


Allergic (including atopic) and other hypersensitivity disorders are inappropriate or exaggerated immune reactions to foreign antigens. Inappropriate immune reactions include those that are misdirected against intrinsic body components (self), leading to autoimmune disorders. This topic focuses on type I hypersensitivity reactions.
Classification of Hypersensitivity Reactions
Hypersensitivity reactions are divided into 4 types (I through IV) by the Gell and Coombs classification. Hypersensitivity disorders often involve more than 1 type.
Type I hypersensitivity reactions
Type I reactions (immediate hypersensitivity) are IgE-mediated. Antigen binds to IgE that is bound to tissue mast cells and blood basophils, triggering release of preformed mediators (eg, histamine, proteases, chemotactic factors) and synthesis of other mediators (eg, prostaglandins, leukotrienes, platelet-activating factor, cytokines). These mediators cause vasodilation, increased capillary permeability, mucus hypersecretion, smooth muscle spasm, and tissue infiltration with eosinophils, type 2 helper T (TH2) cells, and other inflammatory cells.
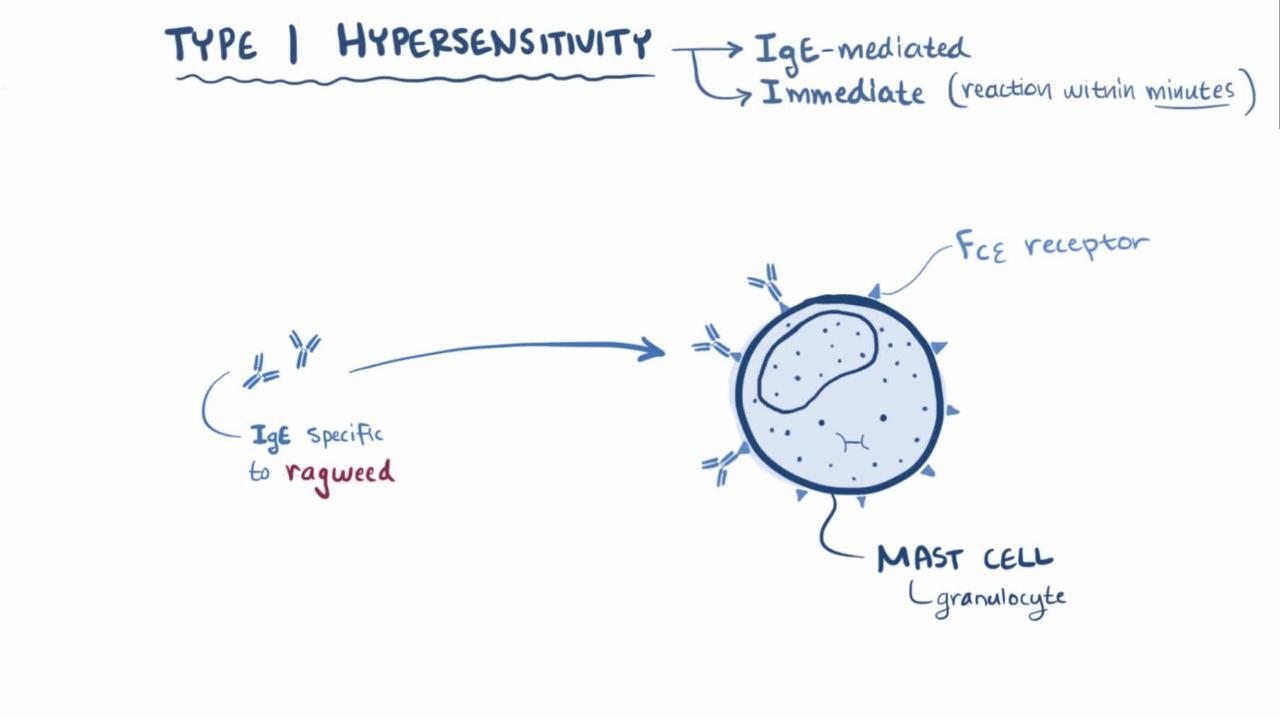
Type I hypersensitivity reactions develop < 1 hour after exposure to antigen.
Type I reactions underlie all atopic disorders (eg, atopic dermatitis, allergic asthma, rhinitis, conjunctivitis) and many allergic disorders (eg, anaphylaxis, some cases of angioedema, urticaria, latex and some food allergies). The terms atopy and allergy are often used interchangeably but are different:
Atopy is an exaggerated IgE-mediated immune response; all atopic disorders are type I hypersensitivity disorders.
Allergy is any exaggerated immune response to a foreign antigen regardless of mechanism.
Thus, all atopic disorders are considered allergic, but many allergic disorders (eg, hypersensitivity pneumonitis) are not atopic.
Atopic disorders most commonly affect the nose, eyes, skin, and lungs. These disorders include conjunctivitis, extrinsic atopic dermatitis (the most common type of eczema), immune-mediated urticaria, some forms of angioedema, acute latex allergy, some allergic lung disorders (eg, allergic asthma, IgE-mediated components of allergic bronchopulmonary aspergillosis), allergic rhinitis, and allergic reactions to venomous stings.
Type II hypersensitivity reactions
Type II reactions (antibody-dependent cytotoxic hypersensitivity) result when antibody binds to cell surface antigens or to a molecule coupled to a cell surface. The surface-bound antigen-antibody structure (as opposed to the circulating antigen-antibody complex in type III hypersensitivity) activates cells that participate in antibody-dependent cell-mediated cytotoxicity (eg, natural killer cells, eosinophils, macrophages), complement, or both. The result is cell and tissue damage.
