulselessness).
Clinicians may suspect fractures based on symptoms and results of the physical examination, but imaging (usually radiographs) is required to confirm the diagnosis.
Patients should be checked for ligament, tendon, and muscle injuries as well as fractures. The presence of a fracture can limit this part of this evaluation (eg, stress testing cannot be done because pain is initially prohibitive).
The joint above and below the injury should also be examined, because concomitant injuries and referred pain are common.
History
The mechanism (eg, the direction and magnitude of force) may suggest the type of injury. However, many patients do not remember or cannot describe the exact mechanism.
A perceived snap or pop at the time of injury may signal a fracture (or a ligament or tendon injury). Fractures and serious ligamentous injuries usually cause immediate pain; pain that begins hours to days after the injury suggests minor injury. Pain that is out of proportion to the apparent severity of the injury or that steadily worsens in the first hours to days immediately after injury suggests compartment syndrome or ischemia.
Physical examination
Examination includes
Vascular and neurologic assessment distal to the injury
Inspection for open wounds, deformity, swelling, ecchymoses, and decreased or abnormal range of motion
Palpation for tenderness, crepitation, and gross defects in bone or tendon
Examination of the joints above and below the injured area (eg, for the shoulder joint, the cervical spine and elbow)
After fracture and dislocation are excluded (clinically or by imaging), stress testing of the affected joints for pain and instability
If muscle spasm and pain limit physical examination (particularly stress testing), examination is sometimes easier after the patient is given a systemic analgesic or local anesthetic. Or the fracture can be immobilized until muscle spasm subsides, usually for a few days, and then the patient can be reexamined.
Certain findings may indicate a fracture or another musculoskeletal injury.
Deformity may indicate a fracture, but it may also indicate dislocation or subluxation (partial separation of bones in a joint).
Swelling commonly indicates a fracture or other significant musculoskeletal injury but may require several hours to develop. If no swelling occurs within this time, fracture is unlikely. With some fractures (eg, buckle fractures, small fractures without displacement), swelling may be subtle, but it is rarely absent.
Tenderness accompanies nearly all musculoskeletal injuries, and for many patients, palpation anywhere around the injured area causes discomfort. However, a noticeable increase in tenderness in one localized area (point tenderness) suggests a fracture.
A defect may be palpable in the affected bone in some fractures.
Crepitus (a characteristic palpable and/or audible grinding produced when the joint is moved) may be a sign of fracture.
If a wound is near a fracture, the fracture is assumed to be open. Open fractures can be classified using the Gustilo-Anderson system (1):
Grade I: Wound < 1 cm, with minimal contamination, comminution, and soft-tissue damage
Grade II: Wound > 1 cm, with moderate soft-tissue damage and minimal periosteal stripping
Grade IIIA: Severe soft-tissue damage and substantial contamination, with adequate soft-tissue coverage
Grade IIIB: Severe soft-tissue damage and substantial contamination, with inadequate soft-tissue coverage
Grade IIIC: Open fracture with arterial injury requiring repair
Higher grades indicate a higher risk of infection and later osteomyelitis (2); however, interobserver reliability using this system is not high, and certain aspects can be best assessed intraoperatively.
Attention to certain areas during examination can help detect commonly missed injuries (see table Examination for Commonly Missed Fractures).
Examination for Commonly Missed Fractures
Symptom | Characteristic History | Physical Finding | Injury |
|---|---|---|---|
Hand pain | Hyperextension of the hand and wrist | Tenderness on the dorsal wrist | Triquetrum fracture |
Elbow pain | Fall on outstretched hand | Elbow pain when supinating and pronating the forearm | Radial head fracture |
Wrist pain or swelling | Fall on an outstretched hand | Tenderness over the anatomic snuffbox (located just distal to the radius, between the extensor pollicis longus, extensor pollicis brevis, and abductor pollicis longus tendons) | Scaphoid fracture |
Various mechanisms | Tenderness over the lunate fossa (in the wrist at the base of the 3rd metacarpal) and pain with axial compression of the 3rd metacarpal | Lunate fracture Lunate or perilunate dislocation | |
Hip pain | Fall | Pain during passive hip rotation when the knee is flexed Inability to flex the hip Leg externally rotated and shortened Inability to bear weight even though radiographs are normal (particularly in patients with osteoporosis) | Hip fracture |
Knee pain in a child or an adolescent | Various mechanisms | Pain during passive hip rotation when the knee is flexed | Hip injury (eg, slipped capital femoral epiphysis, Legg-Calvé-Perthes disease) |
Ankle pain | Fall or step into hole Twisting mechanism | Swollen and tender ankle Tenderness of lateral knee | Maisonneuve fracture (spiral fracture of the proximal third of the fibula plus a tear of the distal tibiofibular syndesmosis and the interosseous membrane) |
For other commonly missed injuries, see tables Examination for Some Commonly Missed Soft-Tissue Injuries and Examination for Some Commonly Missed Injuries. | |||
If physical examination is normal in a joint that patients identify as painful, the cause may be referred pain. For example, patients with a slipped capital femoral epiphysis (or less often hip fracture) may feel pain in their knee.
