



Topic Resources

The immune system consists of cellular components and molecular components that work together to destroy antigens (Ags). (See also Overview of the Immune System.)
Acute Phase Reactants
Acute phase reactants are plasma proteins whose levels change in response to the elevated circulating levels of interleukin (IL)-1 and IL-6 that accompany infection or tissue damage.
Positive acute phase reactants dramatically increase
Negative acute phase reactants decrease
Most dramatically increased are:
C-reactive protein (CRP)
Serum amyloid A
Other acute phase reactants include:
Mannose-binding lectin
Serum amyloid P component
Alpha-1 acid glycoprotein
Fibrinogen
C-reactive protein, mannose-binding lectin, and serum amyloid P component activate complement and act as opsonins (substances that bind to microorganisms rendering them susceptible to phagocytosis). Serum amyloid A and alpha-1 acid glycoprotein are transport proteins, and fibrinogen is a coagulation factor. Elevated C-reactive protein levels are a nonspecific indicator of infection or inflammation. Increased fibrinogen levels are the main reason the erythrocyte sedimentation rate (ESR) is elevated in acute inflammation.
Many acute phase reactants are made in the liver. Collectively, they may help limit tissue injury, enhance host resistance to infection, and promote tissue repair and resolution of inflammation. The acute phase reaction may also be activated by cytokines released from visceral adipocytes, which may in part explain the link between obesity, inflammation, and cardiovascular disease.
Antibodies
Antibodies act as the antigen receptor on the surface of B cells and, in response to antigen, are subsequently secreted by plasma cells. Antibodies recognize specific configurations (epitopes, or antigenic determinants) on the surfaces of antigens (eg, proteins, polysaccharides, nucleic acids). Antibodies and antigens fit tightly together because their shape and other surface properties (eg, charge) are complementary. The same antibody molecule can cross-react with related antigens if their epitopes are similar enough to those of the original antigen.
Antibody structure
Antibodies consist of 4 polypeptide chains (2 identical heavy chains and 2 identical light chains) joined by disulfide bonds to produce a Y configuration (see figure B-cell Receptor). The heavy and light chains are divided into a variable (V) region and a constant (C) region.
B-cell Receptor
The B-cell receptor consists of an Ig molecule anchored to the cell’s surface. CH = heavy chain constant region; CL = light chain constant region; Fab = antigen-binding fragment; Fc = crystallizable fragment; Ig = immunoglobulin; L-kappa (κ) or lambda (λ) = 2 types of light chains; VH = heavy chain variable region; VL = light chain variable region. |

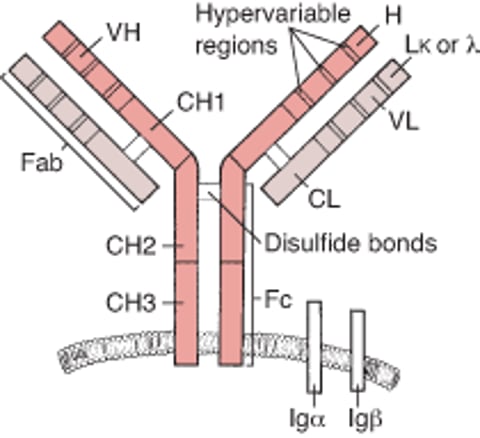
V regions are located at the amino-terminal ends of the Y arms; they are called variable because the amino acids they contain are different in different antibodies. Within the V regions, hypervariable regions determine the specificity of the immunoglobulin (Ig). They also function as antigens (idiotypic determinants) to which certain natural (anti-idiotype) antibodies can bind; this binding may help regulate B-cell responses.
The C region of the heavy chains contains a relatively constant sequence of amino acids (isotype) that is distinctive for each Ig class. A B cell can change the isotype it produces and thus switch the class of Ig it produces. Because the Ig retains the variable part of the heavy chain V region and the entire light chain, it retains its antigenic specificity.
The amino-terminal (variable) end of the antibody binds to antigen to form an antibody-antigen complex. The antigen-binding (Fab) portion of Ig consists of a light chain and part of a heavy chain and contains the V region of the Ig molecule (ie, the combining sites). The crystallizable fragment (Fc) contains most of the C region of the heavy chains; Fc is responsible for complement activation and binds to Fc receptors on cells.
