



- Emergency Treatment of Arrhythmias
- Atrial Fibrillation
- Atrial Fibrillation and Wolff-Parkinson-White Syndrome (WPW Syndrome)
- Atrial Flutter
- Atrioventricular Block
- Bundle Branch Block and Fascicular Block
- Ectopic Supraventricular Arrhythmias
- Reentrant (Paroxysmal) Supraventricular Tachycardias (PSVT)
- Sick Sinus Syndrome
- Syndrome of Inappropriate Sinus Tachycardia
- Torsades de Pointes Ventricular Tachycardia
- Ventricular Fibrillation (VF)
- Ventricular Premature Beats (VPB)
- Ventricular Tachycardia (VT)
- Wolff-Parkinson-White Syndrome (WPW Syndrome)
Various rhythms result from supraventricular foci (usually in the atria). Diagnosis is by electrocardiography. Many are asymptomatic and require no treatment.
")
")

(See also Overview of Arrhythmias.)
Ectopic supraventricular rhythms include
Atrial premature beats
Atrial tachycardia
Multifocal atrial tachycardia
Nonparoxysmal junctional tachycardia
Wandering atrial pacemaker
Atrial premature beats
Atrial premature beats (APB), or premature atrial contractions (PAC), are common episodic impulses. They may occur in normal hearts with or without precipitating factors (eg, caffeine, alcohol, pseudoephedrine) or may be a sign of a cardiopulmonary disorder. They are common in patients with chronic obstructive pulmonary disease (COPD). They occasionally cause palpitations.
Diagnosis is by electrocardiography (ECG—see figure Atrial Premature Beat).
Atrial Premature Beat (APB)
In lead II, after the second beat of sinus origin, the T wave is deformed by an APB. Because the APB occurs relatively early during the sinus cycle, the sinus node pacemaker is reset, and a pause—less than fully compensatory—precedes the next sinus beat. |



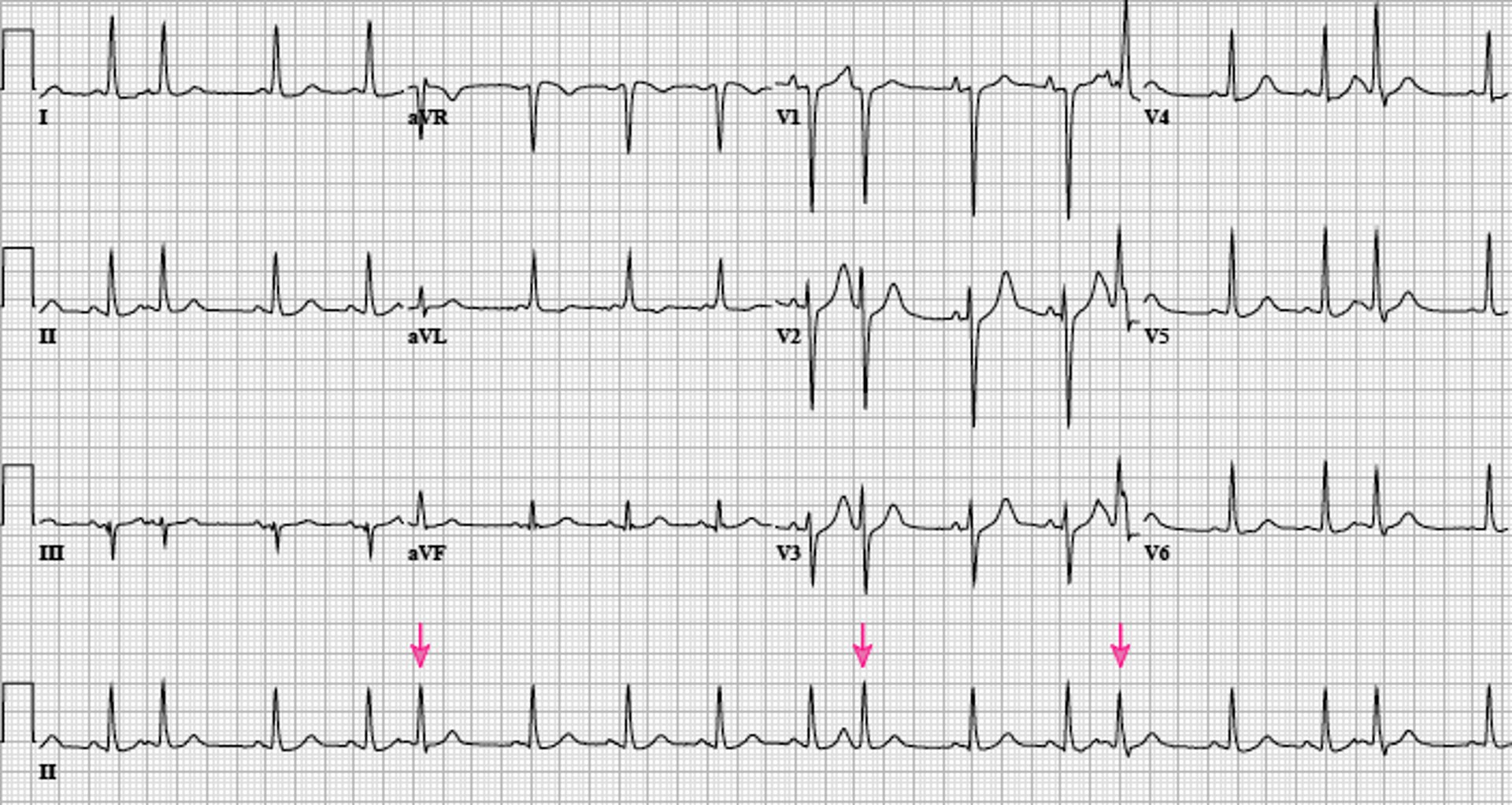
Image courtesy of L. Brent Mitchell, MD.
