








 Diameter in Emphysema")

Key components in the evaluation of patients with pulmonary symptoms are the history, physical examination, and, in many cases, a chest radiograph. These components establish the need for subsequent testing, which may include pulmonary function testing, arterial blood gas (ABG) analysis, chest CT and other chest imaging tests, echocardiography, 6-minute walk test, cardiopulmonary exercise testing, right heart catheterization, bronchoscopy, and lung biopsy.
History
The history can establish whether symptoms of cough, dyspnea, chest pain, wheezing, stridor, and hemoptysis are likely to be pulmonary in origin. A history should also establish whether constitutional symptoms, such as fever, weight loss, and night sweats, are present. Other important information includes
Occupational and environmental exposures
Family history, travel history, and contact history
Previous illnesses and comorbidities
Use of prescription or over-the-counter medications or illicit drugs
Use of tobacco products or other inhaled substances
Previous test results (eg, tuberculin skin test, chest radiographs)
Physical Examination
Physical examination includes an assessment of general appearance. Discomfort and anxiety, body habitus, and the effect of talking or movement on symptoms (eg, inability to speak full sentences without pausing to breathe) can all be assessed while greeting the patient and taking a history, and these assessments may provide useful information relevant to pulmonary status. A thorough pulmonary examination constitutes inspection, auscultation, and chest percussion and palpation. Patients with lung disease should undergo a complete physical examination, including examination of the skin, oral cavity, lymph nodes, neck veins, heart, extremities, and the musculoskeletal system.
Inspection
Inspection should focus on the following:
Signs of respiratory difficulty and hypoxemia (eg, tachypnea, cyanosis, accessory muscle use)
Signs of possible chronic pulmonary disease (eg, clubbing, elevated jugular venous pressure, pedal edema)
Chest wall deformities
Abnormal breathing patterns (eg, prolonged expiratory time, Cheyne-Stokes respiration, Kussmaul respirations)
A sign of hypoxemia is cyanosis (bluish discoloration of the lips, face, or nail beds), which requires the presence of at least 5 g/dL (50 g/L) of unsaturated hemoglobin and thus signifies low arterial oxygen saturation (< 85%); the absence of cyanosis does not exclude the presence of hypoxemia, and the reliability of this sign depends on the underlying hemoglobin level. Depending on the skin color of the patient, cyanosis may be most visible in mucous membranes or nail beds.
Signs of respiratory difficulty include tachypnea, use of accessory respiratory muscles (sternocleidomastoids, intercostals, scalenes) to breathe, intercostal retractions, and paradoxical breathing. Patients with chronic obstructive pulmonary disease (COPD) sometimes brace their arms against their legs or the examination table while seated (ie, tripod position) in a subconscious effort to provide more leverage to accessory muscles and thereby enhance respiration. Intercostal retractions (inward movement of the rib interspaces) are common among infants and older patients with severe airflow limitation. Paradoxical breathing (inward motion of the abdomen during inspiration) signifies respiratory muscle fatigue or weakness.
Signs of possible chronic pulmonary disease include clubbing, barrel chest (the increased anterior-posterior diameter of the chest present in some patients with emphysema), and pursed lip breathing. Jugular vein distention and lower extremity edema can be signs of right heart failure due to chronic pulmonary disease.