Antibody classes
Antibodies are divided into 5 classes:
IgM
IgG
IgA
IgD
IgE
The classes are defined by their type of heavy chain:
Mu (μ) for IgM
Gamma (γ) for IgG
Alpha (α) for IgA
Epsilon (ε) for IgE
Delta (δ) for IgD
There are also 2 types of light chains:
Kappa (κ)
Lambda (λ)
Each of the 5 Ig classes can bear either kappa or lambda light chains.
IgM is the first antibody formed after exposure to new antigen. It has 5 Y-shaped molecules (10 heavy chains and 10 light chains), linked by a single joining (J) chain. IgM circulates primarily in the intravascular space; it complexes with and agglutinates antigens and can activate complement, thereby facilitating phagocytosis. Isohemagglutinins are predominantly IgM. Monomeric IgM acts as a surface antigen receptor on B cells. Patients with hyper-IgM syndrome have a defect in the genes involved in antibody class switching (eg, genes that encode CD40, CD154 [also known as CD40L], AID [activation-induced cytidine deaminase], UNG [uracil-DNA-glycosylase], or NEMO [nuclear factor–kappa-B essential modulator]); therefore, IgA, IgG, and IgE levels are low or absent, and levels of circulating IgM are often high.
IgG is the most prevalent Ig isotype in serum and is present in intravascular and extravascular spaces. It coats antigen to activate complement and facilitate phagocytosis by neutrophils and macrophages. IgG is the primary circulating Ig produced after re-exposure to antigen (secondary immune response) and is the predominant isotype contained in commercial gamma-globulin products. IgG protects against bacteria, viruses, and toxins. It is the only Ig isotype that crosses the placenta; therefore, this class of antibody is important for protecting neonates. However, pathogenic IgG antibodies (eg, anti-Rh0[D] antibodies, anti-SSA antibodies [anti–Sjögren-syndrome A-related antigen], and stimulatory anti-thyroid-stimulating hormone receptor autoantibodies), if present in the mother, can potentially cause significant disease in the fetus.
There are 4 subclasses of IgG: IgG1, IgG2, IgG3, and IgG4. They are numbered in descending order of serum concentration. IgG subclasses differ functionally mainly in their ability to activate complement; IgG1 and IgG3 are most efficient, IgG2 is less efficient, and IgG4 is inefficient. IgG1 and IgG3 are efficient mediators of antibody-dependent cellular cytotoxicity; IgG4 and IgG2 are less so. IgG4-generating cells increase in IgG4 related disease.
IgA occurs at mucosal surfaces, in serum, and in secretions (saliva; tears; respiratory, genitourinary, and gastrointestinal tract secretions; colostrum), where it provides an early antibacterial and antiviral defense. J chain links IgA into a dimer to form secretory IgA. Secretory IgA is synthesized by plasma cells in the subepithelial regions of the gastrointestinal and respiratory tracts. Selective IgA deficiency is relatively common but often has little clinical impact because there is cross-functionality with other classes of antibody.
IgD is coexpressed with IgM on the surface of naive B cells. Whether these 2 classes function differently on the surface of the B cell and, if so, how differently is somewhat unclear. Serum IgD levels are very low, and any unique function of circulating IgD is largely unknown, although there is some evidence for an immunoregulatory role on Th2 responses (1) (see table Functions of T Cells).
IgE is present in low levels in serum and in respiratory and gastrointestinal mucous secretions. IgE binds with a strong affinity to receptors present in high levels on mast cells and basophils and to a lesser extent on several other hematopoietic cells, including dendritic cells. If antigen bridges 2 IgE molecules bound to the mast cell or basophil surface, the cells degranulate, releasing chemical mediators that cause an inflammatory response. IgE levels are elevated in atopic disorders (eg, allergic or extrinsic asthma, hay fever, atopic dermatitis) and parasitic infections.