Imaging
Not all suspected fractures require imaging. Some fractures are minor and are treated similarly to soft-tissue injuries. For example, most injuries of toes 2 through 5 and many fingertip injuries are treated symptomatically whether a fracture is present or not; thus, radiographs are not needed. For example, in many patients with ankle injuries, the probability of finding a fracture that would require a change in treatment is acceptably low, so radiographs are not always needed. Clinical decision rules that help determine which patients are more likely to have a fracture requiring specific treatment (eg, Ottawa ankle rules) can help determine which patients need radiographs (3).
If imaging is needed, radiographs are done first.
Radiographs show primarily bone (and joint effusion secondary to bleeding or occult fracture) and thus are useful for diagnosing fractures. They should include at least 2 views taken in different planes (usually anteroposterior and lateral views).
Additional views (eg, oblique) may be done when
The evaluation suggests fracture and 2 projections are negative.
They are routine for certain joints (eg, a mortise view for evaluating an ankle, an oblique view for evaluating a foot).
Certain abnormalities are suspected.
For lateral views of digits, the digit of interest should be separated from the others.
MRI or CT may be used if
A fracture is not visible on radiographs but is strongly suspected clinically (common with scaphoid fractures and impacted femoral neck [subcapital] hip fractures).
More detail is needed to guide treatment (eg, for scapular fractures, pelvic fractures, or intraarticular fractures).
For example, if findings after a fall suggest hip fracture but radiographs are normal, CT or MRI should be done to check for an occult hip fracture.
Other tests may be done to check for related injuries:
Arteriography or CT angiography to check for suspected arterial injuries (eg, to evaluate the popliteal artery when the knee is dislocated)
Electromyography and/or nerve conduction studies (rarely done immediately; more typically done when nerve symptoms persist weeks to months after the injury)
Fracture description


LIVING ART ENTERPRISES/SCIENCE PHOTO LIBRARY
A fracture’s appearance on radiograph can be described by:
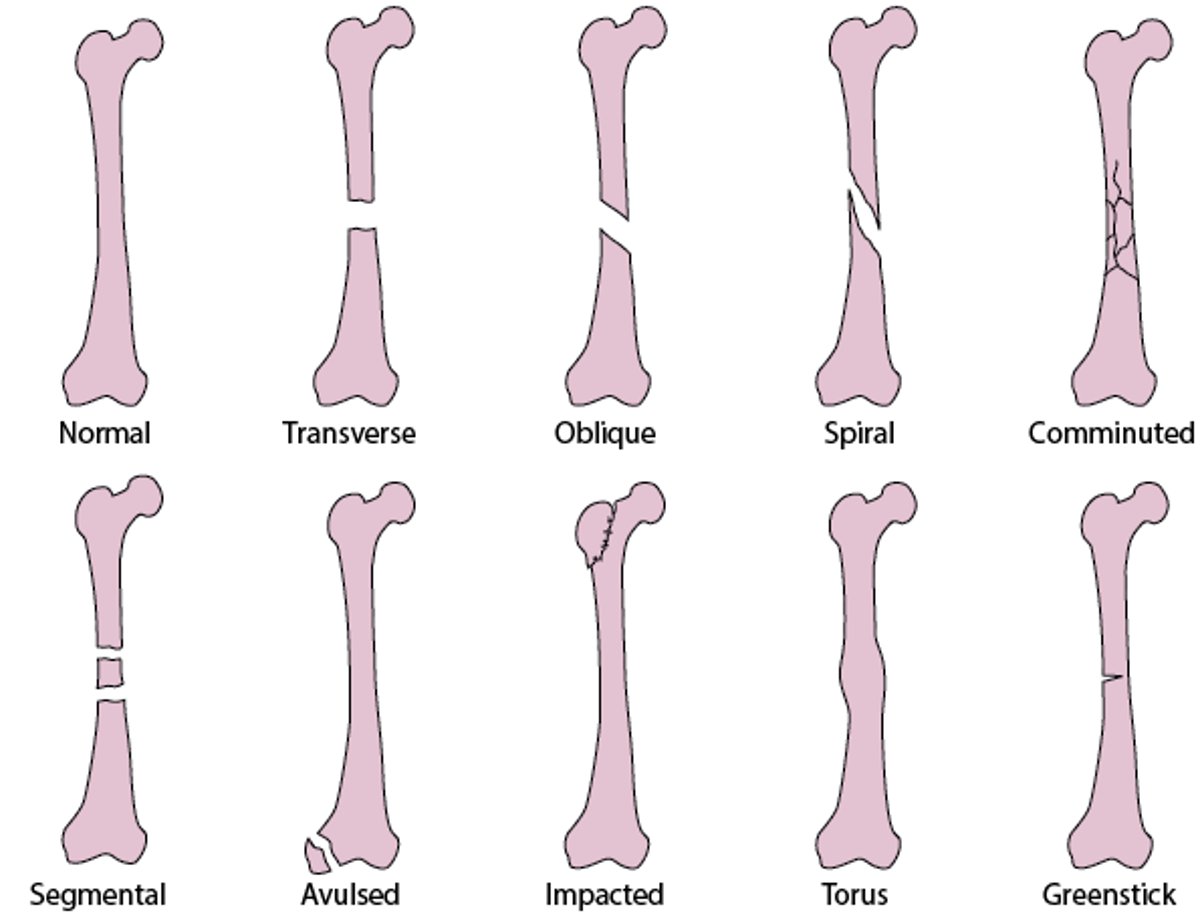
Type of fracture line (see figure Common Types of Fracture Lines)
Location of fracture line
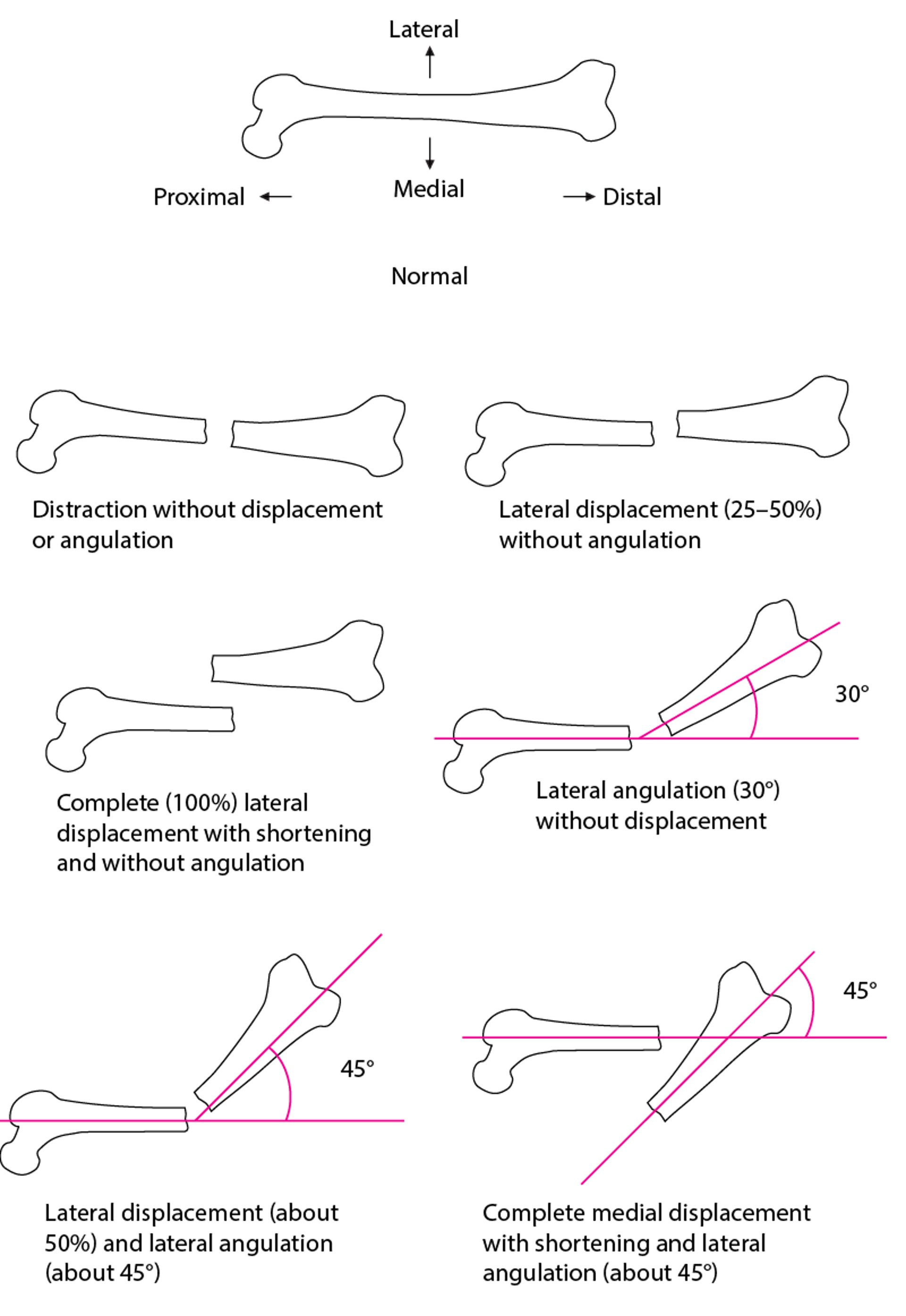
Displacement (see figure Spatial Relationship Between Fracture Fragments)
Open or closed
Terms for fracture location include:
Dorsal or volar
Epiphysis (sometimes involving the articular surface), which can refer to the proximal end of the bone (the head) or the distal end
Metaphysis (neck—the part of a long bone between the epiphysis and diaphysis)
Diaphysis (shaft, divided into the proximal, middle, or distal third)
Common Types of Fracture Lines
