



- Emergency Treatment of Arrhythmias
- Atrial Fibrillation
- Atrial Fibrillation and Wolff-Parkinson-White Syndrome (WPW Syndrome)
- Atrial Flutter
- Atrioventricular Block
- Bundle Branch Block and Fascicular Block
- Ectopic Supraventricular Arrhythmias
- Reentrant (Paroxysmal) Supraventricular Tachycardias (PSVT)
- Sick Sinus Syndrome
- Syndrome of Inappropriate Sinus Tachycardia
- Torsades de Pointes Ventricular Tachycardia
- Ventricular Fibrillation (VF)
- Ventricular Premature Beats (VPB)
- Ventricular Tachycardia (VT)
- Wolff-Parkinson-White Syndrome (WPW Syndrome)
Topic Resources

")
(See also Overview of Arrhythmias.)
Ventricular premature beats (VPBs), also called premature ventricular contractions (PVC), may occur erratically or at predictable intervals (eg, every third [trigeminy] or second [bigeminy] beat). VPBs may increase with stimulants (eg, anxiety, stress, alcohol, caffeine, sympathomimetic drugs or medications), hypoxia, or electrolyte abnormalities. Although VPBs are typically benign, they may be a manifestation of a structural heart disorder. An increase in premature ventricular beat frequency or complexity with exercise may indicate reversible myocardial ischemia. Patients with very frequent VPBs may develop reversible VPB-induced cardiomyopathy, particularly if there is an underlying cardiomyopathy (1).
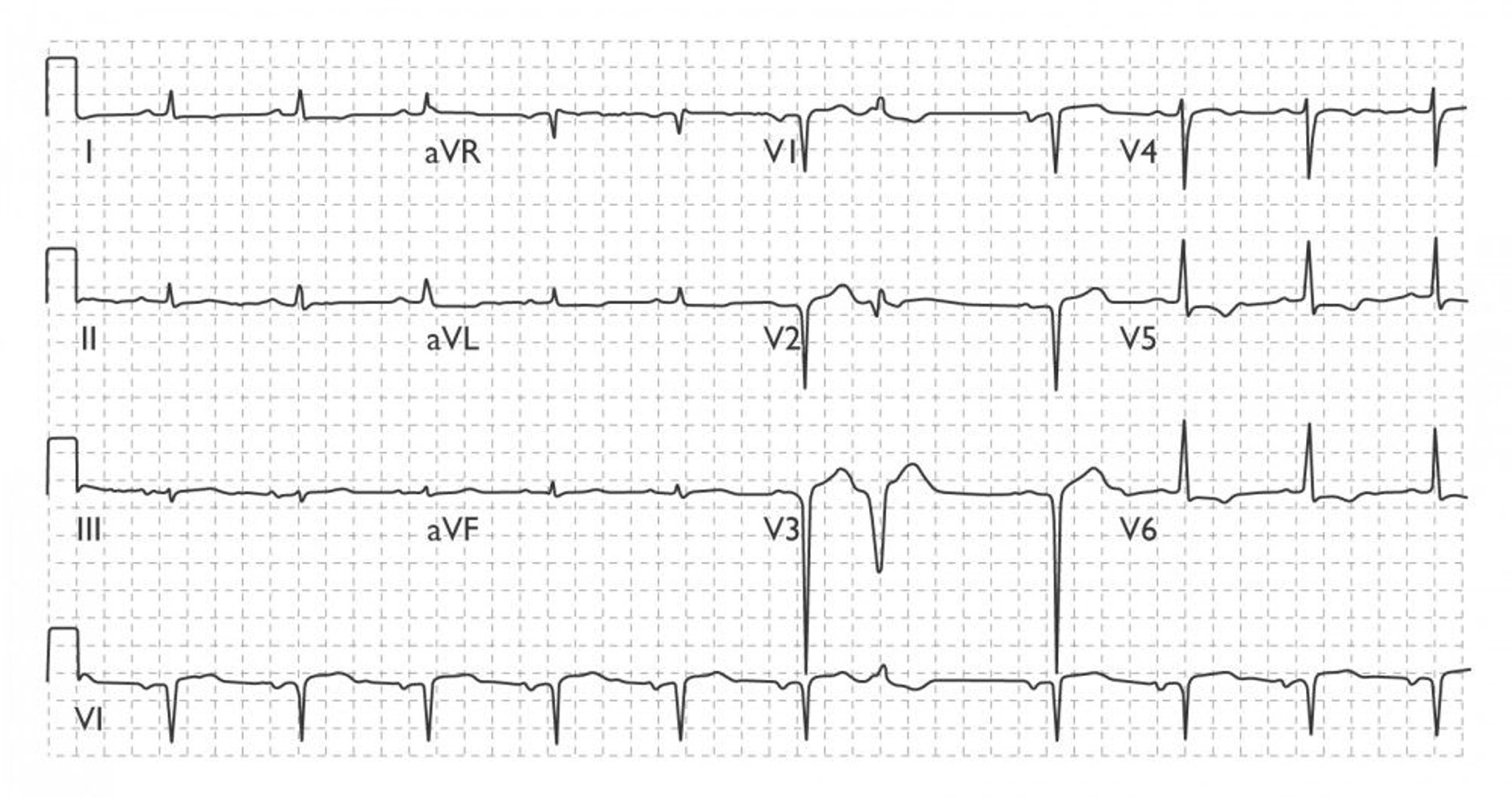
Some people with a structurally normal heart have VPBs due to cAMP-mediated delayed after depolarizations. Recognizing their usual sites of origin, these idiopathic VPBs are termed right ventricular outflow tract VPBs or left-ventricular outflow tract VBPs (2). They typically have a morphology similar to that of left bundle branch block and a vertical downward axis (positive QRS in lead V1, negative QRS in lead AVL, and near-isoelectric QRS in lead I) (see figure Sinus Rhythm With Ventricular Premature Beats Due to Right Ventricular Outflow Tract Ectopy).