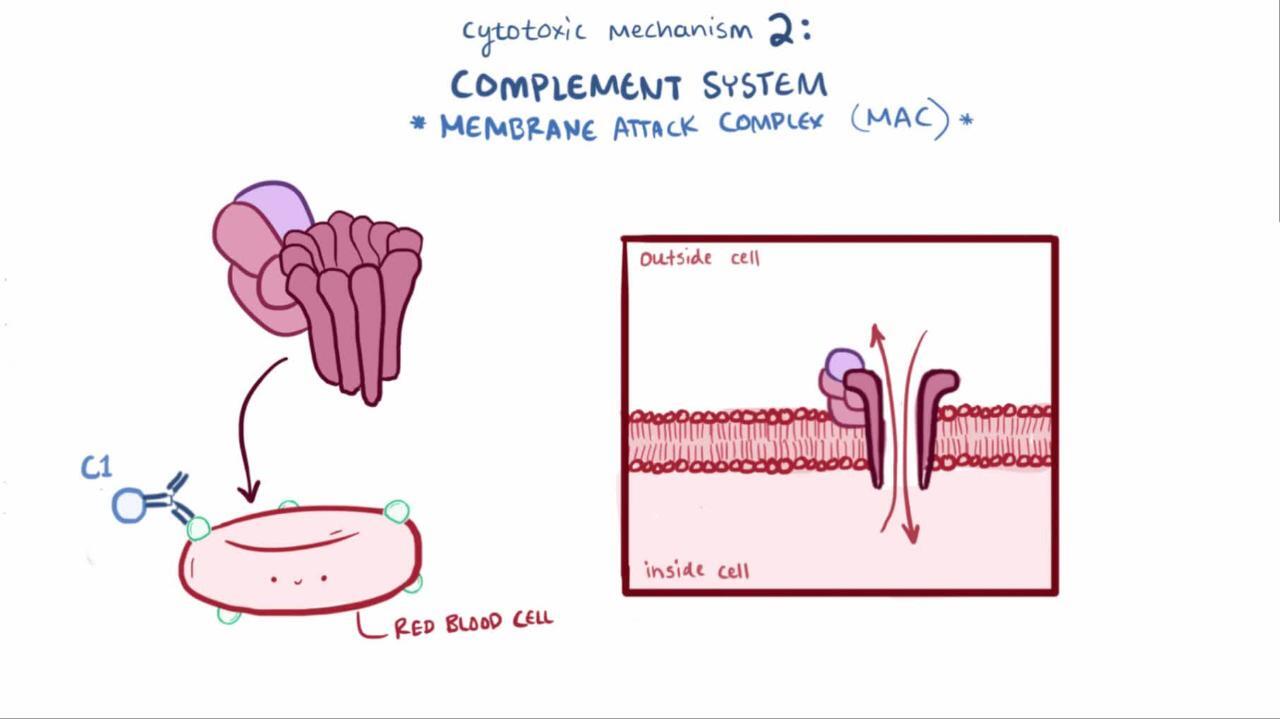
Disorders involving type II reactions include hyperacute graft rejection of an organ transplant, Coombs-positive hemolytic anemias, Hashimoto thyroiditis, and anti–glomerular basement membrane disease (eg, Goodpasture syndrome).
Type III hypersensitivity reactions
Type III reactions (immune complex disease) cause inflammation in response to circulating antigen-antibody immune complexes deposited in vessels or tissue. These complexes can activate the complement system or bind to and activate certain immune cells, resulting in release of inflammatory mediators.
Consequences of immune complex formation depend in part on the relative proportions of antigen and antibody in the immune complex. Early in the immune response, there is excess antigen with small antigen-antibody complexes, which do not activate complement. Later, when antigen and antibody are more balanced, immune complexes are larger and tend to be deposited in various tissues (eg, glomeruli, blood vessels), causing systemic reactions. The isotype of induced antibodies changes during an immune response, and the isotype, glycosylation, size, and charge of the complex’s components contribute to the clinical response.
