


Staphylococci are gram-positive aerobic organisms. Staphylococcus aureus is the most pathogenic; it typically causes skin infections and sometimes pneumonia, endocarditis, and osteomyelitis. It commonly leads to abscess formation. Some strains elaborate toxins that cause gastroenteritis, scalded skin syndrome, and toxic shock syndrome. Diagnosis is by Gram stain and culture. Treatment is usually with penicillinase-resistant beta-lactams, but because antibiotic resistance is common, vancomycin or other newer antibiotics may be required.


The ability to clot blood by producing coagulase distinguishes the virulent pathogen, Staphylococcus aureus, from the less virulent coagulase-negative staphylococcal species. Coagulase-positive S. aureus is among the most ubiquitous and dangerous human pathogens, for both its virulence and its ability to develop antibiotic resistance.
Coagulase-negative species such as S. epidermidis are increasingly associated with hospital-acquired infections; S. saprophyticus causes urinary infections. S. lugdunensis, a coagulase-negative species, can cause invasive disease with virulence similar to that of S. aureus. Unlike most coagulase-negative staphylococcal species, S. lugdunensis often remains sensitive to penicillinase-resistant beta-lactam antibiotics (ie, methicillin-sensitive).
A carrier state is common. Pathogenic staphylococci are ubiquitous. They are carried, usually transiently, in the anterior nares of about 30% of healthy adults and on the skin of about 20%; from these locations, staphylococci can cause infection in the host and others. Carriage rates are higher in hospitalized patients and hospital personnel. S. aureus infections are more prevalent in carriers than in noncarriers and are usually caused by the colonizing strain.
Risk factors for staphylococcal infections
People who are predisposed to staphylococcal infections include
Neonates and breastfeeding mothers
Patients with influenza, chronic bronchopulmonary disorders (eg, cystic fibrosis, emphysema), leukemia, tumors, chronic skin disorders, or diabetes mellitus
Patients with a transplant, an implanted prosthesis, other foreign bodies, or an indwelling intravascular plastic catheter
Patients receiving adrenal steroids, irradiation, immunosuppressants, or antitumor chemotherapy
Injection drug users
Patients who have chronic kidney disease and are being treated with dialysis
Patients with surgical incisions, open wounds, or burns
Predisposed patients may acquire antibiotic-resistant staphylococci from other patients, health care personnel, or inanimate objects in health care settings. Transmission via the hands of personnel is the most common means of spread, but airborne spread also can occur.
Diseases Caused by Staphylococci
Staphylococci cause disease by
Direct tissue invasion
Sometimes exotoxin production
Direct tissue invasion is the most common mechanism for staphylococcal disease, including the following:
Multiple exotoxins are sometimes produced by staphylococci. Some have local effects; others trigger cytokine release from certain T cells, causing serious systemic effects (eg, skin lesions, shock, organ failure, death). Panton-Valentine leukocidin (PVL) is a toxin produced by strains infected with a certain bacteriophage. PVL is typically present in strains of community-associated methicillin-resistant S. aureus (CA-MRSA) and has been thought to mediate the ability to necrotize; however, this effect has not been verified.
Toxin-mediated staphylococcal diseases include the following:
The infections and disorders listed below are further discussed elsewhere in THE MANUAL.
Staphylococcal bacteremia
S. aureus bacteremia, which frequently causes metastatic foci of infection, may occur with any localized S. aureus infection but is particularly common with infection related to intravascular catheters or other foreign bodies. It may also occur without any obvious primary site.
S. epidermidis and other coagulase-negative staphylococci increasingly cause hospital-acquired bacteremia associated with intravascular catheters and other foreign bodies because they can form biofilms on these materials.
Staphylococcal bacteremia is an important cause of morbidity (especially prolongation of hospitalization) and mortality in debilitated patients.
Staphylococcal skin infections
Skin infections are the most common form of staphylococcal disease. Superficial infections may be diffuse, with vesicular pustules and crusting (impetigo) or sometimes cellulitis, or focal with nodular abscesses (furuncles and carbuncles). Deeper cutaneous abscesses are common. Severe necrotizing skin infections may occur.


