


- Overview of Glomerular Disorders
- Overview of Nephritic Syndrome
- Alport Syndrome
- Immunoglobulin A Nephropathy
- Postinfectious Glomerulonephritis (PIGN)
- Rapidly Progressive Glomerulonephritis (RPGN)
- Thin Basement Membrane Disease
- Overview of Nephrotic Syndrome
- Congenital Nephrotic Syndromes
- Diabetic Nephropathy
- Focal Segmental Glomerulosclerosis
- HIV-Associated Nephropathy
- Membranous Nephropathy
- Minimal Change Disease
- Fibrillary and Immunotactoid Glomerulopathies
- Lupus Nephritis
- Membranoproliferative Glomerulonephritis
")

The hallmark of glomerular disorders is proteinuria, which is often in the nephrotic range (≥ 3 g/day).
Glomerular disorders are classified based on urine changes as those that manifest predominantly with:
Nephrotic-range proteinuria and nephrotic urine sediment (fatty casts, oval fat bodies, but few cells or cellular casts)
Hematuria, usually in combination with proteinuria (which may be in the nephrotic range); the red blood cells (RBCs) are usually dysmorphic and often there are RBC or mixed cellular casts (nephritic urine sediment)
Nephrotic syndrome is nephrotic urine sediment plus edema and hypoalbuminemia (typically with hypercholesterolemia and hypertriglyceridemia).
Nephritic syndrome is nephritic urine sediment with or without hypertension, elevated serum creatinine, and oliguria.
Several glomerular disorders typically manifest with features of both nephritic and nephrotic syndromes. These disorders include, but are not limited to, fibrillary and immunotactoid glomerulopathies, membranoproliferative glomerulonephritis (GN), and lupus nephritis.


