



- Overview of Glomerular Disorders
- Overview of Nephritic Syndrome
- Alport Syndrome
- Immunoglobulin A Nephropathy
- Postinfectious Glomerulonephritis (PIGN)
- Rapidly Progressive Glomerulonephritis (RPGN)
- Thin Basement Membrane Disease
- Overview of Nephrotic Syndrome
- Congenital Nephrotic Syndromes
- Diabetic Nephropathy
- Focal Segmental Glomerulosclerosis
- HIV-Associated Nephropathy
- Membranous Nephropathy
- Minimal Change Disease
- Fibrillary and Immunotactoid Glomerulopathies
- Lupus Nephritis
- Membranoproliferative Glomerulonephritis
Topic Resources
")
")
HIV-associated nephropathy, a type of nephrotic syndrome, seems to be more common among patients of African ancestry with human immunodeficiency virus (HIV) infection who are inject drugs or have been poorly adherent to their antiretroviral therapy regimen. This increased risk may be related in part to genetic variants in the APOL1 gene (1). Infection of renal cells with HIV may contribute.
Most clinical findings are similar to those of focal segmental glomerulosclerosis, but hypertension is less common and the kidneys remain enlarged.
Most patients experience rapid progression to kidney failure within 1 to 4 months.
General reference
1. Neves PD, Watanabe A, Watanabe EH, et al. Idiopathic collapsing glomerulopathy is associated with APOL1 high-risk genotypes or Mendelian variants in most affected individuals in a highly admixed population. Kidney Int 2024;105(3):593-607. doi:10.1016/j.kint.2023.11.028
Diagnosis of HIV-Associated Nephropathy
Renal biopsy
HIV-associated nephropathy is suspected in patients with nephrotic syndrome or nephropathy who have severe HIV infection. HIV-associated nephropathy should be distinguished from the many other disorders that occur with higher frequency in HIV-infected patients and cause kidney disease, such as thrombotic microangiopathy (hemolytic-uremic syndrome and thrombotic thrombocytopenic purpura), immune complex–mediated glomerulonephritis, and drug-induced interstitial nephritis (due to indinavir and ritonavir) and ), immune complex–mediated glomerulonephritis, and drug-induced interstitial nephritis (due to indinavir and ritonavir) andrhabdomyolysis (due to statins).
Ultrasound, if performed, shows that the kidneys are enlarged and highly echogenic.
Renal biopsy typically is performed. Light microscopy shows capillary collapse of varying severity (collapsing glomerulopathy) and differing degrees of increased mesangial matrix. Tubular cells show marked degenerative changes and tubular atrophy or microcytic dilation. Interstitial immune cell infiltrate, fibrosis, and edema are common. Tubular reticular inclusions, similar to those in systemic lupus erythematosus, are found within endothelial cells but are rare with effective HIV therapy.

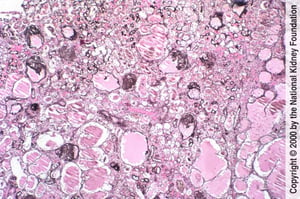
Focal segmental glomerulosclerosis with collapse of glomerular tufts and microcystic tubular changes is characteristic of HIV-associated nephropathy (Jones silver stain, ×100).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
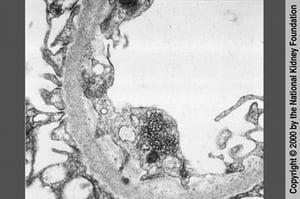
HIV-associated nephropathy can be distinguished from focal segmental glomerulosclerosis by reticular inclusions in endothelial cell cytoplasm on transmission electron microscopy (×20,000). However, these reticular inclusions are now rare with use of highly active antiretroviral therapy.
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Focal segmental glomerulosclerosis with collapse of glomerular tufts and microcystic tubular changes is characteristic of HIV-associated nephropathy (Jones silver stain, ×100).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
HIV-associated nephropathy can be distinguished from focal segmental glomerulosclerosis by reticular inclusions in endothelial cell cytoplasm on transmission electron microscopy (×20,000). However, these reticular inclusions are now rare with use of highly active antiretroviral therapy.
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Normotension and persistently enlarged kidneys help to differentiate HIV-associated nephropathy from focal segmental glomerulosclerosis.
Treatment of HIV-Associated Nephropathy
Antiretroviral therapy (ART) and angiotensin inhibition
Control of the HIV infection may help minimize kidney damage; in fact, HIV-associated nephropathy is rare in patients taking ART with well-controlled HIV infection. The role of corticosteroids is not well defined (1). Angiotensin inhibition with angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) is probably of some benefit. At some centers, kidney transplantation is performed.
Treatment reference
1. Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int 100(4S):S1-S276, 2021. doi:10.1016/j.kint.2021.05.021
Drugs Mentioned In This Article