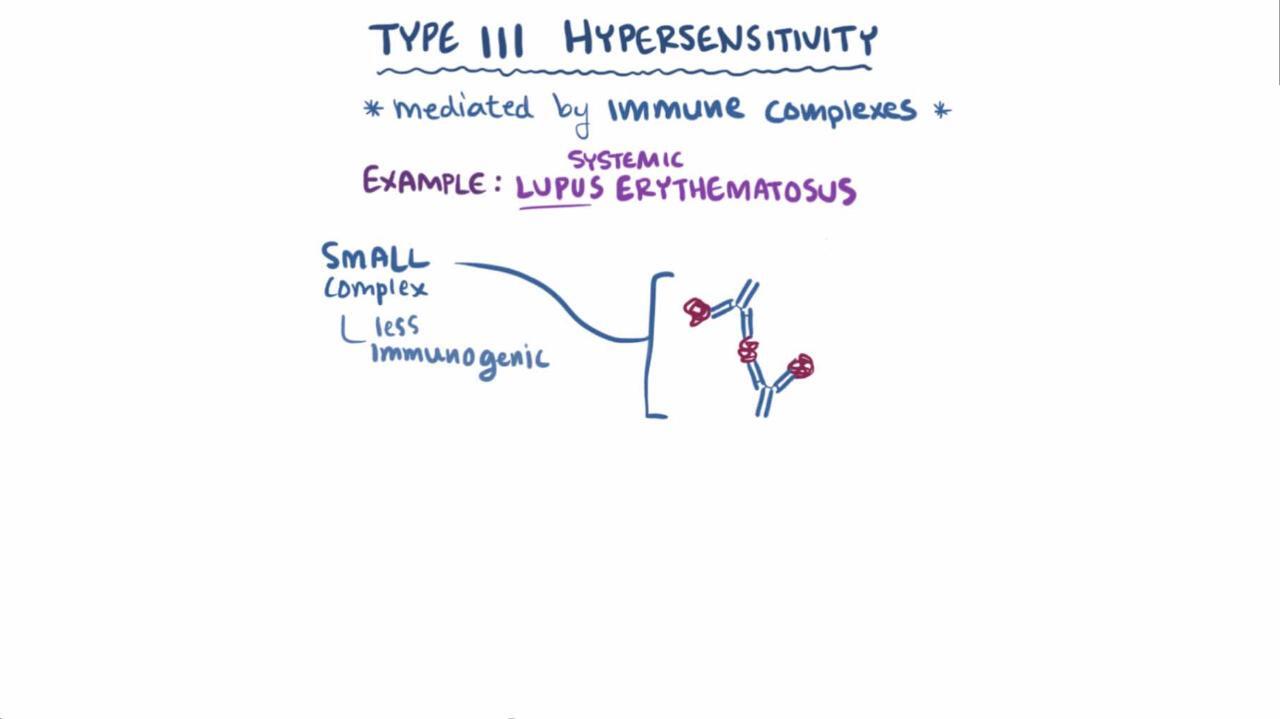
Type III disorders include serum sickness, systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), leukocytoclastic vasculitis, cryoglobulinemia, acute hypersensitivity pneumonitis, and several types of glomerulonephritis.
Type III reactions develop 4 to 10 days after exposure to antigen and, if exposure to the antigen continues, can become chronic.
Type IV hypersensitivity reactions
Type IV reactions (delayed hypersensitivity) do not involve antibodies but are mediated by T cells.
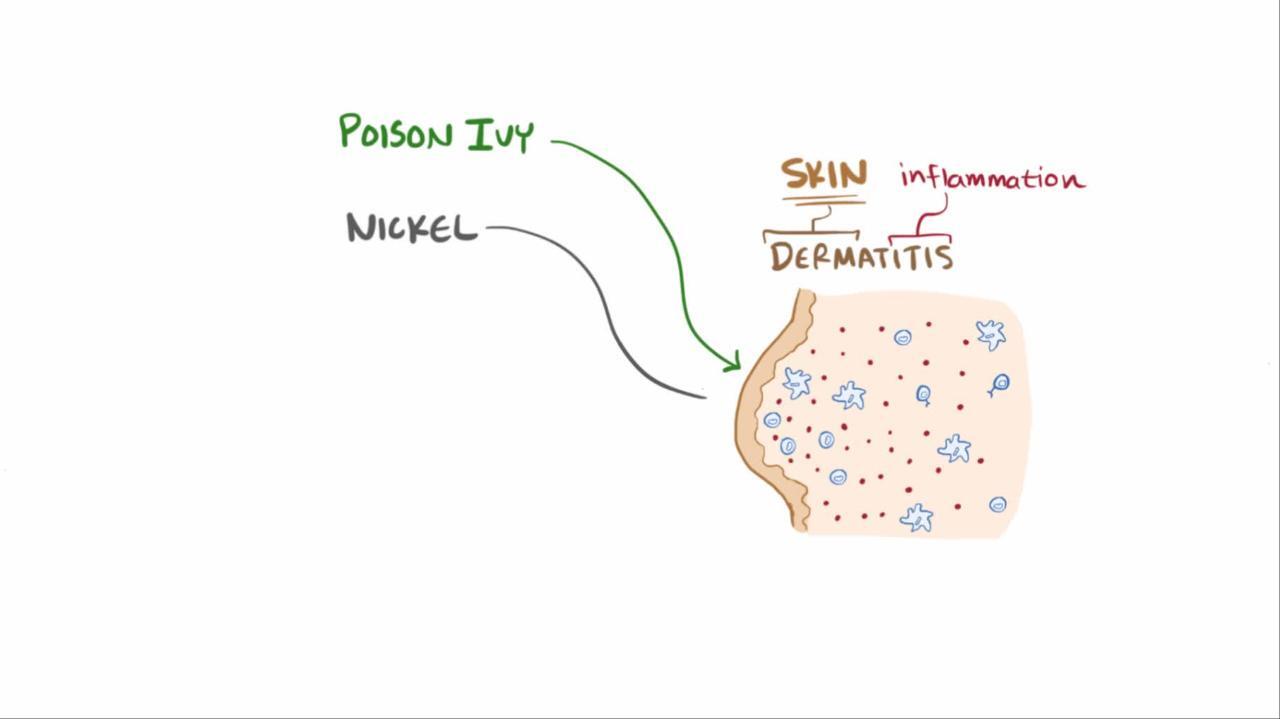
T cells, sensitized after contact with a specific antigen, are activated by continued exposure or reexposure to the antigen; they damage tissue by direct toxic effects or through release of cytokines, which activate eosinophils, monocytes and macrophages, neutrophils, or natural killer cells.
