



- Overview of Peripheral Nervous System Disorders
- Disorders of Neuromuscular Transmission
- Isaacs Syndrome
- Stiff-Person Syndrome
- Guillain-Barré Syndrome (GBS)
- Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)
- Hereditary Neuropathies
- Hereditary Motor Neuropathy With Liability to Pressure Palsies (HNPP)
- Amyotrophic Lateral Sclerosis (ALS) and Other Motor Neuron Diseases (MNDs)
- Myasthenia Gravis
- Nerve Root Disorders
- Peripheral Neuropathy
- Mononeuropathies
- Multiple Mononeuropathy
- Polyneuropathy
- Brachial Plexus and Lumbosacral Plexus Disorders
- Spinal Muscular Atrophies (SMAs)
- Thoracic Outlet Compression Syndromes (TOS)
Disorders of the brachial or lumbosacral plexus cause a painful mixed sensorimotor disorder of the corresponding limb.
Topic Resources

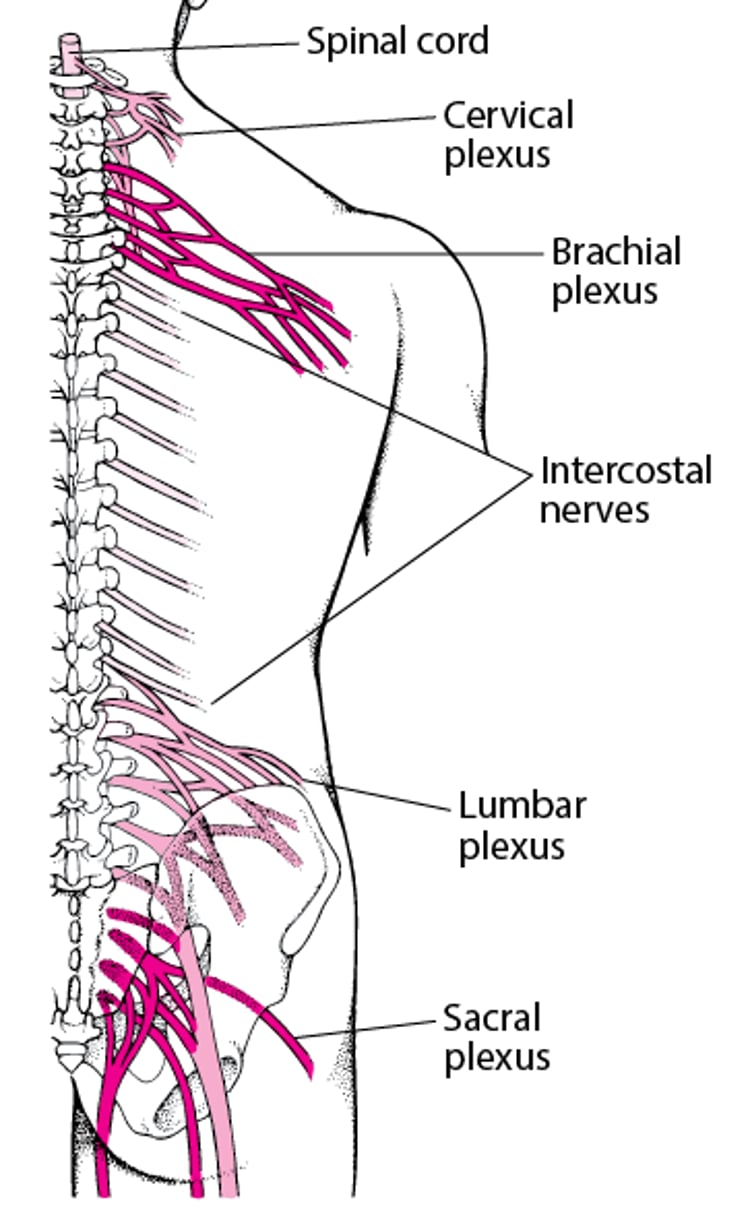
Because several nerve roots intertwine within the plexus (see figure Plexuses), the symptom pattern does not fit the distribution of individual roots or nerves. Which parts of the body are affected depends on which plexus is damaged:
Rostral brachial plexus: Shoulders
Caudal brachial plexus: Hands
Lumbar plexus: Legs
Sacral plexus: Pelvis and legs
Plexuses

Plexus disorders (plexopathies) are usually due to physical compression or injury:
In infants, traction during birth if it damages nerves in the brachial plexus
In adults, usually trauma (typically, for the brachial plexus, a fall that forces the head away from the shoulder) or invasion by metastatic cancer (typically, breast or lung cancer for the brachial plexus and intestinal or genitourinary tumors for the lumbosacral plexus)
In patients receiving anticoagulants, a hematoma may compress the lumbosacral plexus. Neurofibromatosis occasionally involves a plexus. Other causes include postradiation fibrosis (eg, after radiation therapy for breast cancer) and diabetes.
Acute brachial neuritis (neuralgic amyotrophy, Parsonage-Turner syndrome) occurs primarily in men and typically in young adults, although it can occur at any age. Cause is unknown, but viral or immunologic inflammatory processes are suspected.
Symptoms and Signs of Plexus Disorders
Manifestations of plexus disorders include extremity pain and motor or sensory deficits that do not correspond to an isolated nerve root or peripheral nerve distribution.
For acute brachial neuritis, findings include severe supraclavicular pain, weakness, and diminished reflexes, with minor sensory abnormalities in the distribution of the brachial plexus. Usually, weakness develops and reflexes decrease as pain resolves. Severe weakness develops within 3 to 10 days, then typically regresses over the next few months. The most commonly affected muscles are the serratus anterior (causing winging of the scapula), other muscles innervated by the upper trunk, and muscles innervated by the anterior interosseous nerve in the forearm—patients may not be able to make an ο with the thumb and index finger.
Diagnosis of Plexus Disorders
Electromyography and nerve conduction studies
Usually MRI or CT of the appropriate plexus
Diagnosis of a plexus disorder is suggested by clinical findings.
Electromyography and nerve conduction studies should be done to clarify the anatomic distribution (including possible nerve root involvement).
MRI or CT of the appropriate plexus and adjacent spine is done to detect abnormalities such as tumors and hematomas. MRI or CT is indicated for all nontraumatic and traumatic plexopathies except typical cases of brachial neuritis.
Treatment of Plexus Disorders
Treatment directed at the cause
Corticosteroids, although commonly prescribed, have no proven benefit in plexus disorders.
Surgery may be indicated for injuries, hematomas, and benign or metastatic tumors. Metastases should also be treated with radiation therapy, chemotherapy, or both.
Glycemic control can benefit patients with diabetic plexopathy.
Key Points
Plexopathies are usually caused by compression or injury.
Suspect a plexopathy if pain or peripheral neurologic deficits do not correspond to a nerve root or peripheral nerve distribution.
Suspect acute brachial neuritis if patients have severe supraclavicular pain, followed by weakness and hyporeflexia that develop within days and resolve over months.
In most cases, do electromyography and MRI or CT.
Treat the cause.







