



- Angiostrongyliasis
- Anisakiasis
- Ascariasis
- Baylisascariasis
- Dracunculiasis
- Hookworm Infection
- Pinworm Infestation
- Strongyloidiasis
- Toxocariasis
- Trichinosis
- Trichuriasis
- Overview of Filarial Nematode Infections
- Bancroftian Lymphatic Filariasis and Brugian Lymphatic Filariasis
- Dirofilariasis
- Loiasis
- Mansonellosis
- Onchocerciasis (River Blindness)
Ancylostomiasis is infection with the hookworm (a type of nematode) Ancylostoma duodenale or Necator americanus. Symptoms include rash at the site of larval entry and sometimes abdominal pain or other gastrointestinal symptoms during early infection. Later, iron deficiency may develop because of chronic blood loss. Hookworms are a major cause of iron deficiency anemia in endemic regions. Diagnosis is by finding eggs in stool. Treatment is with albendazole, mebendazole, or pyrantel pamoate.. Symptoms include rash at the site of larval entry and sometimes abdominal pain or other gastrointestinal symptoms during early infection. Later, iron deficiency may develop because of chronic blood loss. Hookworms are a major cause of iron deficiency anemia in endemic regions. Diagnosis is by finding eggs in stool. Treatment is with albendazole, mebendazole, or pyrantel pamoate.

")
")
The worldwide prevalence of hookworm infection is estimated at 406 to 480 million (1, 2). Both Ancylostoma duodenale and Necator americanus occur in Africa, Asia, and the Americas. Only A. duodenale occurs in the Middle East, North Africa, and southern Europe. N. americanus predominates in the Americas and Australia; it was once widely distributed in the southern United States and is still present in areas in that region where there is unsanitary disposal of human waste. Hookworm remains endemic on islands of the Caribbean and in Central and South America. Some strains of Ancylostoma ceylanicum, a hookworm of dogs, cats, and hamsters, also mature to adulthood in the human intestine. Infections with A. ceylanicum have been reported in residents of parts of Asia and some South Pacific islands.
Hookworms cause significant morbidity, in part due to anemia, estimated at 400 million disability-adjusted life years in 2010 (3).
(See also Approach to Parasitic Infections.)
General references
1. Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743-800. doi:10.1016/S0140-6736(15)60692-4
2. Centers for Disease Control and Prevention (CDC): About Hookworm. Accessed October 18, 2024.
3. Bartsch SM, Hotez PJ, Asti L, et al. The Global Economic and Health Burden of Human Hookworm Infection. PLoS Negl Trop Dis. 2016;10(9):e0004922. Published 2016 Sep 8. doi:10.1371/journal.pntd.0004922
Pathophysiology of Hookworm Infection
The hookworm species that reach maturity in the human intestine have similar life cycles. Eggs passed in the stool hatch in 1 to 2 days (if they are deposited in a warm, moist place on loose soil) and release rhabditiform larvae, which molt once to become slender filariform larvae in 5 to 10 days. The larvae can survive 3 to 4 weeks if environmental conditions are favorable. Filariform larvae penetrate human skin when people walk barefoot on or otherwise come into direct contact with infested soil.
The larvae reach the lungs via blood vessels, penetrate into pulmonary alveoli, ascend the bronchial tree to the epiglottis, and are swallowed. The larvae develop into adults in the small intestine; there, they attach to the wall, feeding on blood. Adult worms may live ≥ 2 years.