Transverse fractures are perpendicular to the long axis of a bone. Oblique fractures occur at an angle. Spiral fractures result from a rotatory mechanism; on radiographs, they are differentiated from oblique fractures by a component parallel to the long axis of bone in at least 1 view. Comminuted fractures have > 2 bone fragments. Comminuted fractures include segmental fractures (2 separate breaks in a bone). Avulsion fractures are caused by a tendon dislodging a bone fragment. In impacted fractures, bone fragments are driven into each other, shortening the bone; these fractures may be visible as a focal abnormal density in trabeculae or irregularities in bone cortex. Torus fractures (buckling of the bone cortex) and greenstick fractures (cracks in only 1 side of the cortex) are childhood fractures. |



This transverse fracture affects the midshaft of the tibia.
Image courtesy of Danielle Campagne, MD.

Torus fractures may be visible only as subtle irregularities in bone cortex.
PHOTOSTOCK-ISRAEL/SCIENCE PHOTO LIBRARY

This torus fracture of the distal radius is visible only as a slight irregularity of the bone cortex.
LIVING ART ENTERPRISES, LLC/SCIENCE PHOTO LIBRARY


This ankle fracture involves the medial malleolus (of the tibia) and lateral malleolus (of the fibula).
SCIENCE PHOTO LIBRARY

This radiograph shows a greenstick fracture of the distal radius, visible as a discontinuity (step-off) in the radial aspect of the cortex (arrow).
ZEPHYR/SCIENCE PHOTO LIBRARY


This image shows a comminuted, angulated, and shortened midshaft femur fracture.
Image courtesy of Danielle Campagne, MD.

This lateral femur radiograph shows a midshaft femur fracture with soft tissue air and retained metallic density foreign bodies.