APBs may be normally, aberrantly, or not conducted and are usually followed by a noncompensatory pause (1). Aberrantly conducted APBs (usually with right bundle branch block morphology) must be distinguished from premature beats of ventricular origin.
Occasional APBs in apparently healthy people are generally considered benign, and nearly everyone has some. Frequent APBs have been shown to be associated with an increased risk of stroke, of all-cause mortality, of cardiovascular mortality, and atrial fibrillation (2, 3). It is not known if these associations are the consequence of APBs, of unidentified structural heart disorders, of unidentified atrial fibrillation, or simply that they all share the same risk factors (such as aging).
Atrial escape beats are ectopic atrial beats that emerge after long sinus pauses or sinus arrest. They may be single or multiple; escape beats from a single focus may produce a continuous rhythm (called ectopic or escape atrial rhythm). Heart rate is typically 40 to 60 beats/minute, P wave morphology is typically different, and PR interval is slightly shorter than in sinus rhythm. Accelerated atrial rhythm (also called a nonsinus atrial rhythm) may occur at a rate higher than the sinus rate due to either enhanced normal automaticity or abnormal automaticity. Accelerated atrial rhythm is distinguished from atrial tachycardia by being slower with an arbitrary rate cut-off (usually 100 or 120 beats/minute).
Junctional escape beats are ectopic beats that emerge after long sinus pauses or sinus arrest when not terminated by an atrial escape beat. The "junction" includes the atrioventricular (AV) node, His bundle, and adjacent atrial tissue that produce escape beats that cannot be more specifically localized by the ECG. They may be single or multiple; escape beats from a single junctional focus may produce a continuous rhythm (called ectopic or escape junctional rhythm). Heart rate is typically slow (35 to 50 beats/minute), P wave morphology typically shows low to high atrial activation (negative P waves in leads II, III, aVF), and P waves are located immediately before (< 0.1 second), during (thus hidden), or immediately after (< 0.1 second) the QRS complex.
Focal atrial tachycardia
Focal atrial tachycardia is a regular rhythm caused by consistent, rapid atrial activation from a single atrial focus. Heart rate is usually 150 to 200 beats/minute; however, with a very rapid atrial rate, nodal dysfunction, and/or digitalis toxicity, AV block may be present, and ventricular rate may be slower. Mechanisms include abnormal automaticity, triggered activity, and micro-reentry.
Focal atrial tachycardia is the least common (5 to 10%) form of paroxysmal supraventricular tachycardia (4) and usually occurs in patients with a structural heart disorder. Other causes include atrial irritation (eg, pericarditis), medications (eg, digoxin), alcohol, and toxic gas inhalation. ), medications (eg, digoxin), alcohol, and toxic gas inhalation.
Symptoms are those of other tachycardias (eg, light-headedness, dizziness, palpitations, and rarely syncope). When focal atrial tachycardia is incessant, it may lead to a tachycardic cardiomyopathy and heart failure.