JOHN RADCLIFFE HOSPITAL/SCIENCE PHOTO LIBRARY
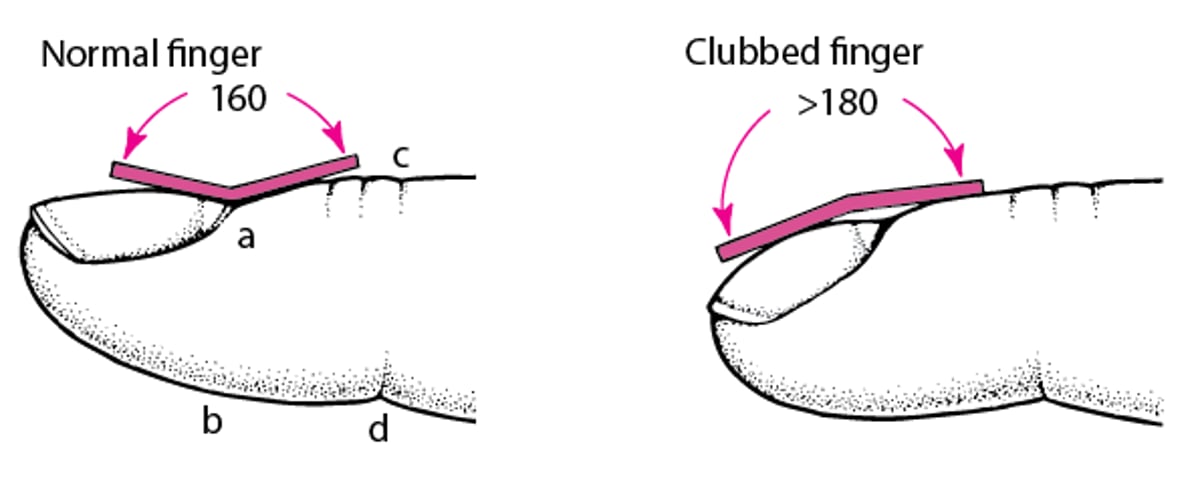
Clubbing is enlargement of the fingertips (or toes) due to proliferation of connective tissue between the fingernail and the bone. Diagnosis is based on an increase in the profile angle of the nail as it exits the finger (to >180°) or on an increase in the phalangeal depth ratio (to > 1—see figure Measuring finger clubbing). “Sponginess” of the nail bed beneath the cuticle also suggests clubbing.
Clubbing is most commonly observed in patients with lung cancer but is an important sign of chronic pulmonary disease, such as cystic fibrosis and idiopathic pulmonary fibrosis; it also occurs (but less commonly) in cyanotic heart disease, chronic infection (eg, infective endocarditis), stroke, inflammatory bowel disease, and cirrhosis. Clubbing occasionally occurs with osteoarthropathy and periostitis (primary or hereditary hypertrophic osteoarthropathy); in this instance, clubbing may be accompanied by skin changes, such as hypertrophied skin on the dorsa of the hands (pachydermoperiostosis), seborrhea, and coarse facial features. Digital clubbing can also occur as a benign hereditary abnormality that can be distinguished from pathologic clubbing by the absence of pulmonary symptoms or disease and by the presence of clubbing from an early age (by patient report).


© Springer Science+Business Media
Measuring Finger Clubbing
The ratio of the anteroposterior diameter of the finger at the nail bed (a–b) to that at the distal interphalangeal joint (c–d) is a simple measurement of finger clubbing. It can be obtained readily and reproducibly with calipers. If the ratio is > 1, clubbing is present. Finger clubbing is also characterized by loss of the normal angle at the nail bed. |

Barrel chest is the increased anterior-posterior diameter of the chest present in some patients with emphysema.


PNMB/SCIENCE PHOTO LIBRARY
In pursed lip breathing, the person inhales through the nose with the mouth closed and then slowly exhales through tightly puckered lips. This maneuver slows the rate of expiration and generates positive end expiratory pressure, which prevents airway collapse and prevents gas trapping.
Chest wall deformities, such as pectus excavatum (a sternal depression usually beginning over the manubrium or sternal body and progressing inward through the xiphoid process) and kyphoscoliosis, may restrict respirations and exacerbate symptoms of preexisting pulmonary disease. Pectus carinatum (also called pigeon chest) is another chest wall deformity that typically does not affect pulmonary function but may be associated with underlying connective tissue diseases such as Marfan syndrome. These abnormalities can usually be observed during careful examination after the patient's shirt is removed. Inspection should also include an assessment of the abdomen and the extent of obesity, ascites, or other conditions that could affect abdominal compliance.


DR P. MARAZZI / SCIENCE PHOTO LIBRARY
Abnormal breathing patterns may suggest underlying disease processes. A prolonged expiratory to inspiratory ratio occurs in obstructive lung disease. Some abnormal breathing patterns cause fluctuations in respiratory rate, so respiratory rate should be assessed and counted for 1 minute.
Cheyne-Stokes respiration (periodic breathing) is a cyclic fluctuation of respiratory rate and depth. From periods of brief apnea, patients breathe progressively faster and deeper (hyperpnea), then slower and shallower until they become apneic and repeat the cycle. Cheyne-Stokes respiration is most often caused by heart failure, a neurologic disorder (eg, stroke, advanced dementia), or medications. The pattern in heart failure has been attributed to delays in cerebral circulation; respiratory centers lag in recognition of systemic acidosis/hypoxia (causing hyperpnea) or alkalosis/hypocapnia (causing apnea).
Biot respiration is an uncommon variant of Cheyne-Stokes respiration in which irregular periods of apnea alternate with periods in which 4 or 5 deep, equal breaths are taken. It differs from Cheyne-Stokes respiration in that it is characterized by abrupt starts and stops and lacks periodicity. It results from injury to the central nervous system and occurs in such disorders as meningitis.
Kussmaul respirations are deep, regular respirations caused by metabolic acidosis.
Jugular venous pressure is evaluated with the patient reclining at 45°. The top of the venous column is normally just above the clavicles (upper limit of normal: 4 cm above the sternal notch in a vertical plane). An increase in the height of the column (or grossly distended jugular veins) corresponds to an increase in central venous pressure and may indicate right heart failure, left ventricular dysfunction, pulmonary hypertension, pericardial tamponade, constrictive pericarditis, or a combination. It should prompt a search for other signs of cardiac disorder (eg, third heart sound [S3] gallop, murmurs, dependent edema).
Percussion and palpation
Percussion is the primary physical maneuver used to detect the presence and level of pleural effusion. Finding areas of dullness during percussion signifies underlying fluid or, less commonly, consolidation.
Palpation includes tactile fremitus (vibration of the chest wall felt while a patient is speaking); it is decreased in pleural effusion and pneumothorax and increased in pulmonary consolidation (eg, lobar pneumonias). Point tenderness on palpation may signal underlying rib fracture, or costochondral dislocation or inflammation.
A right ventricular impulse at the left lower sternal border may become evident and may be increased in amplitude and duration (right ventricular heave) in patients with cor pulmonale.
Auscultation
Lung auscultation is arguably the most important component of the physical examination. All fields of the chest should be listened to, including the flanks and the anterior chest, to detect abnormalities associated with each lobe of the lung. Features to listen for include
Character and volume of breath sounds
Presence or absence of vocal sounds
Pleural friction rubs
Cardiac auscultation may reveal signs of pulmonary hypertension, such as a loud pulmonic second heart sound (P2), and of right heart failure, such as a right ventricular fourth heart sound (S4 gallop) and the murmur of tricuspid regurgitation.