Disorders involving type IV reactions include Stevens-Johnson syndrome, toxic epidermal necrolysis (SJS/TEN), drug rash with eosinophilia and systemic symptoms (DRESS), contact dermatitis (eg, poison ivy), subacute and chronic hypersensitivity pneumonitis, acute and chronic allograft rejection, the immune response to tuberculosis, and many forms of drug hypersensitivity.
Etiology of Allergic and Atopic Disorders
Complex genetic, environmental, and site-specific factors contribute to development of IgE-mediated allergies.
Genetic factors may be involved, as suggested by familial inheritance of disease, association between atopy and specific human leukocyte antigen (HLA) loci, and polymorphisms of several genes, including those for the high-affinity IgE receptor beta-chain, IL-4 receptor alpha-chain, interleukin (IL)-4, IL-13, CD14, dipeptidyl-peptidase 10 (DPP10), and a disintegrin and metalloprotease domain 33 (ADAM33).
Environmental factors interact with genetic factors to maintain type 2 helper T (TH2) cell–directed immune responses. TH2 cells activate eosinophils, promote IgE production, and are proallergic. Early childhood exposure to bacterial and viral infections and endotoxins (eg, lipopolysaccharide) may shift native TH2-cell responses to type 1 helper T (TH1)–cell responses, which suppress TH2 cells and therefore discourage allergic responses. Regulatory T (Treg) cells (eg, CD4+, CD25+, Foxp3+), which are capable of suppressing TH2-cell responses, and IL-12–secreting dendritic cells, which drive TH1-cell responses, are perhaps also involved. Trends in more economically advantaged countries toward smaller families with fewer children, cleaner indoor environments, and more widespread use of antibiotics may limit children's exposure to the infectious agents that drive a predominantly TH1-cell response; such trends may explain the increased prevalence of some allergic disorders.
Other factors thought to contribute to allergy development include chronic allergen exposure and sensitization, diet, and environmental pollutants.
Anatomic site-specific factors include adhesion molecules in bronchial epithelium and skin and molecules in the gastrointestinal (GI) tract that direct TH2 cells to target tissues. The composition of the GI tract, respiratory tract, and skin microbiota appears to strongly influence the development of allergy. These microbiota may provide new targets for allergy therapy.
Allergens
By definition, an allergen induces type I IgE-mediated or type IV T-cell–mediated immune responses. Allergic triggers are almost always low molecular weight proteins; many of them can become attached to airborne particles.
Sources of allergens that most commonly cause acute and chronic allergic reactions (type I and type IV) include
House dust mite feces
Animal dander
Pollens (tree, grass, weed)
Molds
Insect saliva and venom (transmitted by bites and stings)
Household chemicals (eg, hydroxyisohexyl 3-cyclohexene carboxaldehyde, cinnamal, eugenol)
For type IV hypersensitivity reactions, medications are the most common cause.
Pathophysiology of Allergic and Atopic Disorders
When allergen binds to IgE-sensitized mast cells and basophils, histamine is released from their intracellular granules. Mast cells are widely distributed but are most concentrated in skin, lungs, and gastrointestinal (GI) mucosa; histamine facilitates inflammation and is the primary mediator of clinical atopy. Physical disruption of tissue and various substances (eg, tissue irritants, opiates, surface-active agents, complement components C3a and C5a) can trigger histamine release directly, independent of IgE.
Histamine causes the following:
Local vasodilation (causing erythema)
Increased capillary permeability and edema (producing a wheal)
Vasodilation of surrounding arterioles mediated by neuronal reflex mechanisms (causing flare—the redness around a wheal)
Stimulation of sensory nerves (causing itching)
Smooth muscle contraction in the airways (bronchoconstriction) and in the GI tract (increasing GI motility)
Increased nasal, salivary, and bronchial gland secretions
When released systemically, histamine is a potent arteriolar dilator and can cause extensive peripheral pooling of blood and hypotension; cerebral vasodilation may be a factor in vascular headache. Histamine increases capillary permeability; the resulting loss of plasma and plasma proteins from the vascular space can worsen circulatory shock. This loss triggers a compensatory catecholamine surge from adrenal chromaffin cells.
Symptoms and Signs of Allergic and Atopic Disorders
Common symptoms of type I hypersensitivity allergic disorders include
Rhinorrhea, sneezing, and nasal congestion (upper respiratory tract)
Wheezing and dyspnea (lower respiratory tract)
Itching (eyes, nose, skin)
Signs may include nasal turbinate edema, sinus pain during palpation, wheezing, conjunctival hyperemia and edema, urticaria, angioedema, dermatitis, and (if chronic) skin lichenification.
Stridor, wheezing, and hypotension are life-threatening signs of anaphylaxis.
Diagnosis of Allergic and Atopic Disorders
History and physical examination
Sometimes complete blood count (to check for eosinophilia) and occasionally serum IgE levels (nonspecific tests)
Often skin testing and allergen-specific serum IgE testing (specific tests)
Rarely provocative testing
A thorough history is generally more reliable than testing or screening. History should include
Questions about frequency and duration of attacks and changes over time
Triggering factors if identifiable
Relation to seasonal or situational settings (eg, predictably occurring during pollen seasons; after exposure to animals, hay, or dust; during exercise; or in particular places)
Family history of similar symptoms or of atopic disorders
Responses to attempted treatments
Age at onset may be important in asthma because childhood asthma is likely to be atopic and asthma beginning after age 30 is not.
Nonspecific tests
Certain tests can suggest but not confirm an allergic origin of symptoms.