Antibodies reference
1. Shan M, Carrillo J, Yeste A, et al. Secreted IgD Amplifies Humoral T Helper 2 Cell Responses by Binding Basophils via Galectin-9 and CD44. Immunity 2018;49(4):709-724.e8. doi:10.1016/j.immuni.2018.08.013
Cytokines
Cytokines are polypeptides secreted by immune and other cells when the cell interacts with a specific antigen, with pathogen-associated molecules such as endotoxin, or with other cytokines. Main categories include
Chemokines
Colony-stimulating factors (CSFs)
Interferons (IFNs)
Interleukins (ILs)
Transforming growth factors (TGFs)
Tumor necrosis factors (TNFs)
Although lymphocyte interaction with a specific antigen triggers cytokine secretion, cytokines themselves are not antigen-specific; thus, they bridge innate and acquired immunity and generally influence the magnitude of inflammatory or immune responses. They act sequentially, synergistically, or antagonistically. They may act in an autocrine or paracrine manner.
Cytokines deliver their signals via cell surface receptors. For example, the IL-2 receptor consists of 3 chains: alpha (α), beta (β), and gamma (γ). The receptor’s affinity for IL-2 is
High if all 3 chains are expressed
Intermediate if only the beta and gamma chains are expressed
Low if only the alpha chain is expressed
Mutations or deletion of the gamma chain is the basis for X-linked severe combined immunodeficiency.
Chemokines
Chemokines induce chemotaxis and migration of leukocytes. There is a large family of chemokines with at least 47 members, which comprise 4 subsets (C, CC, CXC, CX3C), defined by the number and spacing of their amino terminal cysteine residues. Chemokine receptors (CCR5 on memory T cells, monocytes/macrophages, and dendritic cells; CXCR4 on resting T cells) act as co-receptors for entry of HIV into cells. CXCR4 antagonists may have utility in combination therapies for pancreatic ductal adenocarcinoma.
Colony-stimulating factors
Granulocyte-colony stimulating factor (G-CSF) is produced by endothelial cells and fibroblasts.
The main effect of G-CSF is
Stimulation of growth of neutrophil precursors
Clinical uses of G-CSF include
Reversal of neutropenia after chemotherapy, radiation therapy, or both
Granulocyte-macrophage colony stimulating factor (GM-CSF) is produced by endothelial cells, fibroblasts, macrophages, mast cells, and T helper (Th) cells.
The main effects of GM-CSF are
Stimulation of growth of monocyte, neutrophil, eosinophil, and basophil precursors
Activation of macrophages
Clinical uses of GM-CSF include
Reversal of neutropenia after chemotherapy, radiation therapy, or both
The development of autoantibodies against GM-CSF can result in alveolar proteinosis.
Macrophage colony stimulating factor (M-CSF) is produced by endothelial cells, epithelial cells, and fibroblasts.
The main effect of M-CSF is
Stimulation of growth of monocyte precursors
Clinical uses of M-CSF include
Therapeutic potential for stimulating tissue repair
Interferons (IFNs)
Interferons are a family of proteins that have antiviral activity and also act as immune modulators. Evidence for excess interferon activity is a feature of patients with systemic lupus erythematosus (1).
IFN-alpha is produced by leukocytes.
The main effects of IFN-alpha are
Inhibition of viral replication
Augmentation of class I major histocompatibility complex (MHC) expression
Clinical uses of IFN-alpha include
Treatment of chronic hepatitis B, chronic hepatitis C, AIDS-related Kaposi sarcoma, condylomata acuminata, hairy cell leukemia, chronic myeloid leukemia, follicular lymphoma, and metastatic melanoma
IFN-beta is produced by fibroblasts.
The main effects of IFN-beta are
Inhibition of viral replication
Augmentation of class I MHC expression
Clinical uses of IFN-beta include
Reduction of the number of flare-ups in relapsing multiple sclerosis
IFN-gamma is produced by natural killer (NK) cells, cytotoxic type 1 (Tc1) cells, and T helper type 1 (Th1) cells.