The character and volume of breath sounds are useful in identifying pulmonary disorders. Vesicular breath sounds are the normal sounds heard over most lung fields. Bronchial breath sounds are slightly louder, harsher, and higher pitched; they normally can be heard over the trachea and over areas of lung consolidation, such as occur with pneumonia.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Audio file courtesy of David W. Cugell, MD.
Adventitious sounds are abnormal sounds, such as crackles, rhonchi, wheezes, and stridor.
Crackles (previously called rales) are discontinuous adventitious breath sounds. These sounds are most commonly heard during inspiration. Fine crackles are short, high-pitched sounds; coarse crackles are longer-lasting, low-pitched sounds. Crackles have been compared to the sound of crinkling plastic wrap or the opening of Velcro (in interstitial lung disease) and can be simulated by rubbing strands of hair together between 2 fingers near one’s ear. They occur most commonly with atelectasis, alveolar filling processes (eg, pulmonary edema), and interstitial lung disease (eg, pulmonary fibrosis); they signify opening of collapsed airways or alveoli.
Rhonchi are low-pitched respiratory sounds that can be heard during inspiration or expiration. They occur in various conditions, including chronic bronchitis. The mechanism may relate to variations in obstruction as airways distend with inhalation and narrow with exhalation.
Wheezes are whistling, musical breath sounds that are worse during expiration than inspiration and involve narrowing of small airways. Wheezing can be a physical finding or a symptom and is usually associated with dyspnea.
Stridor is a high-pitched, predominantly inspiratory sound formed by extrathoracic upper airway obstruction. It usually can be heard without a stethoscope. Stridor is usually louder than wheezing, is predominantly inspiratory, and is heard loudly over the larynx. It should trigger a concern for life-threatening upper airway obstruction. Stridor is more common in children since their airways are narrower. Stridor can less commonly be expiratory (occurring due to a narrowing in the thoracic trachea) or biphasic (occurring due to a narrowing in the cervical trachea or subglottis).
Decreased breath sounds signify poor air movement in airways, as occurs with asthma and COPD where bronchospasm or other mechanisms limit airflow. Breath sounds may also be decreased in the presence of a pleural effusion, pneumothorax, or an obstructing endobronchial lesion.
Squeaks are high-pitched, musical lung sounds during the late inspiratory phase of breathing, heard in conditions such as interstitial lung disease, pneumonia, and some small airway disease.
Vocal sounds are heard during auscultation while patients vocalize.
Bronchophony and whispered pectoriloquy occur when the patient’s spoken or whispered voice is clearly transmitted through the chest wall. Voice transmission results from alveolar consolidation, as occurs with pneumonia.
Egophony (E to A change) is said to occur when, during auscultation, a patient says the letter “E” and the examiner hears the letter “A,” as occurs with alveolar consolidation in pneumonia or at the upper border of a pleural effusion. (This vowel change is specific to the English language.)
Friction rubs are grating or creaking sounds that fluctuate with the respiratory cycle and sound like the creak of leather shoes, or a boot crunching against fresh snow. They are a sign of pleural inflammation and are heard in patients with pleuritis or empyema and after thoracotomy.
Inspiratory to expiratory (I:E) ratio is normally 1:2 but is prolonged to ≥ 1:3 when airflow is limited, such as in asthma and COPD, even in the absence of wheezing.