In impetigo, clusters of vesicopustular or bullous lesions form, rupture, and develop a honey-colored crust.
Image courtesy of Thomas Habif, MD.


This photo shows clusters of vesicles and pustules with developing honey-colored crust on the nose.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY


Furuncles (boils) are tender nodules or pustules that involve a hair follicle and are caused by staphylococcal infection.
Image provided by Thomas Habif, MD.
In impetigo, clusters of vesicopustular or bullous lesions form, rupture, and develop a honey-colored crust.
Image courtesy of Thomas Habif, MD.
This photo shows clusters of vesicles and pustules with developing honey-colored crust on the nose.
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
Furuncles (boils) are tender nodules or pustules that involve a hair follicle and are caused by staphylococcal infection.
Image provided by Thomas Habif, MD.
Staphylococci are commonly implicated in wound and burn infections, postoperative incision infections, and mastitis or breast abscess in breastfeeding mothers.
Staphylococcal neonatal infections
Neonatal infections usually appear within 4 weeks after birth and include
Skin lesions with or without exfoliation
Staphylococcal pneumonia
Pneumonia that occurs in a community setting is not common but may develop in patients with one or more of the following characteristics:
Influenza
Chronic bronchopulmonary or other high-risk diseases
Corticosteroid or immunosuppressant therapy
Indwelling IV catheters for home parenteral therapy or hemodialysis
Injection drug use
Staphylococcal pneumonia may be a primary infection or result from hematogenous spread of S. aureus infection elsewhere in the body (eg, IV catheter infection, endocarditis, soft-tissue infection) or from injection drug use. However, S. aureus is a common cause of hospital-acquired pneumonia, including ventilator-associated pneumonia.
Staphylococcal pneumonia is occasionally characterized by formation of lung abscesses followed by rapid development of pneumatoceles and empyema. CA-MRSA often causes severe necrotizing pneumonia.
Staphylococcal endocarditis
Endocarditis can develop, particularly in people who use injection drugs and patients with prosthetic heart valves. Because intravascular catheter use and implantation of cardiac devices have increased, S. aureus has become a leading cause of bacterial endocarditis.
S. aureus endocarditis is an acute febrile illness often accompanied by visceral abscesses, embolic phenomena, pericarditis, subungual petechiae, subconjunctival hemorrhage, purpuric lesions, heart murmurs, perivalvular abscess, conduction defects, and heart failure secondary to cardiac valve damage.
Staphylococcal osteomyelitis
Osteomyelitis occurs more commonly in children, causing chills, fever, and pain over the involved bone. Subsequently, the overlying soft tissue becomes red and swollen. Articular infection may occur; it frequently results in effusion, suggesting septic arthritis rather than osteomyelitis. Most infections of the vertebrae and intervertebral disks in adults involve S. aureus.
Staphylococcal infectious arthritis
Joints typically become infected via hematogenous infection, but infection can also be caused by extension of a bone infection, trauma, or direct infection during joint surgery. Prosthetic joints are particularly prone to infection. Staphylococcal infection of a prosthetic joint in the months after implantation is usually acquired during surgery, whereas infections occurring more than 12 months after surgery are likely due to hematogenous spread. However, infections still may be secondary to organisms that were inadvertently introduced at the time of implantation and remained dormant and then became clinically evident several months later.
Staphylococcal toxic shock syndrome
Staphylococcal toxic shock syndrome may result from use of vaginal tampons or other devices or complicate any type of S. aureus infection (eg, postoperative wound infection, infection of a burn, skin infection). Although most cases have been due to methicillin-susceptible S. aureus (MSSA), cases due to MRSA are becoming more frequent.
