



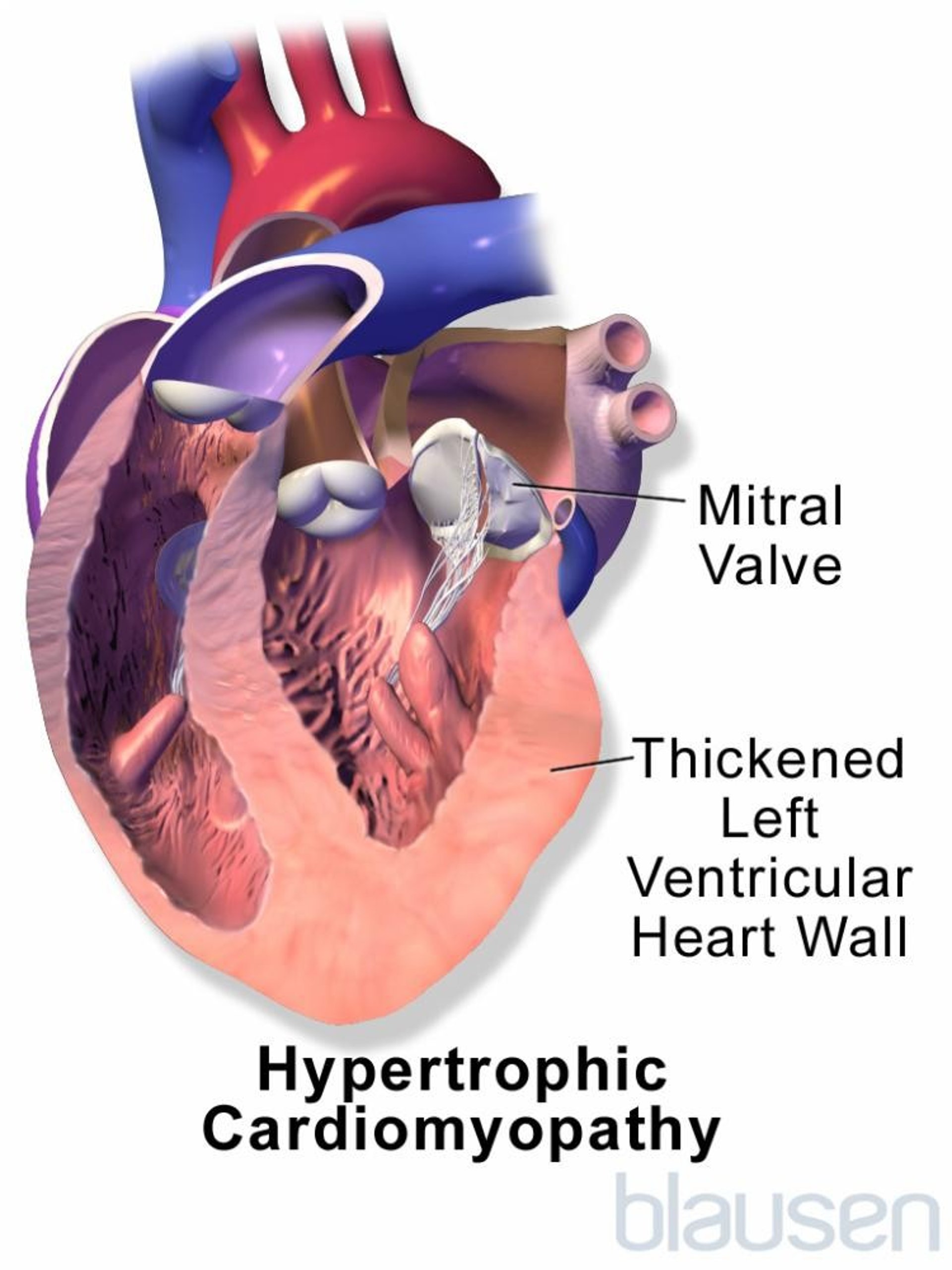
Hypertrophic cardiomyopathy includes a group of heart disorders in which the walls of the ventricles (the 2 lower chambers of the heart) thicken (hypertrophy) and become stiff.
Topic Resources


Most cases of hypertrophic cardiomyopathy are caused by an inherited genetic defect.
People experience fainting, chest pain, shortness of breath, and palpitations (awareness of irregular heartbeats).
Doctors suspect the diagnosis based on physical examination findings, but they use echocardiography or magnetic resonance imaging to confirm the diagnosis.
Medications that reduce the force of the heart’s contractions are given.


Cardiomyopathy refers to progressive impairment of the structure and function of the muscular walls of the heart chambers. There are three main types of cardiomyopathy. In addition to hypertrophic cardiomyopathy, there are dilated cardiomyopathy and restrictive cardiomyopathy (see also Overview of Cardiomyopathy).
The term cardiomyopathy is most often used when a disorder directly affects the heart muscle. Other disorders, such as high blood pressure and abnormal heart valves (such as aortic stenosis), also can eventually cause thickened heart muscle and heart failure.
Hypertrophic cardiomyopathy is a common cause of sudden death in young athletes. At least 1 in 500 people is affected.
Causes of Hypertrophic Cardiomyopathy
Hypertrophic cardiomyopathy is nearly always caused by a genetic defect. The defect may be a
Spontaneous genetic mutation
Inherited genetic defect
Very rarely, people acquire hypertrophic cardiomyopathy when they have disorders such as acromegaly (excessive growth due to overproduction of growth hormone, usually by a noncancerous tumor of the pituitary gland), a pheochromocytoma (a tumor that overproduces the hormone epinephrine), or neurofibromatosis (a genetic disorder in which many soft, fleshy growths of nerve tissue grow under the skin and in other parts of the body).