VPBs may be experienced as missed or skipped beats; the VPB itself is not sensed but rather the following augmented sinus beat. When VPBs are very frequent, particularly when they occur at every second heart beat, mild hemodynamic symptoms are possible because the sinus rate has been effectively halved. Existing ejection murmurs may be accentuated because of increased cardiac filling and augmented contractility after the compensatory pause.
General references
1. Latchamsetty R, Bogun F: Premature Ventricular Complex-Induced Cardiomyopathy. JACC Clin Electrophysiol 5(5):537–550, 2019. doi: 10.1016/j.jacep.2019.03.013
2. Lerman BB: Mechanism, diagnosis, and treatment of outflow tract tachycardia. Nat Rev Cardiol 12(10):597–608, 2015. doi: 10.1038/nrcardio.2015.121
Diagnosis of Ventricular Premature Beats
ECG
Sometimes 24-hour ambulatory monitoring and echocardiography
Diagnosis of ventricular premature beats is by electrocardiography (ECG) showing a wide QRS complex without a preceding P wave, typically followed by a fully compensatory pause. Patients whose history (including family history), physical examination, or ECG suggest a possible underlying structural heart disorder should have 24-hour ambulatory monitoring and echocardiography (1). If ischemic heart disease is suspected, an exercise test is done for diagnostic purposes and to determine the need for further testing to evaluate the severity of coronary artery disease and the potential for coronary revascularization (1).

© Springer Science+Business Media

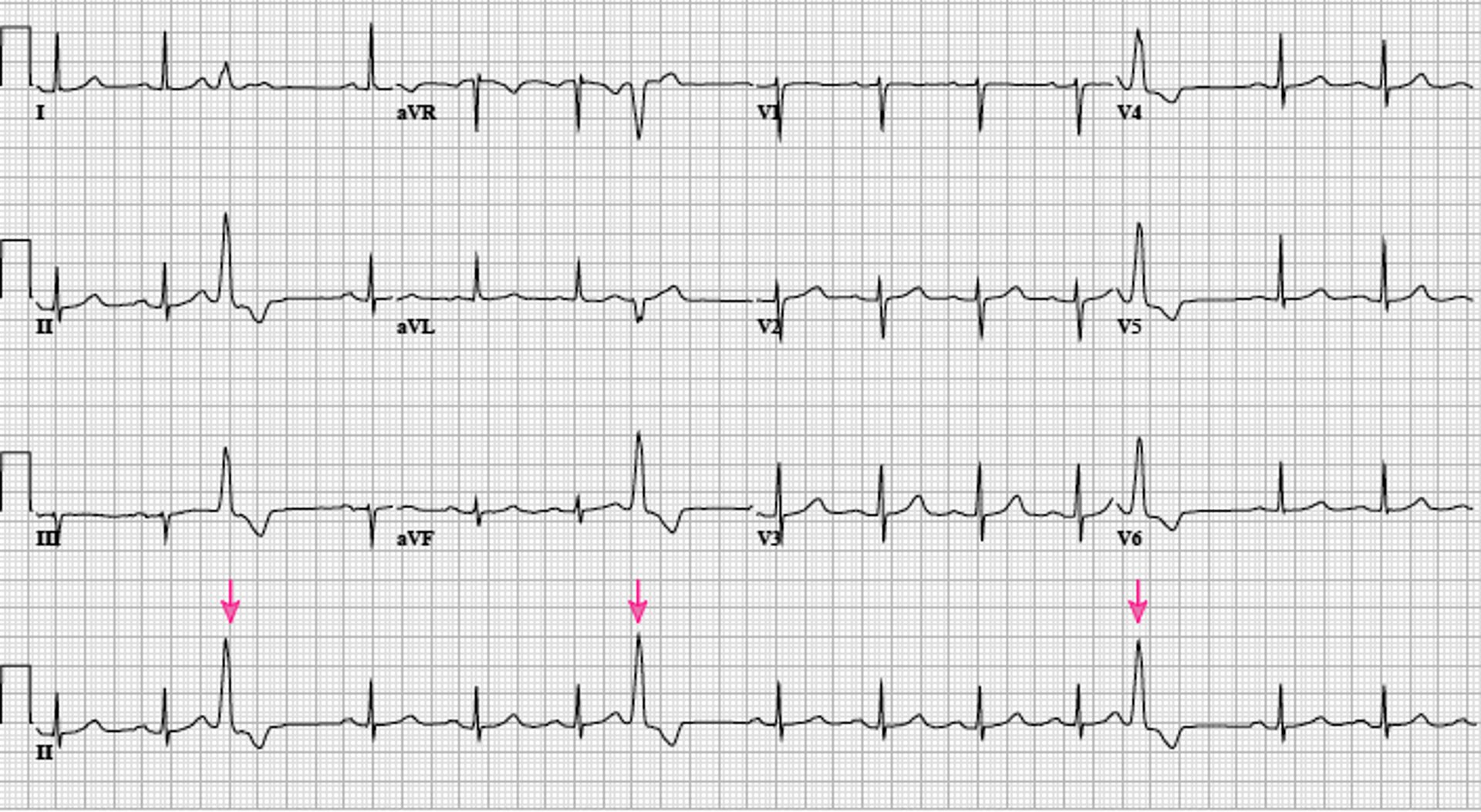
Image courtesy of L. Brent Mitchell, MD.