The main effects of IFN-gamma are
Inhibition of viral replication
Augmentation of classes I and II MHC and of Fc receptor expression
Activation of macrophages and NK cells
Antagonism of several actions of IL-4
Inhibition of Th2 cell proliferation
Clinical uses of IFN-gamma include
Control of infection in chronic granulomatous disease
Delay of progression in severe malignant osteopetrosis
Interleukins (ILs)
Interleukins (IL-1 to IL-38) are collectively produced by a wide variety of cells and have multiple effects on cell development and the regulation of immune responses. Interleukins that have been particularly well characterized and investigated for clinical relevance include:
IL-1 (alpha and beta) is produced by B cells, dendritic cells, endothelium, macrophages, monocytes, and natural killer (NK) cells.
The main effects of IL-1 are
Costimulation of T-cell activation by enhancing production of cytokines (eg, IL-2 and its receptor)
Enhancement of B-cell proliferation and maturation
Enhancement of NK-cell cytotoxicity
Induction of IL-1, IL-6, IL-8, TNF, GM-CSF, and prostaglandin E2 production by macrophages
Proinflammatory activity by inducing chemokines, intercellular adhesion molecule 1 (ICAM-1), and vascular cell adhesion molecule 1 (VCAM-1) on endothelium
Induction of sleep, anorexia, release of tissue factor, acute phase reactants, and bone resorption by osteoclasts
Endogenous pyrogenic activity
Clinical relevance of IL-1 includes
For anti–IL-1 beta monoclonal antibody (mAb), treatment of periodic fever syndromes, systemic juvenile idiopathic arthritis, acute gout, and calcium pyrophosphate arthritis (pseudogout)
For IL-1 receptor antagonist (IL-1RA), treatment of adults with moderate to severe rheumatoid arthritis and patients with neonatal-onset multisystem inflammatory disease (NOMID)
IL-2 is produced by Th1 cells.
The main effects of IL-2 are
Induction of activated T-cell and B-cell proliferation
Enhancement of NK-cell cytotoxicity and killing of tumor cells and bacteria by monocytes and macrophages
Clinical relevance of IL-2 includes
For IL-2, treatment of metastatic renal cell carcinoma and metastatic melanoma
For anti-IL-2 receptor mAb, help with prevention of acute kidney rejection
IL-3 (also known as multi-CSF) is produced by T cells and mast cells
The main effects of IL-3 are
Stimulation of growth and differentiation of hematopoietic precursors
Stimulation of mast cell growth
Clinical relevance of IL-3 includes
Targeting of IL-3 receptor alpha chain with monoclonal antibodies or chimeric antigen receptor (CAR) T cells, which may be of benefit in patients with certain disorders, often hematogenous cancers such as relapsed refractory acute myeloid leukemia
IL-4 is produced by mast cells, NK cells, natural killer T (NKT) cells, gamma-delta T cells, Tc2 cells, and Th2 cells.
The main effects of IL-4 are
Induction of Th2 cells
Stimulation of activated B-cell, T-cell, and mast cell proliferation
Upregulation of class II MHC molecules on B cells and on macrophages and CD23 on B cells
Downregulation of IL-12 production, thereby inhibiting Th1 cell-differentiation
Augmentation of macrophage phagocytosis
Induction of switch to IgG1 and IgE
Clinical relevance of IL-4 includes
Involvement of IL-4 (with IL-13) in the production of IgE in atopic allergy
For anti-IL-4 receptor mAb, treatment of patients with moderate to severe atopic dermatitis
IL-5 is produced by mast cells and Th2 cells.
The main effects of IL-5 are
Induction of eosinophil and activated B-cell proliferation
Induction of switch to IgA
Clinical relevance of IL-5 includes
For anti–IL-5 mAb, treatment of patients with severe eosinophilic asthma and eosinophilic granulomatosis with polyangiitis
For anti-IL-5 receptor mAb, treatment of patients with severe eosinophilic asthma
IL-6 is produced by dendritic cells, fibroblasts, macrophages, monocytes, and Th2 cells.