Image courtesy of Danielle Campagne, MD.
This transverse fracture affects the midshaft of the tibia.
Image courtesy of Danielle Campagne, MD.
Torus fractures may be visible only as subtle irregularities in bone cortex.
PHOTOSTOCK-ISRAEL/SCIENCE PHOTO LIBRARY
This torus fracture of the distal radius is visible only as a slight irregularity of the bone cortex.
LIVING ART ENTERPRISES, LLC/SCIENCE PHOTO LIBRARY
This ankle fracture involves the medial malleolus (of the tibia) and lateral malleolus (of the fibula).
SCIENCE PHOTO LIBRARY
This radiograph shows a greenstick fracture of the distal radius, visible as a discontinuity (step-off) in the radial aspect of the cortex (arrow).
ZEPHYR/SCIENCE PHOTO LIBRARY
This image shows a comminuted, angulated, and shortened midshaft femur fracture.
Image courtesy of Danielle Campagne, MD.
This lateral femur radiograph shows a midshaft femur fracture with soft tissue air and retained metallic density foreign bodies.
Image courtesy of Danielle Campagne, MD.
Spatial Relationship Between Fracture Fragments
Distraction, displacement, angulation, or shortening (overriding) may occur. Distraction is separation in the longitudinal axis. Displacement is the degree to which the fractured ends are out of alignment with each other; it is described in millimeters or bone width percentage. Angulation is the angle of the distal fragment measured from the proximal fragment. Displacement and angulation may occur in the ventral-dorsal plane, lateral-medial plane, or both. |

Evaluation references
1. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976;58(4):453-458.
2. Kim PH, Leopold SS. In brief: Gustilo-Anderson classification. [corrected] [published correction appears in Clin Orthop Relat Res. 2012 Dec;470(12):3624] [published correction appears in Clin Orthop Relat Res. 2019 Oct;477(10):2388. doi: 10.1097/CORR.0000000000000950]. Clin Orthop Relat Res. 2012;470(11):3270-3274. doi:10.1007/s11999-012-2376-6
3. Gomes YE, Chau M, Banwell HA, Causby RS. Diagnostic accuracy of the Ottawa ankle rule to exclude fractures in acute ankle injuries in adults: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2022;23(1):885. Published 2022 Sep 23. doi:10.1186/s12891-022-05831-7
Treatment of Fractures
Reduction as indicated, splinting, and analgesia
RICE (rest, ice, compression, and elevation) or PRICE (protection [with a splint or cast], rest, ice, compression, and elevation) as indicated
Usually immobilization
Sometimes surgery
Treatment of associated injuries
Initial treatment
Serious associated problems, if present, are treated first. Hemorrhagic shock is treated immediately. Injuries to arteries are surgically repaired unless they affect only small arteries with good collateral circulation. Compartment syndrome is treated, if present.
Severed nerves are surgically repaired; for neuropraxia and axonotmesis, initial treatment is usually observation, supportive measures, and sometimes physical therapy.
Suspected open fractures require sterile wound dressings, tetanus prophylaxis, broad-spectrum antibiotics (eg, a second-generation cephalosporin plus an aminoglycoside), and surgery to irrigate and debride them (and thus prevent infection). To minimize the risk of infection in open fractures, IV antibiotics should be given early, for example, within 1 hour of emergency department presentation (1).
Most moderate and severe fractures, particularly grossly unstable ones or ones with deformities that cause skin tenting with possible skin necrosis, are reduced and immobilized immediately by splinting (immobilization with a nonrigid or noncircumferential device) to decrease pain and to prevent further injury to soft tissues by unstable fractures. In patients with long-bone fractures, splinting may prevent fat embolism.
Pain is treated as soon as possible, typically with opioids or regional nerve blocks. If a patient has an isolated extremity fracture and compartment syndrome is not suspected, regional anesthesia may be used; this approach can help minimize the use of opioids and provides greater pain relief than opioids alone (2).
After initial treatment, fractures are reduced, immobilized, and treated symptomatically as indicated.
Reduction
Rotational malalignment or significant angulation or displacement of fractures is typically treated with reduction (realignment of bones or bone fragments by manipulation), which usually requires analgesia and/or sedation. Exceptions include some fractures in children in whom remodeling over time can correct significant deformities.