Diagnosis reference
1. Pedersen CT, Kay GN, Kalman J, et al: EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm 11(10):e166–e196, 2014. doi: 10.1016/j.hrthm.2014.07.024
Treatment of Ventricular Premature Beats
Beta-blockers or non-dihydropyridine calcium antagonists for patients with bothersome symptoms
Rarely, a class I or class III antiarrhythmic medication
Rarely, ablation
In the absence of a structural heart disorder, asymptomatic or mildly symptomatic premature VPBs have a benign prognosis and require no treatment other than reassurance (1). Treatment for VPBs is only required for relief from bothersome symptoms.
Treatment begins with beta-blockers or non-dihydropyridine calcium antagonists (verapamil or diltiazem). These medications are particularly effective in patients with right or left ventricular outflow tract VPBs (Treatment begins with beta-blockers or non-dihydropyridine calcium antagonists (verapamil or diltiazem). These medications are particularly effective in patients with right or left ventricular outflow tract VPBs (1). Class I or class III antiarrhythmic medications may increase risk of mortality and are not commonly used in patients with a structural heart disorder. To help prevent and/or reverse VPB-induced cardiomyopathy, patients with medication-resistant VPBs and progressive ventricular systolic dysfunction are treated with transcatheter ablation (2). Ablation may also be offered if symptoms are intolerable (1). Ablation is particularly effective in patients with right or left ventricular outflow VPBs (1).
In patients with a structural heart disorder, frequent VPBs (> 10/minute) correlate with increased mortality. Nevertheless, no studies have shown that pharmacologic suppression reduces mortality.
Patients in the post-myocardial infarction period have a higher mortality rate when treated with class I antiarrhythmics than with placebo (3). This finding probably reflects adverse effects of the antiarrhythmics. Beta-blockers (class II antiarrhythmics) should be used if indicated as part of guideline-directed therapy for the underlying structural heart disease. They are beneficial in symptomatic heart failure or if required for relief of symptoms resulting from VPBs. Non-dihydropyridine calcium antagonists (verapamil, diltiazem) should not be used in patients with significantly reduced left ventricular systolic function. If VPBs increase during exercise in a patient with ) should be used if indicated as part of guideline-directed therapy for the underlying structural heart disease. They are beneficial in symptomatic heart failure or if required for relief of symptoms resulting from VPBs. Non-dihydropyridine calcium antagonists (verapamil, diltiazem) should not be used in patients with significantly reduced left ventricular systolic function. If VPBs increase during exercise in a patient withcoronary artery disease, evaluation for percutaneous transluminal coronary angioplasty or coronary artery bypass graft surgery should be considered (1).
Treatment references
1. Pedersen CT, Kay GN, Kalman J, et al: EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm 11(10):e166–e196, 2014. doi: 10.1016/j.hrthm.2014.07.024
2. Latchamsetty R, Bogun F: Premature Ventricular Complex-Induced Cardiomyopathy. JACC Clin Electrophysiol 5(5):537–550, 2019. doi: 10.1016/j.jacep.2019.03.013
3. Echt DS, Liebson PR, Mitchell LB, et al: Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. N Engl J Med 324(12):781–788, 1991. doi: 10.1056/NEJM199103213241201
Prognosis for Ventricular Premature Beats
VPBs are not significant in patients without a heart disorder, and no treatment is required beyond avoiding obvious triggers. Therapy is offered only if symptoms are intolerable or if the VPBs are very frequent and, by inducing interventricular dyssynchrony, induce cardiomyopathy with heart failure. Other antiarrhythmics that suppress VPBs increase risk of more serious arrhythmias.
Drugs Mentioned In This Article