The main effects of IL-6 are
Induction of differentiation of B cells into plasma cells and differentiation of myeloid stem cells
Induction of acute phase reactants
Enhancement of T-cell proliferation
Induction of Tc-cell differentiation
Pyrogenic activity
Clinical relevance of IL-6 includes
For anti–IL-6 mAb, treatment of multicentric Castleman disease in patients who are negative for HIV and human herpesvirus 8 (HHV-8)
For anti–IL-6 receptor mAb, treatment of rheumatoid arthritis when the response to TNF-antagonists is inadequate and treatment of juvenile idiopathic arthritis, giant cell arteritis, and of severe cytokine release syndrome following CAR T cell treatment. In combination with dexamethasone, treatment of patients with following CAR T cell treatment. In combination with dexamethasone, treatment of patients withCOVID-19 with hypoxia and systemic inflammation.
IL-7 is produced by bone marrow and thymus stromal cells.
The main effects of IL-7 are
Induction of differentiation of lymphoid stem cells into T-cell and B-cell precursors
Activation of mature T cells
Clinical relevance of IL-7 includes
Potential immunostimulation in the treatment of viral infections, cancer, and lymphopenic sepsis
IL-8 (a chemokine) is produced by endothelial cells, macrophages, and monocytes.
The main effect of IL-8 is
Mediation of chemotaxis and activation of neutrophils
Clinical relevance of IL-8 includes
For IL-8 antagonists, potential for the treatment of chronic inflammatory disorders
IL-9 is produced by Th cells.
The main effects of IL-9 are
Induction of thymocyte proliferation
Enhancement of mast cell growth
Synergistic action with IL-4 to induce switch to IgG1 and IgE
Clinical trials of anti-IL-9 mAb in asthma have generally failed to demonstrate efficacy (2).
IL-10 is produced by B cells, macrophages, monocytes, Tc cells, Th2 cells, and regulatory T cells.
The main effects of IL-10 are
Inhibition of IL-2 secretion by Th1 cells
Downregulation of production of class II MHC molecules and cytokines (eg, IL-12) by monocytes, macrophages, and dendritic cells, thereby inhibiting Th1-cell differentiation
Inhibition of T-cell proliferation
Enhancement of B-cell differentiation
Clinical relevance of IL-10 includes
Possible suppression of pathogenic immune response in allergy and autoimmune disorders
IL-11 is produced by bone marrow stromal cells
The main effects of IL-11 are
Promotion of pro-B cell and megakaryocyte differentiation
Induction of acute phase reactants
Clinical relevance of IL-11 includes
Prevention of thrombocytopenia after myelosuppressive chemotherapy
IL-12 is produced by B cells, dendritic cells, macrophages, and monocytes.
The main effects of IL-12 are
A critical role in Th1 differentiation
Induction of proliferation of Th1 cells, CD8 T cells, gamma-delta T cells, and NK cells and their production of IFN-gamma
Enhancement of NK and CD8 T-cell cytotoxicity
Clinical relevance of IL-12 includes
For anti–IL-12 mAb, treatment of plaque psoriasis and psoriatic arthritis
IL-13 is produced by mast cells and Th2 cells.
The main effects of IL-13 are
Inhibition of activation and cytokine secretion by macrophages
Coactivation of B-cell proliferation
Upregulation of class II MHC molecules and CD23 on B cells and monocytes
Induction of switch to IgG1 and IgE
Induction of vascular cell adhesion molecule 1 (VCAM-1) on endothelium
Clinical relevance of IL-13 includes
Involvement of IL-13 (with IL-4) in the production of IgE in atopic allergy
IL-15 is produced by B cells, dendritic cells, macrophages, monocytes, NK cells, and T cells.
The main effects of IL-15 are
Induction of proliferation of T cells, NK cells, and activated B cells
Induction of cytokine production and cytotoxicity of NK cells and CD8 T cells
Chemotactic activity for T cells
Stimulation of intestinal epithelium growth
Clinical relevance of IL-15 includes
Potential as an immunostimulatory agent in the treatment of cancer
IL-16 is produced by helper T cells and cytotoxic T cells
The main effects of IL-16 are
Chemotactic activity for CD4 T cells, monocytes, and eosinophils
Induction of MHC class II molecules
Clinical relevance of IL-16 includes
Potential to promote CD4 T cell reconstitution in patients with HIV infection
IL-16 antagonists may have utility in allergic and autoimmune conditions
IL-17 (A and F) is produced by Th17 cells, gamma-delta T cells, NKT cells, and macrophages.