Closed reduction (by manipulation, without skin incision) is done when possible. If closed reduction is not possible, open reduction (with skin incision) is done; anesthesia is required.
Closed reduction of fractures is usually maintained by casting, but some fractures require only a splint or sling.
Open reduction of fractures is usually maintained by various surgical hardware, external and/or internal. In open reduction with internal fixation (ORIF), fracture fragments are aligned and held in place using a combination of pins, screws, and plates. ORIF is usually indicated when
Intra-articular fractures are displaced (to precisely align the joint surface).
ORIF has better results than nonsurgical treatment for some types of fracture.
Closed reduction was ineffective.
Pathologic fractures occur in a bone weakened by cancer; such bone does not heal normally, and ORIF reduces pain more quickly than other treatments and makes early ambulation possible.
Prolonged immobility (required for fracture healing) is undesirable (eg, for hip or femoral shaft fractures); ORIF provides early structural stability, minimizes pain, and facilitates mobilization.
PRICE
PRICE (protection, rest, ice, compression, elevation) may be beneficial.
Protection helps prevent further injury. It may involve limiting the use of an injured part, applying a splint or cast, or using crutches.
Rest may prevent further injury and speed healing.
Ice and compression may minimize swelling and pain. Ice is enclosed in a plastic bag or towel and applied intermittently during the first 24 to 48 hours (for 15 to 20 minutes, as often as possible). Injuries can be compressed by a splint, an elastic bandage, or, for certain injuries likely to cause severe swelling, a Jones compression dressing. The Jones dressing is 4 layers; layers 1 (the innermost) and 3 are cotton batting, and layers 2 and 4 are elastic bandages.
Elevation of the injured limb above the heart for the first 2 days in a position that provides an uninterrupted downward path; such a position allows gravity to help drain edema fluid and minimize swelling.
After 48 hours, periodic application of warmth (eg, a heating pad) for 15 to 20 minutes may relieve pain and speed healing.
Immobilization
Immobilization decreases pain and facilitates healing by preventing further injury and keeping the fracture ends in alignment. Joints proximal and distal to the injury should be immobilized.
Most fractures are immobilized for weeks in a cast (a rigid, circumferential device). A few rapidly healing, stable fractures (eg, buckle wrist fractures in children) are not casted; early mobilization has the best results.
A cast is usually used for fractures that require weeks of immobilization. Rarely, swelling under a cast is severe enough to contribute to compartment syndrome. If clinicians suspect severe swelling under a cast, the cast (and all padding) is cut open from end to end medially and laterally (bivalved).
Patients with casts should be given written instructions, including the following:
Keep the cast dry.
Keep the exposed area of skin around the edges of the cast clean and dry.
Never put an object inside the cast.
Inspect the cast’s edges and skin around the cast every day and report any red or sore areas.
Pad any rough edges with soft adhesive tape, cloth, or other soft material to prevent the cast’s edges from injuring the skin.
When resting, position the cast carefully, possibly using a small pillow or pad, to prevent the edge from pinching or digging into the skin.
Elevate the cast whenever possible to control swelling.
Seek medical care immediately if pain persists or the cast feels excessively tight.
Seek medical care immediately if an odor emanates from within the cast or if a fever, which may indicate infection, develops.
Seek care immediately for progressively worsening pain or any new numbness or weakness, which may indicate compartment syndrome.
A splint (see figure Joint Immobilization as Acute Treatment: Some Commonly Used Techniques) can be used to immobilize some stable injuries, including some suspected but unproven fractures and rapidly healing fractures that require immobilization for several days or less. A splint is noncircumferential; thus, it enables patients to apply ice and to move more than a cast does. Also, it allows for some swelling, so it does not contribute to compartment syndrome. Some injuries that ultimately require casting are immobilized initially with a splint until most of the swelling resolves.



© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.
© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.








© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.