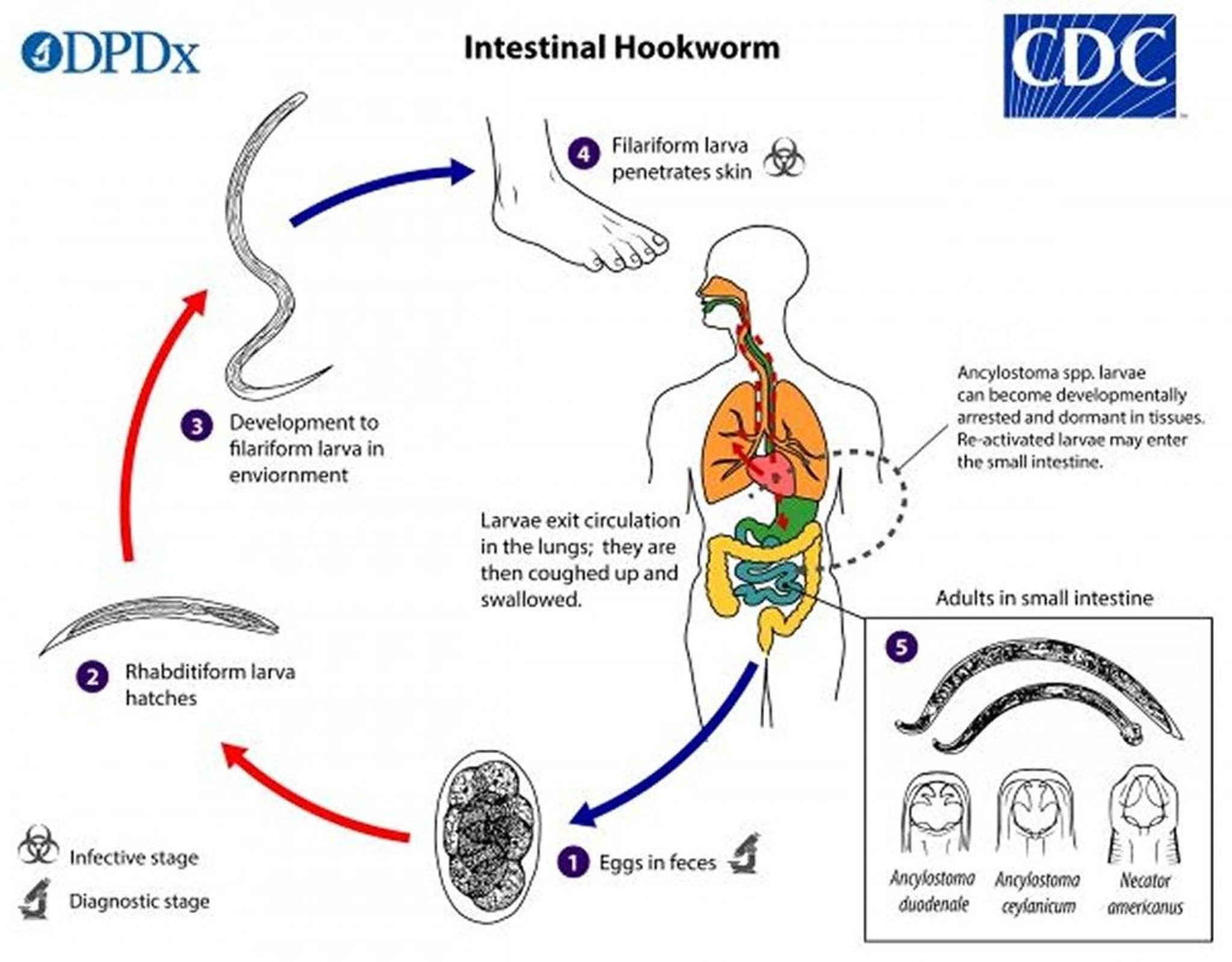
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Chronic blood loss leads to iron deficiency anemia. Development of anemia depends on worm burden and the amount of absorbable iron in the diet.
Zoonotic (animal) hookworm infections
Zoonotic hookworms infections include
Eosinophilic enterocolitis
Ancylostoma braziliense and Ancylostoma caninum are hookworms that have cats and dogs as the primary hosts. These hookworms cannot complete their life cycle in humans. If their larvae penetrate human skin, they typically wander in the skin, causing cutaneous larva migrans, rather than migrate to the intestine.
Rarely, A. caninum larvae migrate to the intestine, where they may cause eosinophilic enterocolitis. However, they do not cause significant blood loss and anemia, and because they do not mature to full adulthood, they do not lay eggs (making diagnosis difficult). Such intestinal infection may be asymptomatic or cause acute abdominal pain and eosinophilia.
(See also Hookworms in Small Animals.)
Symptoms and Signs of Hookworm Infection
Hookworm infection is often asymptomatic. However, a transient pruritic papulovesicular rash (ground itch) may develop at the site of larval penetration, usually on the feet.
Migration of large numbers of larvae through the lungs occasionally causes Löffler syndrome, with cough, wheezing, eosinophilia, and sometimes hemoptysis.
During the acute phase, adult worms in the intestine may cause colicky epigastric pain, anorexia, flatulence, diarrhea, and weight loss.