Complete blood count (CBC) may be done to detect eosinophilia if patients are not taking corticosteroids, which reduce the eosinophil count. However, CBC is of limited value because although eosinophils may be increased in atopy or other conditions (eg, drug hypersensitivity, cancer, inflammatory bowel disease, parasitic infection), a normal eosinophil count does not exclude allergy. Total white blood cell count is usually normal. Anemia and thrombocytosis are not typical of allergic responses and should prompt consideration of a systemic inflammatory disorder.
Conjunctival or nasal secretions or sputum can be examined for leukocytes; finding any eosinophils suggests that TH2-mediated inflammation is likely.
Total serum IgE levels are elevated in atopic disorders but are of little help in making a specific allergic diagnosis because they may also be elevated in parasitic infections, infectious mononucleosis, some autoimmune disorders, drug reactions, immunodeficiency disorders (hyper-IgE syndrome and Wiskott-Aldrich syndrome), IgG4-related disease, and in some forms of multiple myeloma. IgE levels are helpful for following response to therapy in allergic bronchopulmonary aspergillosis.
Specific tests
Skin testing uses standardized concentrations of antigen introduced directly into skin and is indicated when a detailed history and physical examination do not identify the cause and triggers for persistent or severe symptoms. Skin testing has higher positive predictive values for diagnosing allergic rhinitis and conjunctivitis than for diagnosing allergic asthma or food allergy; negative predictive value for food allergy is high (1).
The most commonly used antigens are pollens (tree, grass, weed), molds, house dust mite feces, animal danders and sera, insect venom, foods, and beta-lactam antibiotics. Choice of antigens to include is based on patient history and geographic prevalence.
Two skin test techniques can be used:
Percutaneous (prick)
Intradermal
The prick test can detect most common allergies; it is usually done first. The intradermal test is more sensitive but less specific; it can be used to evaluate sensitivity to allergens when prick test results are negative or equivocal.
For the prick test, a drop of antigen extract is placed on the skin, which is then tented up and pricked or punctured through the extract with the tip of a 27-gauge needle held at a 20° angle or with a commercially available prick device.
If no allergen is identified in the prick test, an intradermal test is done.
For the intradermal test, just enough extract to produce a 1- or 2-mm bleb (typically 0.02 mL) is injected intradermally with a 0.5- or 1-mL syringe and a 27-gauge short-bevel needle.
Prick and intradermal skin testing should include the diluent alone as a negative control and histamine (10 mg/mL for prick tests, 0.01 mL of a 1:1000 solution for intradermal tests) as a positive control. For patients who have had a recent (< 1 year) generalized reaction to the test antigen, testing begins with the standard reagent diluted 100-fold, then 10-fold, and then the standard concentration.
A test is considered positive if a wheal and flare reaction occurs and wheal diameter is 3 to 5 mm greater than that of the negative control after 15 to 20 minutes.
False positives occur in dermatographism (a wheal and flare reaction provoked by stroking or scraping the skin). False negatives occur when allergen extracts have been stored incorrectly or are outdated.
Certain medications can also interfere with results and should be stopped a few days to a week before testing. These medications include over-the-counter (OTC) and prescription antihistamines, tricyclic antidepressants, omalizumab, and monoamine oxidase inhibitors. Some clinicians suggest that testing should be avoided in patients taking beta-blockers because these patients are more likely to have risk factors for severe reactions. These risk factors tend to predict limited cardiopulmonary reserve and include coronary artery disease, arrhythmias, and older age. Also, beta-blockers can interfere with treatment of severe reactions by blocking response to beta-adrenergic agonists such asepinephrine.
Allergen-specific serum IgE tests use an enzyme-labeled anti-IgE antibody to detect binding of serum IgE to a known allergen. These tests are done when skin testing might be ineffective or risky—for example, when drugs that interfere with test results cannot be temporarily stopped before testing or when a skin disorder such as eczema, dermatographism, or psoriasis would make skin testing difficult. For allergen-specific serum IgE tests, the allergen is immobilized on a synthetic surface. After incubation with patient serum and enzyme-labeled anti-IgE antibody, a substrate for the enzyme is added; the substrate provides colorimetric, fluorescent, or chemiluminescent detection of binding. Allergen-specific IgE tests have replaced radioallergosorbent testing (RAST), which used 125-I-labeled anti-IgE antibody. Although the allergen-specific serum IgE tests are not radioactive, they are still sometimes referred to as RAST.
Provocative testing includes an oral challenge, which involves direct exposure of the mucosae to allergen; it is indicated for patients who must document their reaction (eg, for occupational or disability claims) and for excluding an IgE-mediated allergy in patients thought to be at low risk of allergy. This test is frequently done to exclude food and medication allergy. Other types of provocative testing include asking patients to exercise to diagnose exercise-induced asthma. Various provocative tests for physical urticaria can be done in the office; they include placing an ice cube on the skin for 4 minutes to diagnose cold-induced urticaria, asking patients to exercise to increase body temperature and thus confirm cholinergic urticaria, and placing a vortex (laboratory vibratory device) on a patient's arm or hand to identify mast-cell mediated vibratory urticaria.
Nasal and bronchial challenge are primarily research tools, but bronchial challenge is sometimes used when the clinical significance of a positive skin test is unclear or when no antigen extracts are available (eg, for work-related asthma).
Diagnosis reference
1. Patel G, Saltoun C. Skin testing in allergy. Allergy Asthma Proc 2019;40(6):366-368. doi:10.2500/aap.2019.40.4248
Treatment of Allergic and Atopic Disorders
Emergency treatment
Removal or avoidance of allergic triggers
H1 blockers
Mast cell stabilizers
Anti-inflammatory corticosteroids and leukotriene inhibitors
Immunotherapy (desensitization)
Emergency treatment
Severe allergic reactions (eg, anaphylaxis) require prompt emergency treatment with epinephrine.