The main effects of IL-17 are
Proinflammatory action
Stimulation of production of cytokines (eg, TNF, IL-1 beta, IL-6, IL-8, G-CSF)
Clinical relevance of IL-17 includes
For anti-IL-17A mAb, treatment of adults with active ankylosing spondylitis, active psoriatic arthritis, or moderate to severe plaque psoriasis, but inhibition may trigger inflammatory bowel disease
IL-18 is produced by monocytes, macrophages, and dendritic cells.
The main effects of IL-18 are
Induction of IFN-gamma production by T cells
Enhancement of NK-cell cytotoxicity
IL-18 has been investigated as an immunotherapeutic agent in cancer, but efficacy has not been established.
IL-20 is produced by monocytes, macrophages, and dendritic cells.
The main effects of IL-20 are
Proinflammatory action
Stimulation of keratinocyte proliferation
Clinical relevance of IL-20 includes
Receptor for IL-20 is upregulated on keratinocytes in patients with psoriasis
IL-21 is produced by NKT cells and Th cells.
The main effects of IL-21 are
Stimulation of B-cell proliferation after CD40 cross-linking
Stimulation of NK cells
Costimulation of T cells
Stimulation of bone marrow precursor cell proliferation
Clinical relevance of IL-21 includes
In clinical trials, stimulation of cytotoxic T-cells and NK cells in cancer
For IL-21 antagonists, potential in the treatment of autoimmune disorders
IL-22 is produced by NK cells, Th17 cells, and gamma-delta T cells.
The main effects of IL-22 are
Proinflammatory activity
Induction of acute phase reactant synthesis
Clinical relevance of IL-22 includes
For IL-22 antagonists, potential in the treatment of autoimmune disorders
IL-23 is produced by dendritic cells and macrophages.
The main effect of IL-23 is
Induction of Th-cell proliferation
Clinical relevance of IL-23 includes
For anti–IL-23 mAb, treatment of plaque psoriasis, psoriatic arthritis, and Crohn disease
IL-24 is produced by B cells, macrophages, monocytes, and T cells.
The main effects of IL-24 are
Suppression of tumor cell growth
Induction of apoptosis in tumor cells
Clinical relevance of IL-24 includes
Potential in the treatment of cancer
IL-25 (also called IL-17E) is produced by T cells, macrophages, dendritic cells, mast cells, eosinophils and epithelium.
The main effect of IL-25 is
Stimulation of Th2 cells
Clinical relevance of IL-25 includes
Implicated in the development of allergy and autoimmune disorders (3)
IL-27 is produced by dendritic cells, monocytes, and macrophages.
The main effect of IL-27 is
Induction of Th1 cells
Clinical relevance of IL-27 includes
Potential in the treatment of cancer
IL-31 is produced by Th2 cells
The main effect of IL-31 is
Proinflammatory activity
Clinical relevance of IL-31 includes
Role in atopic dermatitis, asthma, and inflammatory bowel disease
IL-32 is produced by NK cells and T cells.
The main effects of IL-32 are
Proinflammatory activity
Participation in activation-induced T cell apoptosis
Clinical relevance of IL-32 includes
Potential in the treatment of autoimmune disorders
IL-33 is produced by endothelial cells, stromal cells, and dendritic cells.
The main effects of IL-33 are
Induction of Th2 cytokines
Promotion of eosinophilia
Clinical relevance of IL-33 includes
For IL-33 antagonists, potential in the treatment of asthma
IL-34 is produced by keratinocytes and neurons.
The main effects of IL-34 are
Supporting cell growth and survival of monocytes
Stimulation of monocyte differentiation into macrophages
Clinical relevance of IL-34 includes
Possible involvement in the pathogenesis of rheumatoid arthritis (4) and inflammatory bowel disease
IL-35 is produced by regulatory T cells, macrophages, and dendritic cells.
The main effect of IL-35 is
Suppression of inflammation, eg, by inducing regulatory T cells and B cells and inhibiting Th17 cells
Clinical relevance of IL-35 includes
Potential to suppress pathogenic immune responses in allergy and autoimmune disorders
IL-36 is produced by epithelium, monocytes, macrophages, dendritic cells, and T cells.
