



- Overview of Peripheral Nervous System Disorders
- Disorders of Neuromuscular Transmission
- Isaacs Syndrome
- Stiff-Person Syndrome
- Guillain-Barré Syndrome (GBS)
- Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)
- Hereditary Neuropathies
- Hereditary Motor Neuropathy With Liability to Pressure Palsies (HNPP)
- Amyotrophic Lateral Sclerosis (ALS) and Other Motor Neuron Diseases (MNDs)
- Myasthenia Gravis
- Nerve Root Disorders
- Peripheral Neuropathy
- Mononeuropathies
- Multiple Mononeuropathy
- Polyneuropathy
- Brachial Plexus and Lumbosacral Plexus Disorders
- Spinal Muscular Atrophies (SMAs)
- Thoracic Outlet Compression Syndromes (TOS)
Single mononeuropathies are characterized by sensory disturbances and weakness in the distribution of the affected peripheral nerve. Diagnosis is clinical but may require confirmation with electrodiagnostic tests. Treatment is directed at the cause, sometimes with splinting, nonsteroidal anti-inflammatory drugs, corticosteroid injections, and, for severe cases of nerve entrapment, surgery.
Topic Resources

(See also Overview of Peripheral Nervous System Disorders.)
Etiology of Mononeuropathies
Trauma is the most common cause of acute mononeuropathy and may occur as follows:
Violent muscular activity or forcible overextension of a joint may cause focal neuropathy, as may repeated small traumas (eg, tight gripping of small tools, excessive vibration from air hammers).
Prolonged, uninterrupted pressure at bony prominences can cause pressure neuropathy, usually affecting superficial nerves (ulnar, radial, peroneal), particularly in thin people; such pressure may occur during sound sleep, intoxication, bicycle riding, or anesthesia.
Compression of nerves in narrow passageways causes entrapment neuropathy (eg, in carpal tunnel syndrome).
Nerve compression by a tumor, hyperostosis, a cast, crutches, or prolonged cramped postures (eg, during gardening) may cause compression paralysis.
Hemorrhage that compresses a nerve, exposure to cold or radiation, or direct tumor invasion may also cause neuropathy.
Compression of a nerve may be transient (eg, caused by an activity) or fixed (eg, caused by a mass or anatomic abnormality).
Symptoms and Signs of Mononeuropathies
Single mononeuropathies are characterized by pain, weakness, and paresthesias in the distribution of the affected nerve or nerves. Pure motor nerve involvement begins with painless weakness; pure sensory nerve involvement begins with sensory disturbances and no weakness.
Carpal tunnel syndrome
Carpal tunnel syndrome is the most common mononeuropathy. It may be unilateral or bilateral. It results from compression of the median nerve in the volar aspect of the wrist between the transverse superficial carpal ligament and the flexor tendons of the forearm muscles.
Risk factors for carpal tunnel syndrome include
Pregnancy
Certain forms of amyloidosis
Work that requires repeated forceful movements with the wrist extended (eg, using a screwdriver)
Possibly use of a computer keyboard that is not positioned correctly (controversial)
However, most cases are idiopathic.
The compression causes paresthesias in the radial-palmar aspect of the hand and pain in the wrist and palm. Pain may be referred to the forearm and shoulder. Pain may be more severe at night. A sensory deficit in the palmar aspect of the first 3 fingers may follow, and the muscles that control thumb abduction and opposition may become weak and atrophied.
Sensory symptoms due to carpal tunnel syndrome are similar to those due to C6 root dysfunction secondary to cervical radiculopathy.
Peroneal nerve palsy
Peroneal nerve palsy is usually caused by compression of the nerve against the lateral aspect of the fibular neck. It is most common among emaciated bedbound patients and thin people who habitually cross their legs.
Peroneal nerve palsy causes footdrop (weakened dorsiflexion and eversion of the foot) and, occasionally, a sensory deficit in the anterolateral aspect of the lower leg and the dorsum of the foot or in the web space between the 1st and 2nd metatarsals.
L5 radiculopathy can cause similar deficits but, unlike peroneal nerve palsy, tends to weaken hip abduction by the gluteus medius.
Radial nerve palsy
Radial nerve palsy (Saturday night palsy) is caused by compression of the nerve against the humerus, as when the arm is draped over the back of a chair for a long time (eg, during intoxication or deep sleep).
Typical symptoms of radial nerve palsy include wristdrop (weakness of the wrist and finger extensors) and sensory loss in the dorsal aspect of the first dorsal interosseous muscle.
C7 radiculopathy can cause similar motor deficits.
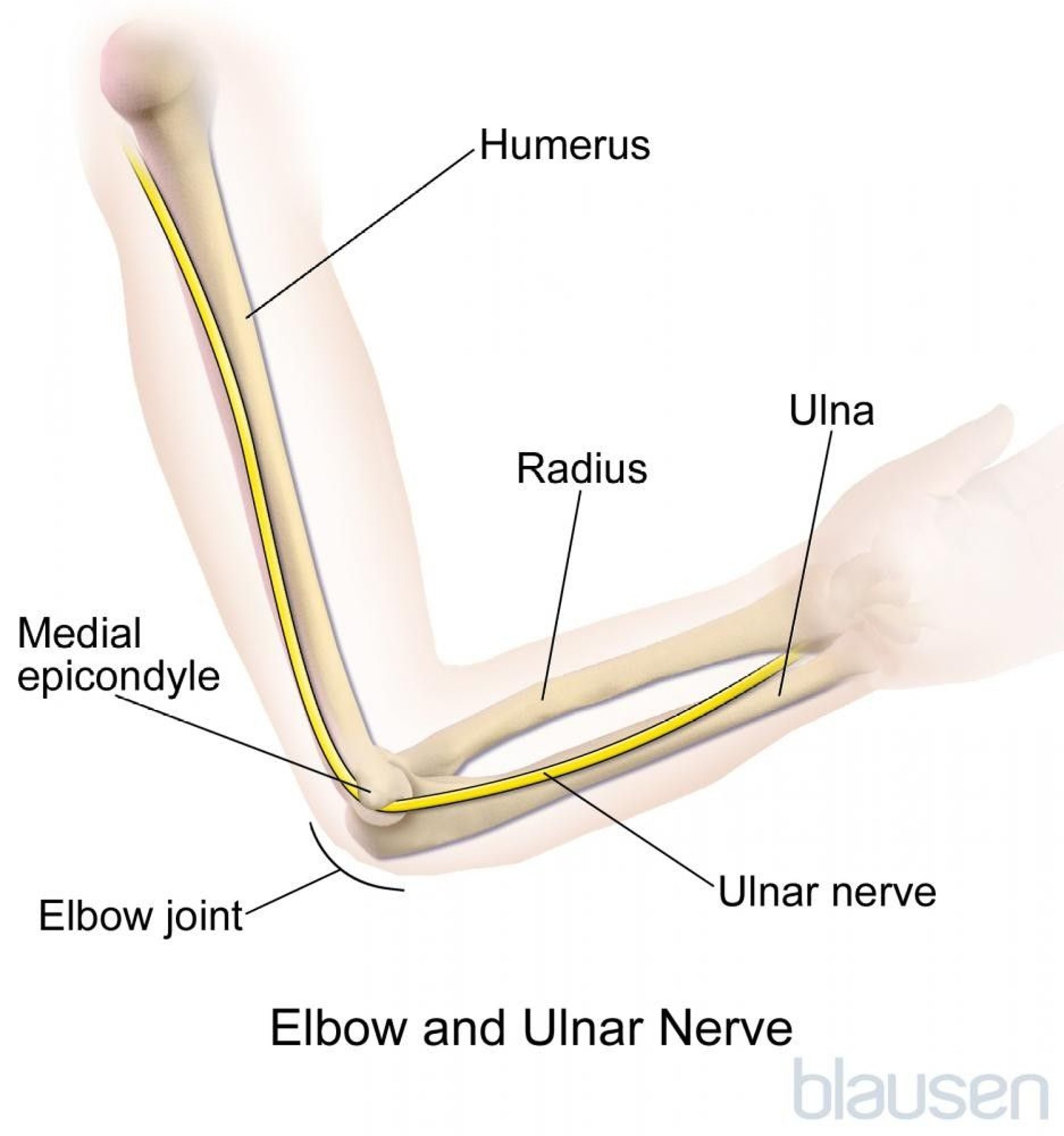
Ulnar nerve palsy
Ulnar nerve palsy at the elbow is often caused by trauma to the nerve in the ulnar groove of the elbow by repeated leaning on the elbow or by asymmetric bone growth after a childhood fracture (tardy ulnar palsy). The ulnar nerve can also be compressed as it runs under the medial epicondyle through tissue forming the cubital tunnel (sometimes causing cubital tunnel syndrome).
Compression at the level of the elbow can cause paresthesias and a sensory deficit in the 5th digit and medial half of the 4th digit; the thumb adductor, 5th digit abductor, and interosseus muscles are weak and may be atrophied. Severe chronic ulnar palsy causes a clawhand deformity.