If the airways are affected (eg, in angioedema), securing an airway is the highest priority. Treatment may include epinephrine and/or endotracheal intubation.
Patients who have severe allergic reactions should be advised to always carry a prefilled, self-injecting syringe of epinephrine and oral antihistamines and, if a severe reaction occurs, to use these treatments as quickly as possible and then go to the emergency department. There, patients can be closely monitored and treatment can be repeated or adjusted as needed.
Environmental control
Removal or avoidance of allergic triggers is the primary treatment and preventive strategy for allergy. However, when patients are sensitized to multiple allergens, complete avoidance is essentially impossible.
Antihistamines
Antihistamines block histamine receptors; they do not affect histamine production or metabolism. There are 4 different histamine receptors: H1, H2, H3, and H4.
Antihistamines that block the H1 receptor (H1 blockers) are a mainstay of treatment for allergic disorders. H2 blockers are used primarily for gastric acid suppression and but are useful for certain allergic reactions; they may be indicated as adjunctive therapy for treatment of anaphylaxis, mastocytosis, and certain atopic disorders, especially chronic spontaneous urticaria.
Oral H1 blockers relieve symptoms in various atopic and allergic disorders (eg, seasonal hay fever, allergic rhinitis, conjunctivitis, urticaria, other dermatoses, minor reactions to blood transfusion incompatibilities); they are less effective for allergic bronchoconstriction and systemic vasodilation. Onset of action is usually 15 to 30 minutes, with peak effects in 1 hour; duration of action is usually 3 to 6 hours.
Products that contain an oral H1 blocker and a sympathomimetic (eg, pseudoephedrine) are widely available over-the-counter for use in adults and children ≥ 12 years. These products are particularly useful when both an antihistamine and an intranasal decongestant are needed; however, they are sometimes contraindicated (eg, if patients are taking a monoamine oxidase inhibitor [MAOI]).
Oral H1 blockers are classified as
First-generation: Sedating
Second-generation: Nonsedating (better thought of as less sedating)
First-generation antihistamines are widely available without prescription. They easily cross the blood-brain barrier. All have significant sedative and anticholinergic properties; they pose particular problems for older patients and for patients with glaucoma, benign prostatic hyperplasia, constipation, orthostatic hypotension, delirium, or dementia.
Second-generation antihistamines are also widely available without prescription. They do not cross the blood-brain barrier as easily as first-generation antihistamines. Second-generation antihistamines are usually preferred.
Antihistamines may be given by various routes, including
Oral (multiple—see table Oral H1 Blockers)
Intranasal (azelastine or olopatadine to treat rhinitis)
Ocular (eg, azelastine, emedastine, ketotifen, levocabastine, olopatadine, pemirolast [not available in the United States] to treat conjunctivitis)
Cutaneous (eg, diphenhydramine, doxepin)
Oral H1 Blockers
Medication | Available Preparations |
|---|---|
First-generation* | |
Brompheniramine† | Available only as combination products with a decongestant or an antitussive, which are not recommended for children < 6 years 4-, 8-, and 12-mg tablets 2 mg/5 mL elixir 8- and 12-mg tablets (sustained-release, single-entity) |
Chlorpheniramine† | Available only as combination products with a decongestant or an antitussive, which are not recommended for children < 6 years 2-mg chewable tablets 4-, 8-, and 12-mg tablets Extended-release: 12-mg tablets or capsules 2 mg/5 mL syrup |
Clemastine | 1.34- and 2.68-mg tablets 0.67 mg/5 mL syrup |
Cyproheptadine | 4-mg tablets 2 mg/5 mL syrup |
Dexchlorpheniramine | 2-mg tablets 2 mg/5 mL syrup 4- and 6-mg tablets (extended-release) |
Diphenhydramine | 25- and 50-mg capsules or tablets 12.5-mg chewable tablet 12.5 mg/5 mL elixir 12.5 mg/mL syrup |
Hydroxyzine | 25-, 50-, and 100-mg capsules 10-, 25-, 50-, and 100-mg tablets 10 mg/5 mL syrup 25 mg/5 mL oral suspension |
Promethazine | Safer alternatives preferred for allergic disorders in children 12.5-, 25-, and 50-mg tablets 6.25 mg/5 mL and 25 mg/5 mL syrup |
Second-generation | |
Acrivastine/pseudoephedrine | 8-mg acrivastine plus 60-mg pseudoephedrine capsules |
Cetirizine | 5- and 10-mg tablets 1 mg/mL syrup |
Desloratadine | 5-mg tablets 0.5 mg/mL syrup |
Fexofenadine | 30-, 60-, and 180-mg tablets 30-mg orally disintegrating tablets 6 mg/mL oral suspension |
Levocetirizine | 5-mg tablets 0.5 mg/mL oral solution |
Loratadine | 10-mg tablets and capsules 5-mg chewable tablets 5- and 10-mg disintegrating oral tablets 1 mg/mL syrup 1 mg/mL oral solution |
Mizolastine | 10-mg tablets |
* Most first-generation antihistamines have strong anticholinergic properties. Generally, they should not be used in older adults or in patients with glaucoma, benign prostatic hyperplasia, constipation, delirium, dementia, or orthostatic hypotension. These medications commonly cause sedation, dry mouth, blurred vision, urinary retention, constipation, and orthostatic hypotension. In children, first-generation antihistamines should be used only as needed given their potential adverse effects, particularly when combined with other medications; second-generation antihistamines are preferred for allergic rhinitis. | |
† Usually, brompheniramine and chlorpheniramine are available only in combination with other medications (eg, decongestants, cough suppressants).Brompheniramine and chlorpheniraminecombined with other medications (eg, dextromethorphan, phenylephrine) should not be used in children < 6 years. | |
Mast cell stabilizers
Mast cell stabilizers block the release of mediators from mast cells.