Joint Immobilization as Acute Treatment: Some Commonly Used Techniques

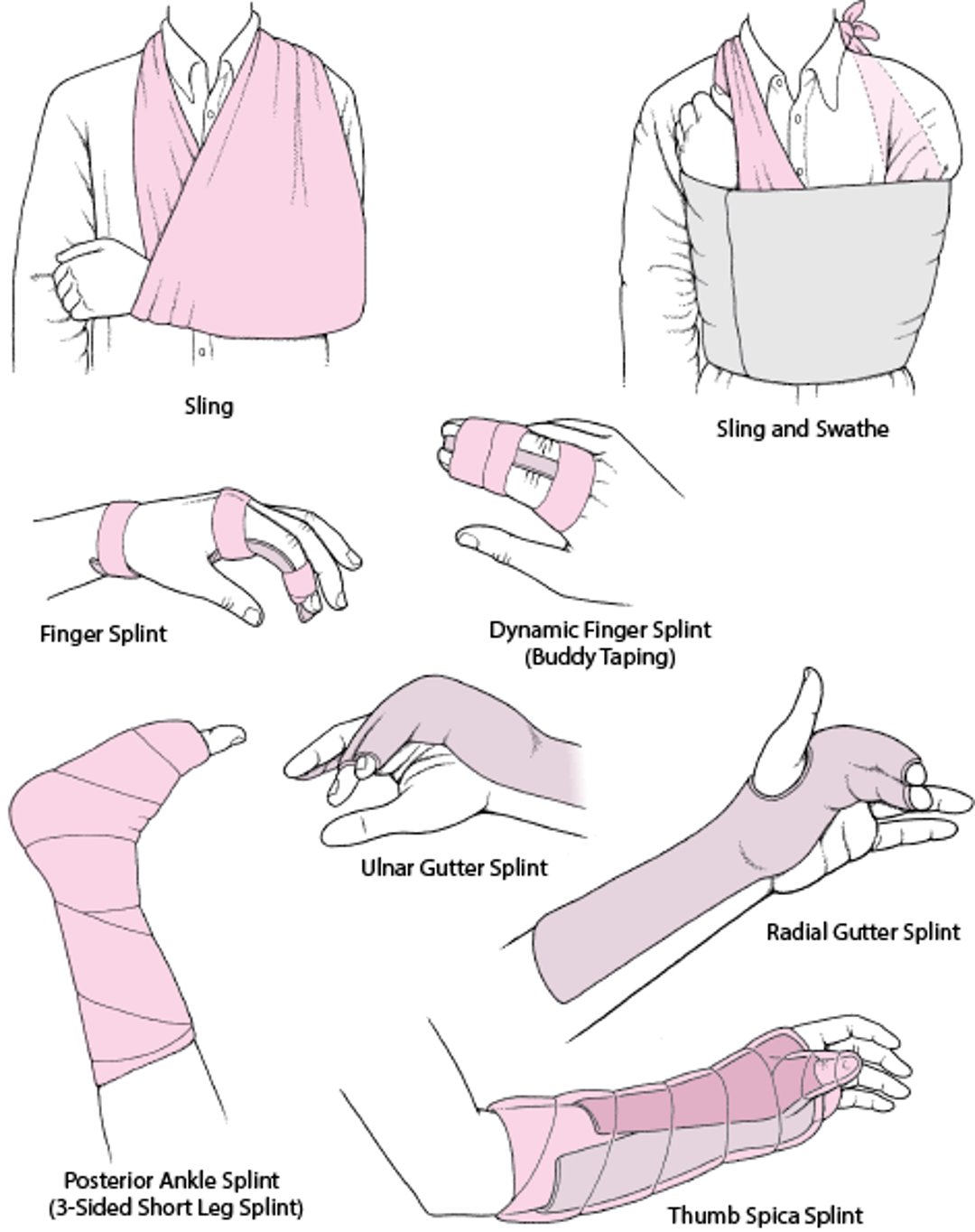
A sling provides some degree of support and comfort and limits mobility; it can be useful for certain fractures (eg, minimally displaced clavicle fractures, certain proximal humerus fractures), particularly if complete immobilization is undesirable (eg, for shoulder injuries, which, if completely immobilized, can rapidly lead to adhesive capsulitis [frozen shoulder]).

A swathe (a piece of cloth or a strap) may be used with a sling to prevent the arm from swinging outward, especially at night. The swathe is wrapped around the back and over the injured part. A swathe is sometimes used with a sling to immobilize one-part proximal humeral fractures.