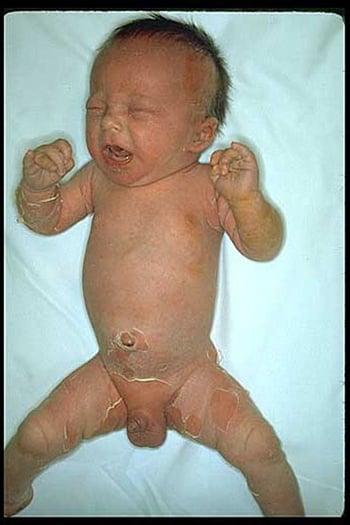
Staphylococcal scalded skin syndrome
Staphylococcal scalded skin syndrome, which is caused by several toxins termed exfoliatins, is an exfoliative dermatitis of childhood characterized by large bullae and peeling of the upper layer of skin. Eventually, exfoliation occurs. Scalded skin syndrome most commonly occurs in infants and children < 5 years.

Staphylococcal food poisoning
Staphylococcal food poisoning is caused by ingesting a preformed heat-stable staphylococcal enterotoxin. Food can be contaminated by staphylococcal carriers or people with active skin infections. In food that is incompletely cooked or left at room temperature, staphylococci reproduce and elaborate enterotoxin. Many foods can serve as growth media, and, despite contamination, they have a normal taste and odor. Severe nausea and vomiting begin 2 to 8 hours after ingestion, typically followed by abdominal cramps and diarrhea. The attack is brief, often lasting < 12 hours.
Diagnosis of Staphylococcal Infections
Gram stain and culture
Diagnosis of staphylococcal infections is by Gram stain and culture of infected material.
Susceptibility tests should be done because methicillin-resistant organisms are now common and require alternative therapy.
When staphylococcal scalded skin syndrome is suspected, cultures should be obtained from blood, urine, the nasopharynx, the umbilicus, abnormal skin, or any suspected focus of infection; the intact bullae are sterile. Although the diagnosis is usually clinical, a biopsy of the affected skin may help confirm the diagnosis.
Staphylococcal food poisoning is usually suspected because of case clustering (eg, within a family, attendees of a social gathering, or customers of a restaurant). Confirmation (typically by the health department) entails isolating staphylococci from suspect food and sometimes testing for enterotoxins.
In osteomyelitis, x-ray changes may not be apparent for 10 to 14 days, and bone rarefaction and periosteal reaction may not be detected for even longer. Abnormalities in MRI, CT, or radionuclide bone scans are often apparent earlier. Bone biopsy (open or percutaneous) should be done for pathogen identification and susceptibility testing.
MRSA surveillance in health care institutions
Some institutions that have a high incidence of methicillin-resistant S. aureus (MRSA) nosocomial infections routinely screen admitted patients for MRSA (active surveillance) by using rapid laboratory techniques to evaluate nasal swab specimens. Some institutions screen only high-risk patients (eg, those who are admitted to the intensive care unit, who have had previous MRSA infection, or who are about to undergo vascular, orthopedic, or cardiac surgery).
Quick identification of MRSA does the following:
Allows carriers to be placed in contact isolation and, when preoperative antibiotic prophylaxis against skin organisms is required, to be given vancomycin as part of their medication regimenagainst skin organisms is required, to be given vancomycin as part of their medication regimen
Decreases the spread of MRSA
May decrease the incidence of nosocomial infections with MRSA
In patients with pneumonia, polymerase chain reaction (PCR) testing for MRSA colonization in the nares has been shown to have a negative predictive value of > 95% for MRSA lung infection and may therefore be useful in antibiotic management.
Treatment of Staphylococcal Infections
Local measures (eg, debridement, removal of catheters)
Antibiotics selected based on severity of infection and local resistance patterns
Management of staphylococcal infections includes abscess drainage, debridement of necrotic tissue, removal of foreign bodies (including intravascular catheters), and use of antibiotics (see table Antibiotic Treatment of Staphylococcal Infections in Adults).
Initial choice and dosage of antibiotics depend on
Infection site
Illness severity
Probability that resistant strains are involved
Thus, it is essential to know local resistance patterns for initial therapy (and ultimately, to know actual drug susceptibility).