Mast cell stabilizers are used when other medications (eg, antihistamines, topical corticosteroids) are ineffective or not well-tolerated. They are also frequently used in patients with mast cell disease when mast activation and release of mediators overwhelms conventional antihistamines.
These medications may be given
Orally (cromolyn, ketotifen)
Intranasally (eg, azelastine, cromolyn)
Ocularly (eg, azelastine, cromolyn, lodoxamide, ketotifen, nedocromil, olopatadine, pemirolast)
Several ocular and intranasal medications (eg, azelastine, ketotifen, olopatadine, pemirolast) are dual-acting mast cell stabilizers/antihistamines.
Anti-inflammatory medications
Corticosteroids can be given intranasally (see tables Intranasal Corticosteroids and Intranasal Mast Cell Stabilizers) or orally.
Oral corticosteroids are indicated for the following:
Allergic disorders that are severe but self-limited and not easily treated with topical corticosteroids (eg, acute asthma exacerbations, severe widespread contact dermatitis)
Disorders refractory to other measures
Ocular corticosteroids are used only when an ophthalmologist is involved because infection and increased intraocular pressure are potential adverse effects.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are typically not useful, with the exception of topical forms used to relieve conjunctival injection and itching due to allergic conjunctivitis.
Intranasal Corticosteroids
Medication | Dose per Spray |
|---|---|
Beclomethasone | 42 mcg |
40 mcg | |
80 mcg | |
Budesonide | 32 mcg |
Ciclesonide | Nasal aerosol (37 mcg) Nasal spray (50 mcg) |
Flunisolide | 25 mcg |
Fluticasone furoate | 27.5 mcg |
Fluticasone propionate* | 50 mcg |
Mometasone | 50 mcg |
Triamcinolone | 55 mcg |
* A combination of azelastine/fluticasone (137 mcg/50 mcg) is available. | |
Intranasal Mast Cell Stabilizers
Medication | Dose per Spray |
|---|---|
Azelastine*,† | 137 mcg in 0.1% solution 205.5 mg in 0.15% solution |
Cromolyn | 5.2 mg |
Olopatadine* | 665 mcg |
* Azelastine and olopatadine are dual-acting mast cell stabilizers/antihistamines. | |
† A combination of azelastine/fluticasone (137 mcg/50 mcg) is available. | |
Other medications
Leukotriene inhibitors(eg, montelukast, zafirlukast, zileuton) are indicated for treatment of the following (see also tableMedication Treatment of Asthma):
Mild persistent asthma; Montelukast, zafirlukast, or zileuton
Seasonal allergic rhinitis: Montelukast
Urticaria: Montelukast or zafirlukast
Anti-IgE antibody (omalizumab) is indicated for the following:
Moderately persistent or severe asthma refractory to standard treatment
Chronic idiopathic urticaria refractory to antihistamine therapy
Nasal polyps
Type 1 allergic reactions (including anaphylaxis) that may occur with accidental exposure to 1 or more foods in patients ≥ 1 year old with IgE-mediated food allergy
Immunotherapy
Exposure to allergen in gradually increasing doses (hyposensitization or desensitization) via injection or orally or in high doses sublingually can induce tolerance. This therapy is indicated when allergen exposure cannot be avoided and pharmacotherapy is inadequate.
Mechanism is unknown but may involve induction of the following:
IgG antibodies, which compete with IgE for allergen or block IgE from binding with mast cell IgE receptors
Interferon-gamma, IL-12, and cytokines secreted by TH1 cells
Regulatory T cells
For full effect, injections are initially given once or twice a week. Dose typically starts at 0.1 to 1.0 biologically active units (BAU), depending on how sensitive the patient appears to be, and is increased weekly or every 2 weeks by ≤ 2 times with each injection until the maximum tolerated dose (the dose that begins to elicit moderate adverse effects) is established. Patients should be observed for about 30 minutes postinjection during dose escalation because anaphylaxis may occur after injection. Subsequently, injections of the maximum tolerated dose should be given every 2 to 4 weeks year-round; year-round treatment is better than preseasonal or coseasonal treatment, even for seasonal allergies.
Allergens used are those that typically cannot be avoided:
Pollens
House dust mite feces
Molds
Venom of stinging insects
Insect venoms are standardized by weight. Animal dander desensitization is ordinarily limited to patients who cannot avoid exposure (eg, veterinarians, laboratory workers), but there is little evidence that it is useful. Desensitization for peanut is available and has been successful in about 60 to 80% of the cases (1). Desensitization for penicillin and certain other medications and for foreign (xenogeneic) serum can be done. Desensitization for medication allergies is successful in most cases (2).