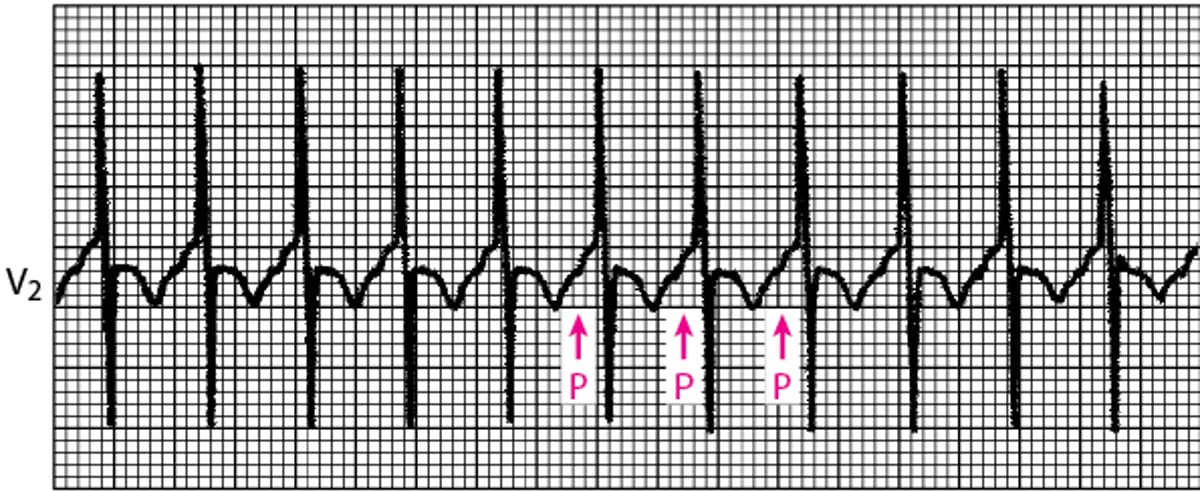
Diagnosis is by electrocardiography (ECG); P waves, which differ in morphology from normal sinus P waves, precede QRS complexes but may be hidden within the preceding T wave (see figure Focal Atrial Tachycardia).
Focal Atrial Tachycardia
This narrow QRS tachycardia arises from an abnormal automatic focus or micro-reentry. P waves precede the QRS complexes; it is often a long RP interval tachycardia (PR < RP) but may be a short RP tachycardia (PR > RP) if atrioventricular nodal conduction is slow. |

Vagal maneuvers may be used to slow the heart rate, allowing visualization of P waves when they are hidden, but these maneuvers do not usually terminate the arrhythmia (because the AV node is not an obligate part of the arrhythmia circuit).
Acute treatment begins with IV adenosine, which may terminate atrial tachycardias due to Acute treatment begins with IV adenosine, which may terminate atrial tachycardias due toadenosine-sensitive delayed after depolarizations (DAD) that result from intracellular calcium overload (one form of triggered activity) or reveal the mechanism by producing AV block without termination of the tachycardia. Acute treatment includes discontinuing digoxin therapy when this is the cause. The ventricular response rate may be slowed with an IV beta-blocker,IV verapamil, or IV diltiazem (-sensitive delayed after depolarizations (DAD) that result from intracellular calcium overload (one form of triggered activity) or reveal the mechanism by producing AV block without termination of the tachycardia. Acute treatment includes discontinuing digoxin therapy when this is the cause. The ventricular response rate may be slowed with an IV beta-blocker,IV verapamil, or IV diltiazem (5), although this is often unsuccessful. The atrial arrhythmia may be terminated by IV procainamide, IV flecainide, or IV amiodarone. An episode may also be terminated by ), although this is often unsuccessful. The atrial arrhythmia may be terminated by IV procainamide, IV flecainide, or IV amiodarone. An episode may also be terminated bydirect current cardioversion.
Pharmacologic approaches to prevention of focal atrial tachycardia include beta-blockers, non-dihydropyridine calcium channel blockers, and/or antiarrhythmic medications in class Ia, Ic, or III (5). Transcatheter ablation of focal atrial tachycardia, which is effective and reasonably safe, is the preferred approach for chronic prophylaxis.
Multifocal atrial tachycardia
Multifocal atrial tachycardia (chaotic atrial tachycardia) is an irregularly irregular rhythm caused by the random discharge of multiple ectopic atrial foci. By definition, heart rate is > 100 beats/minute. On ECG, P-wave morphology differs from beat to beat, and there are ≥ 3 distinct P-wave morphologies. The presence of P waves distinguishes multifocal atrial tachycardia from atrial fibrillation. Except for the rate, features are the same as those of wandering atrial pacemaker. Symptoms, when they occur, are those of rapid tachycardia. Multifocal atrial tachycardia can be due to an underlying pulmonary disorder such as chronic obstructive pulmonary disease, especially when accompanied by hypoxia, acidosis, theophylline-intoxication, or a combination. Less commonly, it is caused by underlying cardiac disease such as coronary artery disease, and electrolyte abnormalities such as hypokalemia. Treatment is directed at the underlying disorder. When therapy directed at the arrhythmia is required, the most effective agents are IV magnesium, IV verapamil, and a beta-blocker (. Treatment is directed at the underlying disorder. When therapy directed at the arrhythmia is required, the most effective agents are IV magnesium, IV verapamil, and a beta-blocker (5). Treatment with digoxin, class I or III antiarrhythmic medications, or cardioversion is usually ineffective (). Treatment with digoxin, class I or III antiarrhythmic medications, or cardioversion is usually ineffective (5).