Treatment of toxin-mediated staphylococcal disease (the most serious of which is toxic shock syndrome) involves decontamination of the toxin-producing area (exploration of surgical wounds, irrigation, debridement), intensive support (including IV fluids, vasopressors, and respiratory assistance), electrolyte balancing, and antimicrobials. In vitro evidence supports use of a combination of beta-lactamase–resistant, antistaphylococcal antimicrobial agent IV (eg, nafcillin, oxacillin, vancomycin) plus a protein synthesis inhibitor (eg, clindamycin, linezolid). IV immune globulin has been beneficial in severe cases.) involves decontamination of the toxin-producing area (exploration of surgical wounds, irrigation, debridement), intensive support (including IV fluids, vasopressors, and respiratory assistance), electrolyte balancing, and antimicrobials. In vitro evidence supports use of a combination of beta-lactamase–resistant, antistaphylococcal antimicrobial agent IV (eg, nafcillin, oxacillin, vancomycin) plus a protein synthesis inhibitor (eg, clindamycin, linezolid). IV immune globulin has been beneficial in severe cases.
Antibiotic resistance
Many staphylococcal strains produce penicillinase, an enzyme that inactivates several beta-lactam antibiotics; these strains are resistant to penicillin G, ampicillin, amoxicillin, and antipseudomonal penicillins (eg, piperacillin). Many staphylococcal strains produce penicillinase, an enzyme that inactivates several beta-lactam antibiotics; these strains are resistant to penicillin G, ampicillin, amoxicillin, and antipseudomonal penicillins (eg, piperacillin).
Community-acquired strains are often susceptible to penicillinase-resistant penicillins (eg, methicillin, oxacillin, nafcillin, cloxacillin, dicloxacillin), cephalosporins, carbapenems (eg, imipenem, meropenem, ertapenem), tetracyclines, macrolides, fluoroquinolones, trimethoprim/sulfamethoxazole (TMP/SMX), gentamicin, vancomycin, and teicoplanin.are often susceptible to penicillinase-resistant penicillins (eg, methicillin, oxacillin, nafcillin, cloxacillin, dicloxacillin), cephalosporins, carbapenems (eg, imipenem, meropenem, ertapenem), tetracyclines, macrolides, fluoroquinolones, trimethoprim/sulfamethoxazole (TMP/SMX), gentamicin, vancomycin, and teicoplanin.
MRSA isolates have become common, especially in hospitals. MRSA isolates are resistant to almost all beta-lactam antibiotics, including most cephalosporins and carbapenems; however, they may be susceptible to the newest class of MRSA-active cephalosporins (eg, ceftaroline, ceftobiprole [not available in the United States]). Hospital-acquired MRSA is also commonly resistant to many other antibiotics, including erythromycin, clindamycin, and fluoroquinolones. In addition, community-associated MRSA (CA-MRSA) has emerged over the past several years in most geographic regions. CA-MRSA tends to be less resistant to multiple antibiotics than hospital-acquired MRSA. These strains, although resistant to most beta-lactams, are often susceptible to TMP/SMX and tetracyclines (minocycline, doxycycline) and are often susceptible to clindamycin, but there is the potential for emergence of isolates have become common, especially in hospitals. MRSA isolates are resistant to almost all beta-lactam antibiotics, including most cephalosporins and carbapenems; however, they may be susceptible to the newest class of MRSA-active cephalosporins (eg, ceftaroline, ceftobiprole [not available in the United States]). Hospital-acquired MRSA is also commonly resistant to many other antibiotics, including erythromycin, clindamycin, and fluoroquinolones. In addition, community-associated MRSA (CA-MRSA) has emerged over the past several years in most geographic regions. CA-MRSA tends to be less resistant to multiple antibiotics than hospital-acquired MRSA. These strains, although resistant to most beta-lactams, are often susceptible to TMP/SMX and tetracyclines (minocycline, doxycycline) and are often susceptible to clindamycin, but there is the potential for emergence ofclindamycin resistance by strains inducibly resistant to erythromycin (laboratories may report these strains as D-test positive).