Adverse effects are most commonly related to overdose, occasionally via inadvertent IM or IV injection of a dose that is too high, and range from mild cough or sneezing to generalized urticaria, severe asthma, anaphylactic shock, and, rarely, death. Adverse effects can be prevented by the following:
Increasing the dose in small increments
Repeating or decreasing the dose if local reaction to the previous injection is large (≥ 2.5 cm in diameter)
Reducing the dose when a fresh extract is used
Reducing the dose of pollen extract during pollen season is recommended. Epinephrine, oxygen, and resuscitation equipment should be immediately available for prompt treatment of anaphylaxis.
Sublingual immunotherapy with grass pollen, ragweed, or house dust mite allergen extracts can be used for allergic rhinitis when it is induced by these allergens. The first dose is given in a health care setting; patients should be observed for 30 minutes after administration because anaphylaxis may occur. If the first dose is tolerated, patients take subsequent doses daily at home. In adults, the initial dose is not increased, but in children and adolescents aged 10 to 17 years, the dose is increased over the first 3 days. In patients with grass pollen or ragweed allergy, treatment is initiated at least 3 months before the onset of each grass pollen or ragweed season and maintained throughout the season.
The anaphylaxis rate to commercially available sublingual immunotherapy extracts has been reported as 0.02 to 0.03% vs near 0.1% with subcutaneous immunotherapy (SCIT) (3).
Oral immunotherapy for peanut allergy uses defatted peanut flour. Dose escalation is done using 5 incremental doses from 0.5 mg to 6 mg over one day given in a health care setting. This initial regimen is followed by a daily dose starting at 3 mg and increasing by 50 to 100% every 2 weeks over 22 weeks before reaching the maintenance dose of 300 mg once a day. Each increase in dose is given in a health care setting. If the initial dose is tolerated, subsequent doses are taken daily for 2 weeks; they can be taken at home. After patients successfully tolerate the 300-mg dose in a health care setting, they must take the 300-mg daily dose indefinitely to maintain desensitization.
Allergy treatment during pregnancy and breastfeeding
For pregnant women with environmental allergies and sinopulmonary symptoms, avoidance of the allergen is the best way to control symptoms. If symptoms are severe, an antihistamine intranasal spray is recommended. An oral antihistamine should be used only if antihistamine intranasal sprays are inadequate.
During breastfeeding, nonsedating antihistamines are preferred. Sedating antihistamines can be used, but they may cause drowsiness and irritability in the infant. If a sedating antihistamine is required, the infant should be monitored for these effects.
Antihistamine intranasal sprays are preferred to oral antihistamines. If oral antihistamines are essential for controlling symptoms, they should be taken immediately after breastfeeding. Cyproheptadine is contraindicated during breastfeeding because it lowers prolactin levels and thus may reduce lactation.
Treatment references
1. Alghamdi R, Alshaier R, Alotaibi A, et al: Immunotherapy Effectiveness in Treating Peanut Hypersensitivity: A Systemic Review. Cureus 14(2):e21832, 2022. doi:10.7759/cureus.21832
2. Brennan PJ, Rodriguez Bouza T, Hsu FI, Sloane DE, Castells MC: Hypersensitivity reactions to mAbs: 105 desensitizations in 23 patients, from evaluation to treatment. J Allergy Clin Immunol 124(6):1259–1266, 2009. doi:10.1016/j.jaci.2009.09.009
3. Zeiger RS, Schatz M, Pomichowski ME, et al: Real-world assessment of anaphylaxis and eosinophilic esophagitis with 12 SQ house dust mite SLIT-tablet sublingual immunotherapy. J Allergy Clin Immunol Glob 3(3):100250, 2024. doi:10.1016/j.jacig.2024.100250
Prevention of Allergic and Atopic Disorders
Allergic triggers should be removed or avoided. Strategies include the following:
Removing items that collect dust, such as knickknacks, magazines, books, and soft toys
Using synthetic fiber pillows and impermeable mattress covers
Frequently washing bed sheets, pillowcases, and blankets in hot water
Frequently cleaning the house, including dusting, vacuuming, and wet-mopping
Removing upholstered furniture and carpets or frequently vacuuming upholstered furniture and carpets
Replacing draperies and shades with blinds
Exterminating cockroaches to eliminate exposure
Using dehumidifiers in basements and other poorly aerated, damp rooms
Using high-efficiency particulate air (HEPA) vacuums and filters
Avoiding food or medication triggers
Limiting pets to certain rooms or keeping them out of the house
For people with severe seasonal allergies, possibly moving to an area that does not have the allergen
Adjunctive nonallergenic triggers (eg, cigarette smoke, strong odors, irritating fumes, air pollution, cold temperatures, high humidity) should also be avoided or controlled when possible.
Key Points
Atopic reactions (commonly caused by mite feces, animal dander, pollen, or mold) are IgE-mediated allergic reactions that trigger histamine release.
Take a thorough history, including a detailed description of the frequency and duration of attacks, relationship of symptoms to seasons or situations, family history, possible triggers, and responses to attempted treatments because history is more reliable than testing.
When the history and examination do not identify the cause, skin tests or an allergen-specific serum IgE test may help identify the allergen.
Eliminating or avoiding the allergen is key to treatment and prevention; to relieve symptoms, use H1 blockers, topical corticosteroids, and/or mast cell stabilizers.
If the allergen cannot be avoided and other treatments are ineffective, immunotherapy may be needed.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Academy of Allergy, Asthma and Immunology: This site provides general information about allergic disorders for clinicians in the US, information about educational opportunities, and information for patients
European Academy of Allergy and Clinical Immunology: This site promotes both basic and clinical research into allergic disorders, provides clinicians with a central location to seek out information and contacts, and provides resources for patients