DENNIS KUNKEL MICROSCOPY/SCIENCE PHOTO LIBRARY
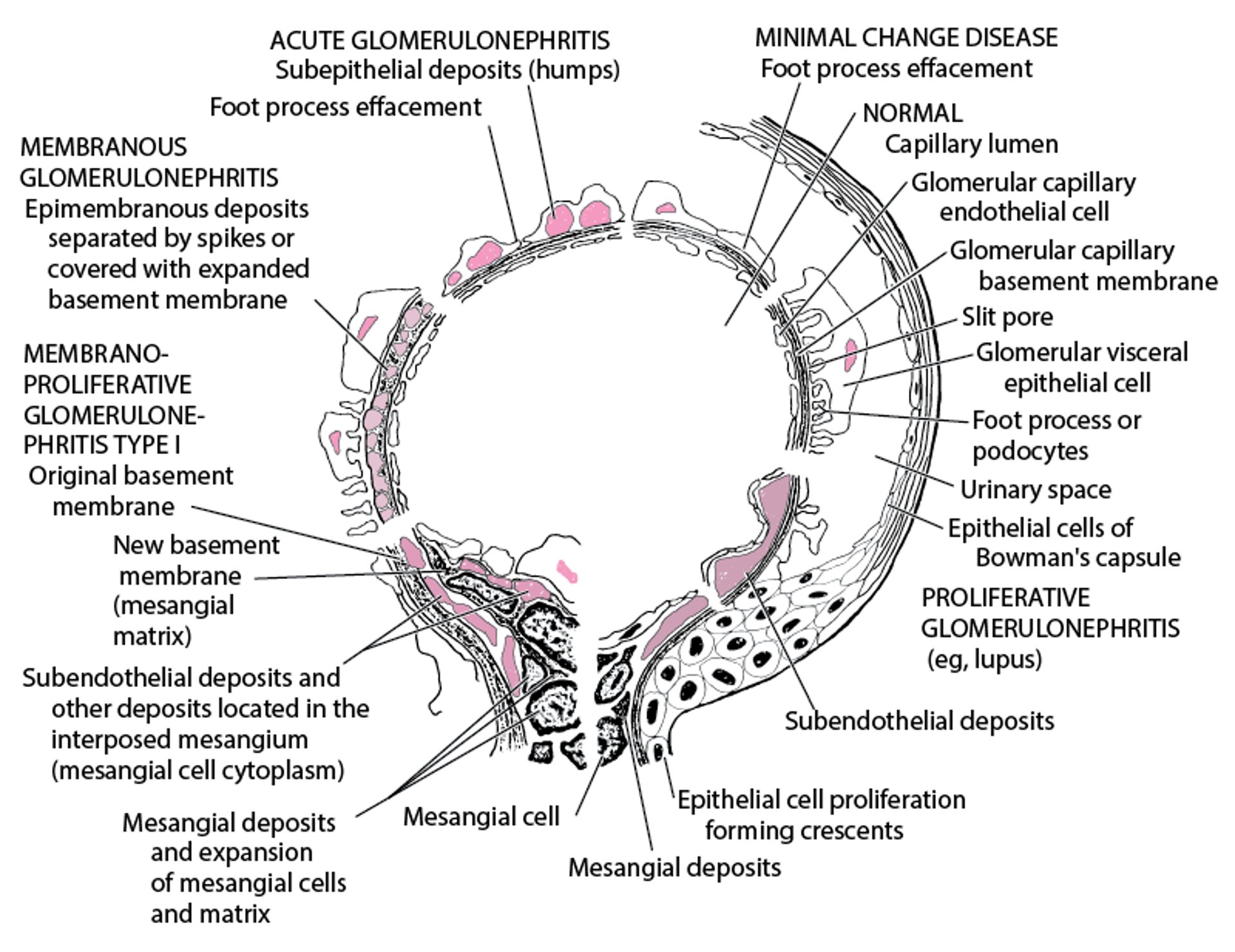
The pathophysiology of nephritic and nephrotic disorders differs substantially (see figure Electron Microscopic Features in Immunologic Glomerular Disorders), but their clinical overlap is considerable—eg, several disorders may manifest with the same clinical picture—and the presence of hematuria or proteinuria does not itself predict response to treatment or prognosis.
Disorders tend to manifest at different ages (see table Glomerular Disorders by Age and Manifestations), although there is much overlap. The disorders may be:
Primary (idiopathic)
Secondary (see tables Causes of Glomerulonephritis and Causes of Nephrotic Syndrome)
Glomerular Disorders by Age and Manifestations
Age (years) | Nephritic Syndrome | Nephrotic Syndrome | Mixed Nephritic and Nephrotic Syndrome |
|---|---|---|---|
< 15 | Alport syndrome (hereditary nephritis) Mild PIGN | Congenital nephrotic syndromes Focal segmental glomerulosclerosis Lupus nephritis (membranous subtype) | |
15–40 | Focal segmental glomerulosclerosis Lupus nephritis (membranous subtype) | ||
> 40 | Focal segmental glomerulosclerosis Late PIGN | ||
* More commonly manifests as nephrotic syndrome. | |||
GN = glomerulonephritis; IgA = immunoglobulin A; PIGN = postinfectious glomerulonephritis; RPGN = rapidly progressive glomerulonephritis. | |||
Adapted from Rose BD: Pathophysiology of Renal Disease, ed. 2. New York, McGraw-Hill, 1987, p. 167. | |||
Electron Microscopic Features in Immunologic Glomerular Disorders



CHOKSAWATDIKORN / SCIENCE PHOTO LIBRARY
Diagnosis of Glomerular Disorders
Serum creatinine level and urinalysis
A glomerular disorder is usually suspected when screening or diagnostic testing reveals an elevated serum creatinine level and abnormal urinalysis (hematuria with or without casts, proteinuria, or both). Approach to the patient involves distinguishing predominant-nephritic from predominant-nephrotic features and identifying likely causes by patient age, accompanying illness (see table Glomerular Disorders by Age and Presentation and table Causes of Nephrotic Syndrome), and other elements of the history (eg, time course, systemic manifestations, family history).
Renal biopsy is indicated when diagnosis is unclear from history or when histology influences choice of treatment and outcomes (eg, lupus nephritis).