Bed rest, which is occasionally required for fractures (eg, some vertebral or pelvic fractures), can cause problems (eg, deep venous thrombosis, urinary tract infection, muscle deconditioning).
Prolonged immobilization of a joint can cause stiffness, contractures, and muscle atrophy and is usually not recommended. These complications may develop rapidly and may be permanent, particularly in older people. Some rapidly healing injuries are best treated with resumption of active motion within the first few days or weeks. Early mobilization may minimize contractures and muscle atrophy, thus accelerating functional recovery. Splints and casts should immobilize joints in positions that optimize the likelihood of return of full function (eg, immobilization of the metacarpophalangeal [MCP] joints should position the MCP joints in flexion to maintain lengthening of the hand tendons).
Physical therapists can advise patients about what they can do during immobilization to maintain as much function as possible. After immobilization, physical therapists can provide patients with exercises to improve range of motion and muscle strength, strengthen and stabilize the injured joint, and thus help prevent recurrence and long-term impairment.
Other procedures
Joint replacement (arthroplasty) may be needed, usually when fractures severely damage the upper end of the femur or the humerus.
Bone grafting may be done immediately if the gap between fragments of bone is too large. It may be done later if healing is delayed (delayed union) or does not occur (nonunion).
Treatment references
1. Lack WD, Karunakar MA, Angerame MR, et al. Type III open tibia fractures: immediate antibiotic prophylaxis minimizes infection. J Orthop Trauma. 29(1):1–6, 2015. doi: 10.1097/BOT.0000000000000262. Erratum in: J Orthop Trauma. 29(6):e213, 2015. PMID: 25526095
2. Beaudoin FL, Haran JP, Liebmann O. A comparison of ultrasound-guided three-in-one femoral nerve block versus parenteral opioids alone for analgesia in emergency department patients with hip fractures: A randomized controlled trial. Acad Emerg Med. 20(6):584–591, 2013. doi: 10.1111/acem.12154
Geriatrics Essentials: Fractures
Older adults are predisposed to fractures because of the following:
A tendency to fall frequently (eg, due to age-related loss of proprioception, adverse effects of medications on proprioception or postural reflexes, orthostatic hypotension)
Impaired protective reflexes during falls
Osteoporosis, which becomes more common with aging
Common fractures from falls include fractures of the distal radius, proximal humerus, pelvis, proximal femur, and vertebrae.
For older patients, the goal of treatment is rapid return to activities of daily living rather than restoration of perfect limb alignment and length.
Because immobility (joint immobilization or bed rest) is more likely to have adverse effects (eg, deconditioning, pressure sores) in older patients, use of open reduction with internal fixation (ORIF) to treat fractures of the lower extremity is preferred in older patients without health concerns that would make surgery unacceptably risky.
Early mobilization (made possible by ORIF) and physical therapy are essential to recovery of function.
Coexisting disorders (eg, arthritis) can interfere with recovery.
Key Points
Fractures that disrupt arterial supply and/or result in compartment syndrome threaten limb viability and may ultimately threaten life.
Check for ligament, tendon, and muscle injuries as well as fractures; the presence of a fracture may limit or delay this evaluation.
Examine the joints above and below the injured area.
Consider referred pain, particularly if physical findings are normal in a joint that patients identify as painful (eg, knee pain in patients with a hip fracture).
For many distal extremity injuries (eg, some injuries in toes 2 through 5, some ankle sprains), radiographs are not necessary to check for fractures because the presence of a fracture would not change treatment.
Consider MRI (sometimes CT) when radiographs are normal but a fracture is strongly suspected clinically (eg, in an older adult who has hip pain and cannot walk after a fall and initial radiographs are normal).
Immediately treat serious associated injuries, splint unstable fractures, and, as soon as possible, treat pain and reduce certain angulated or displaced fractures.
Immobilize unstable fractures immediately; use a cast or splint to immobilize all fractures that require reduction as soon as they are reduced.
Treat fractures with PRICE (protection, rest, ice, compression, elevation).
Provide patients with explicit, written instructions about cast care.
When treating older patients, usually choose the method that results in the earliest mobilization.