Sensory symptoms due to ulnar nerve palsy are similar to those due to C8 root dysfunction secondary to cervical radiculopathy; however, radiculopathy normally affects the more proximal aspects of the C8 dermatome.
Diagnosis of Mononeuropathies
Clinical evaluation
Electrodiagnostic testing if clinical diagnosis is inconclusive
Symptoms and examination findings may be nearly pathognomonic for specific mononeuropathies.
Electrodiagnostic tests are usually done to clarify the diagnosis, particularly when clinical findings are inconclusive—for example,
To distinguish sensory symptoms due to ulnar nerve palsy from C8 root dysfunction due to cervical radiculopathy
To distinguish sensory symptoms due to carpal tunnel syndrome from C6 root dysfunction due to cervical radiculopathy
Electrodiagnostic tests also help localize the lesion, assess severity, and estimate prognosis.
Treatment of Mononeuropathies
Various treatments depending on the cause
Underlying disorders are treated.
Treatment of compression neuropathy depends on cause:
Fixed compression (eg, by tumor) often must be relieved surgically.
For transient compression, rest, heat, limited courses of nonsteroidal anti-inflammatory drugs (NSAIDs) in doses that reduce inflammation (eg, ibuprofen 800 mg 3 times a day), and avoidance or modification of the causative activity usually relieve symptoms.rest, heat, limited courses of nonsteroidal anti-inflammatory drugs (NSAIDs) in doses that reduce inflammation (eg, ibuprofen 800 mg 3 times a day), and avoidance or modification of the causative activity usually relieve symptoms.
For carpal tunnel syndrome, conservative therapy includes splinting the wrist, oral or injected corticosteroids, and ultrasound. For refractory cases, surgical release is usually effective.
Braces or splints are often used pending resolution to prevent contractures.
Surgery should be considered when progression occurs despite conservative treatment.
Key Points
If findings indicate that a single nerve is affected, trauma is the most likely cause.
Do electrodiagnostic tests if necessary to distinguish mononeuropathies from radiculopathies and other disorders that cause similar symptoms.
For transient nerve compression, advising patients to avoid the causative activity may be all that is needed; in other patients, consider surgery when progression occurs despite conservative treatment.