The main effect of IL-36
Proinflammatory activity
Clinical relevance of IL-36 includes
Promotes inflammation in psoriasis
IL-37 is produced by macrophages and inflamed tissue.
The main effects of IL-37 are
Anti-inflammatory
Possible IL-18 receptor antagonist
Clinical relevance of IL-37 includes
Potential to block inflammation
Transforming growth factors (TGF)
There are alpha and beta forms of TGFs with 3 TGF-beta subtypes.
TGF-alpha is produced by epithelial cells, monocytes, macrophages, brain cells, and keratinocytes.
The main effects of TGF-alpha are
Stimulation of cell proliferation and differentiation
Regulation of mucus production
Inhibition of gastric acid secretion
Clinical relevance of TGF-alpha includes
TGF-alpha antagonists alleviate symptoms in Menetrier disease
TGF-beta is produced by B cells, macrophages, mast cells, and Th3 cells.
The main effects of the TGF-beta family are
Proinflammatory activity (eg, by chemoattraction of monocytes and macrophages) but also anti-inflammatory activity (eg, by inhibiting lymphocyte proliferation)
Induction of switch to IgA
Promotion of tissue repair and fibrosis
Clinical relevance of TGF-beta includes
Trials of antagonists (eg, antisense oligonucleotides) in cancer are ongoing (5).
Tumor necrosis factors (TNFs)
TNF-alpha (cachectin) is produced by B cells, dendritic cells, macrophages, mast cells, monocytes, NK cells, and Th cells.
The main effects of TNF-alpha include
Cachexia
Induction of secretion of several cytokines (eg, IL-1, GM-CSF, IFN-gamma) that stimulate inflammation
Induction of E-selectin on endothelium
Activation of macrophages
Antiviral activity
Cytotoxicity to tumor cells
Clinical relevance of TNF-alpha includes
For TNF-alpha antagonists (mAb or soluble receptor), treatment of rheumatoid arthritis, plaque psoriasis, Crohn disease refractory to standard treatments, ulcerative colitis, hidradenitis suppurativa, ankylosing spondylitis, psoriatic arthritis, polyarticular juvenile idiopathic arthritis, noninfectious intermediate uveitis, posterior uveitis, and panuveitis. Despite its name, blocking the activity of TNF does not lead to a marked increase in primary or secondary cancers.
TNF-beta (lymphotoxin) is produced by Tc cells and Th1 cells.
The main effects of TNF-beta include
Cytotoxicity to tumor cells
Antiviral activity
Enhancement of phagocytosis by neutrophils and macrophages
Involvement in lymphoid organ development
Clinical relevance of TNF-beta includes
For TNF-beta antagonists, similar effects to well-established TNF-alpha antagonists but have not been shown to be superior
Cytokines references
1. Tanaka Y, Kusuda M, Yamaguchi Y. Interferons and systemic lupus erythematosus: Pathogenesis, clinical features, and treatments in interferon-driven disease. Mod Rheumatol 2023;33(5):857-867. doi:10.1093/mr/roac140
2. Oh CK, Leigh R, McLaurin KK, Kim K, Hultquist M, Molfino NA. A randomized, controlled trial to evaluate the effect of an anti-interleukin-9 monoclonal antibody in adults with uncontrolled asthma. Respir Res 2013;14(1):93. Published 2013 Sep 19. doi:10.1186/1465-9921-14-93
3. Liu Y, Shao Z, Shangguan G, Bie Q, Zhang B. Biological Properties and the Role of IL-25 in Disease Pathogenesis. J Immunol Res 2018;2018:6519465. Published 2018 Sep 23. doi:10.1155/2018/6519465
4. Zhou RP, Wu XS, Xie YY, et al. Functions of interleukin-34 and its emerging association with rheumatoid arthritis. Immunology 2016;149(4):362-373. doi:10.1111/imm.12660
5. Lee HJ. Recent Advances in the Development of TGF-β Signaling Inhibitors for Anticancer Therapy. J Cancer Prev 2020;25(4):213-222. doi:10.15430/JCP.2020.25.4.213