Complications
The thick, stiff walls of the ventricles do not relax appropriately to allow the heart chambers to fill with blood. This difficulty becomes more severe when the heart beats quickly (as during exercise) because there is then even less time for the heart to fill. Because the heart does not fill properly, it pumps less blood with each beat. Sometimes the thickened heart walls also interfere with blood flow out of the heart. This variation is called hypertrophic obstructive cardiomyopathy.
Because the ventricle walls thicken, the mitral valve (the valve that opens between the left atrium and the left ventricle) may be unable to close normally, resulting in leakage of blood back into the left atrium (mitral regurgitation). This valve leakage and the enlarged ventricular walls typically cause abnormal heart sounds (heart murmurs).
Abnormal heart rhythms can occur, which can cause sudden death.
Symptoms of Hypertrophic Cardiomyopathy
Symptoms are highly variable, but when they occur, they usually develop when people are between ages 20 and 40 years. Symptoms first occur during exercise and include
Fainting (syncope)
Chest pain
Shortness of breath
Sensation of irregular heartbeats (palpitations)
Fainting usually occurs suddenly without any warning symptoms. Fainting or even sudden death may be the first sign that a person has this condition.
Diagnosis of Hypertrophic Cardiomyopathy
Echocardiography and/or magnetic resonance imaging (MRI) of the heart
Doctors usually suspect the diagnosis of hypertrophic cardiomyopathy based on the person's symptoms and the results of a physical examination, electrocardiography (ECG), and a chest x-ray. The heart sounds and any murmurs heard through a stethoscope may be helpful. Although ECG and echocardiography are not recommended for all young competitive athletes, all such athletes should be evaluated for risk factors that indicate the need for further testing.
Echocardiography is the best way to confirm the diagnosis, but MRI of the heart may also be used because it may provide more detailed information.
Cardiac catheterization, an invasive procedure in which a catheter is threaded from a blood vessel in the arm, neck, or leg into the heart, is often done to measure pressures in the heart chambers and the degree to which blood flow from the left ventricle is blocked due to the thickened walls.
Because hypertrophic cardiomyopathy is usually caused by a gene mutation, genetic testing may also be done to help identify affected relatives.
Treatment of Hypertrophic Cardiomyopathy
Medications such as a beta-blocker and/or a calcium channel blocker
Sometimes a procedure to improve blood flow
Sometimes an implantable cardioverter-defibrillator
If possible, doctors treat the condition causing hypertrophic cardiomyopathy.
Treatment of hypertrophic cardiomyopathy is aimed primarily at reducing the heart’s resistance to filling with blood between heartbeats.
Medications for hypertrophic cardiomyopathy
Beta-blockers and the calcium channel blocker verapamil—taken separately or together—are the main treatment. Both reduce the force of heart muscle contraction. As a result, the heart can fill better and, if the thickened muscle was blocking blood flow, blood can flow out of the heart more easily. Also, beta-blockers and Beta-blockers and the calcium channel blocker verapamil—taken separately or together—are the main treatment. Both reduce the force of heart muscle contraction. As a result, the heart can fill better and, if the thickened muscle was blocking blood flow, blood can flow out of the heart more easily. Also, beta-blockers andverapamil slow the heart rate, so that the heart has more time to fill. Sometimes, disopyramide, a medication that decreases the strength of heart contractions, is also used. slow the heart rate, so that the heart has more time to fill. Sometimes, disopyramide, a medication that decreases the strength of heart contractions, is also used.
Amiodarone is sometimes used to treat abnormal heart rhythms.Amiodarone is sometimes used to treat abnormal heart rhythms.
Mavacamten decreases the contraction of the heart and seems to relieve symptoms and increase exercise tolerance.Mavacamten decreases the contraction of the heart and seems to relieve symptoms and increase exercise tolerance.
Myectomy
Surgery to remove some of the thickened heart muscle (myectomy) can improve the flow of blood from the heart, but surgery is done only when symptoms are incapacitating despite medication. Myectomy can relieve symptoms, but it does not reduce the risk of death. When myectomy is done in hospitals that have extensive experience doing the procedure, long-term results are excellent.
Alcohol ablation
Alcohol ablation (controlled destruction of a small area of heart muscle by injecting it with alcohol) is used in certain people to improve blood flow from the heart because it can be done during cardiac catheterization. Although cardiac catheterization is an invasive procedure in which a catheter is threaded into the heart, it has fewer risks in people who are at high risk of complications if they have heart surgery.
Implantable cardioverter-defibrillator
People who have severe heart muscle thickening, especially thickening of the wall that separates the heart chambers (cardiac septum), have a high risk of developing deadly abnormal heart rhythms which cause sudden death. Doctors may recommend an implantable cardioverter-defibrillator for these people.
Prognosis for Hypertrophic Cardiomyopathy
About 1% of adults with hypertrophic cardiomyopathy die each year. Children with hypertrophic cardiomyopathy are more likely to die than adults.
Other factors that suggest a greater risk of death include the following:
Family history of sudden death, particularly premature sudden death
Unexplained fainting
Occurrence of rapid and certain abnormal heart rhythms
Cardiac arrest
Severity of thickening in the heart muscle
Severe inability of the heart to pump enough blood
Characteristic MRI appearance
Death is usually sudden, presumably due to an abnormal heart rhythm. Death due to chronic heart failure is less common.
People who learn that they have inherited this disorder should have genetic counseling when they plan a family because they have a 50% chance of passing this disorder on to their offspring. First-degree family members (siblings or children) of people who have this inherited disorder should have their heart evaluated (with either genetic testing and/or routine echocardiography).
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
American Heart Association: Hypertrophic cardiomyopathy: Provides comprehensive information on symptoms, diagnosis, and treatment of hypertrophic cardiomyopathy