© Springer Science+Business Media


Photo courtesy of Karen McKoy, MD.
Chronic, heavy, intestinal infection can lead to iron deficiency anemia, causing pallor, dyspnea, weakness, tachycardia, lassitude, and peripheral edema. A low-grade eosinophilia is often present. In children, chronic blood loss may lead to severe anemia, heart failure, and anasarca and, in pregnant women, to growth retardation in the fetus.
Cutaneous larva migrans can occur when animal hookworms infect humans but do not reach adulthood. It is caused by larvae as they migrate through the skin and is characterized by itchy, erythematous, serpiginous skin lesions. On rare occasion, A. caninum larvae reach the human intestine where they cause eosinophilic enterocolitis with abdominal pain and associated symptoms. Eggs are not present in the stool.
Diagnosis of Hookworm Infection
Microscopic examination of stool
A. duodenale, A. ceylanicum, and N. americanus produce thin-shelled oval eggs that are readily detected in fresh stool. Concentration procedures are needed to diagnose light infections. If the stool is not kept cold and examined within several hours, the eggs may hatch and release larvae that must be differentiated from those of Strongyloides stercoralis. Although the 3 hookworm species that infect humans can be differentiated by molecular probes, the ova are indistinguishable, and a species-specific diagnosis is not made in clinical laboratories.
Eosinophilia is often present in people infected with hookworms. During the prepatent period of infection (ie, the 5 to 9 weeks between penetration of larvae and appearance of eggs in the stool), eosinophilia may be the only laboratory abnormality. Hookworm infestation is an important consideration in the differential diagnosis of eosinophilia in immigrants or travelers returning from endemic regions where sanitation is poor.
Nutritional status, anemia, and iron stores should be evaluated (see Diagnosis of Iron Deficiency Anemia).
Diagnosis of cutaneous larva migrans is based on the clinical manifestations. Ova are not present in the stool.
Treatment of Hookworm Infection
Anthelmintics
Intestinal hookworm infection
Intestinal hookworm infection is treated with anthelmintics. Albendazole, mebendazole, or pyrantel pamoate may be used.Intestinal hookworm infection is treated with anthelmintics. Albendazole, mebendazole, or pyrantel pamoate may be used.
Benzimidazoles should be avoided during pregnancy, but pyrantel pamoate is considered safe. Ivermectin, a common anthelmintic, is not effective for intestinal hookworm infection.
General support and correction of iron deficiency anemia are needed if infection is heavy.
Cutaneous larva migrans
Cutaneous larva migrans is a self-limited infection, but symptoms can last 5 to 6 weeks. Treatment with albendazole or ivermectin is curative.is a self-limited infection, but symptoms can last 5 to 6 weeks. Treatment with albendazole or ivermectin is curative.
Prevention of Hookworm Infection
Preventing unhygienic defecation and avoiding direct skin contact with the soil (eg, wearing shoes, using barriers when seated on the ground) are effective in preventing hookworm infection but difficult to implement in many endemic areas.
Periodic mass treatment of susceptible populations at 3- to 4-month intervals has been used in high-risk areas.
Risk of developing cutaneous larva migrans can be reduced by the following:
Avoiding direct skin contact with potentially infested sand or other soil where dogs or cats have defecated.
Key Points
Hookworm larvae penetrate the skin when people walk barefoot on or otherwise come into direct contact with infested soil.
In humans, larvae of the hookworms Ancylostoma duodenale and Necator americanus travel through the bloodstream to the lungs, penetrate the alveoli, ascend to the epiglottis, are swallowed, and then mature in the small intestine.
Infection may be asymptomatic, but a pruritic rash may appear at the site of larval penetration, and pulmonary involvement may cause cough and wheezing.
Intestinal involvement may cause iron deficiency anemia.
Diagnose by microscopic examination of stool.
Treat with albendazole, mebendazole, or pyrantel pamoate.Treat with albendazole, mebendazole, or pyrantel pamoate.