Wandering atrial pacemaker
Wandering atrial pacemaker (multifocal atrial rhythm) is an irregularly irregular rhythm caused by the random discharge of multiple ectopic atrial foci. By definition, heart rate is ≤ 100 beats/minute. Except for the rate, features are the same as those of multifocal atrial tachycardia. Treatment is directed at causes, which tend to be the same as the causes of atrial premature beats.
Nonparoxysmal junctional tachycardia
Nonparoxysmal junctional tachycardia is caused by abnormal automaticity in the AV node or adjacent tissue, which typically follows open heart surgery, acute inferior myocardial infarction, myocarditis, or digitalis toxicity. Heart rate is 60 to 120 beats/minute; thus, symptoms are usually absent. ECG shows regular, normal-appearing QRS complexes without identifiable P waves or with retrograde P waves (inverted in the inferior leads) that occur shortly before (< 0.1 second) or after the QRS complex. The rhythm is distinguished from paroxysmal supraventricular tachycardia by the lower heart rate and gradual onset and offset. Treatment is directed at the underlying heart disorder.
Junctional ectopic tachycardia
Junctional ectopic tachycardia (JET) is a rare (< 1%) supraventricular tachycardia that is caused by enhanced automaticity, abnormal automaticity, or triggered activity in the AV node, His bundle, or adjacent atrial tissue; the automaticity may be congenital (occurring in utero or in the first 6 months of life), postoperative (in children after heart surgery that includes surgery near the junction), or in adults with myocardial ischemia or digoxin-intoxication (Junctional ectopic tachycardia (JET) is a rare (digoxin-intoxication (6). Heart rate is 200 to 250 beats/minute in children; thus, a tachycardia-induced cardiomyopathy and heart failure may result. JET is distinguished from nonparoxysmal junctional tachycardia by the faster rate and the sudden onset-sudden/offset character of JET. JET is rare in adults, and the rate is slower, in the range of 120 to 200 beats/minute. Antiarrhythmic pharmacotherapy may be successful with amiodarone, flecainide, ivabradine, procainamide, propranolol, or verapamil (). Heart rate is 200 to 250 beats/minute in children; thus, a tachycardia-induced cardiomyopathy and heart failure may result. JET is distinguished from nonparoxysmal junctional tachycardia by the faster rate and the sudden onset-sudden/offset character of JET. JET is rare in adults, and the rate is slower, in the range of 120 to 200 beats/minute. Antiarrhythmic pharmacotherapy may be successful with amiodarone, flecainide, ivabradine, procainamide, propranolol, or verapamil (5). Transcatheter ablation is less successful than in other supraventricular tachycardias and has a higher risk of inadvertent creation of AV block.
References
1. Mond HG, Haqqani HM: The Electrocardiographic Footprints of Atrial Ectopy. Heart Lung Circ 28(10):1463–1471, 2019. doi: 10.1016/j.hlc.2019.03.005
2. Durmaz E, Ikitimur B, Kilickiran Avci B, et al: The clinical significance of premature atrial contractions: How frequent should they become predictive of new-onset atrial fibrillation. Ann Noninvasive Electrocardiol 25(3):e12718, 2020. doi:10.1111/anec.12718
3. Huang BT, Huang FY, Peng Y, et al: Relation of premature atrial complexes with stroke and death: Systematic review and meta-analysis. Clin Cardiol 40(11):962–969, 2017. doi:10.1002/clc.22780
4. Porter MJ, Morton JB, Denman R, et al: Influence of age and gender on the mechanism of supraventricular tachycardia. Heart Rhythm 1(4):393–396, 2004. doi: 10.1016/j.hrthm.2004.05.007
5. Brugada J, Katritsis DG, Arbelo E, et al: 2019 ESC Guidelines for the management of patients with supraventricular tachycardia. The Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J 41(5):655–720, 2020. doi: 10.1093/eurheartj/ehz467
6. Alasti M, Mirzaee S, Machado C, et al: Junctional ectopic tachycardia (JET). J Arrhythm 36(5):837–844, 2020. doi: 10.1002/joa3.12410