Vancomycin is effective against most MRSA, sometimes with rifampin and an aminoglycoside added for some serious infections (ie, osteomyelitis, prosthetic joint infections, prosthetic valve endocarditis). An alternative antibiotic (daptomycin, linezolid, tedizolid, dalbavancin, oritavancin, telavancin, tigecycline, omadacycline, lefamulin, eravacycline, delafloxacin, quinupristin/dalfopristin, TMP/SMX, ceftaroline) should be considered when treating MRSA strains with a is effective against most MRSA, sometimes with rifampin and an aminoglycoside added for some serious infections (ie, osteomyelitis, prosthetic joint infections, prosthetic valve endocarditis). An alternative antibiotic (daptomycin, linezolid, tedizolid, dalbavancin, oritavancin, telavancin, tigecycline, omadacycline, lefamulin, eravacycline, delafloxacin, quinupristin/dalfopristin, TMP/SMX, ceftaroline) should be considered when treating MRSA strains with avancomycin minimum inhibitory concentration (MIC) of ≥ 1.5 mcg/mL.
Vancomycin-resistant S. aureus (VRSA; MIC ≥ 16 mcg/mL) and vancomycin-intermediate–susceptible S. aureus (VISA; MIC 4 to 8 mcg/mL) strains have appeared in the United States. These organisms require linezolid, tedizolid, quinupristin/dalfopristin, daptomycin, TMP/SMX, delafloxacin, oritavancin, or ceftaroline. Dalbavancin and telavancin are active against VISA but have little activity against VRSA. Oritavancin is active against both VISA and VRSA.(VISA; MIC 4 to 8 mcg/mL) strains have appeared in the United States. These organisms require linezolid, tedizolid, quinupristin/dalfopristin, daptomycin, TMP/SMX, delafloxacin, oritavancin, or ceftaroline. Dalbavancin and telavancin are active against VISA but have little activity against VRSA. Oritavancin is active against both VISA and VRSA.
Because incidence of MRSA has increased, initial empiric treatment for serious staphylococcal infections (particularly those that occur in a health care setting) should include an antibiotic with reliable activity against MRSA. Thus, appropriate antibiotics include the following:
For proven or suspected bloodstream infections, vancomycin or daptomycinvancomycin or daptomycin
For pneumonia,vancomycin, telavancin, or linezolid (because , telavancin, or linezolid (becausedaptomycin is not reliably active in the lungs)
Table Antibiotic Treatment of Staphylococcal Infections in Adults summarizes treatment options.
Antibiotic Treatment of Staphylococcal Infections in Adults
Infection | Antibiotics |
|---|---|
Community-acquired cutaneous infections (non-MRSA) | Dicloxacillin or cephalexin 250–500 mg orally every 6 hours for 7–10 daysDicloxacillin or cephalexin 250–500 mg orally every 6 hours for 7–10 days |
Penicillin-allergic patients | Erythromycin 250–500 mg orally every 6 hoursErythromycin 250–500 mg orally every 6 hours Clarithromycin 500 mg orally every 12 hoursClarithromycin 500 mg orally every 12 hours Azithromycin 500 mg orally on the first day, then 250 mg orally every 24 hours on days 2–5Azithromycin 500 mg orally on the first day, then 250 mg orally every 24 hours on days 2–5 Clindamycin 300 mg orally every 6 hoursClindamycin 300 mg orally every 6 hours |
Community-acquired cutaneous infections likely to be due to MRSA | Trimethoprim/sulfamethoxazole 160/800 mg orally every 8–12 hoursTrimethoprim/sulfamethoxazole 160/800 mg orally every 8–12 hours Clindamycin 300–450 mg orally every 6–8 hoursClindamycin 300–450 mg orally every 6–8 hours Linezolid 600 mg orally every 12 hoursLinezolid 600 mg orally every 12 hours Tedizolid 200 mg orally every 24 hoursTedizolid 200 mg orally every 24 hours Delafloxacin 450 mg orally every 12 hoursDelafloxacin 450 mg orally every 12 hours Omadacycline 450 mg orally once a day for 2 days, followed by 300 mg once a dayOmadacycline 450 mg orally once a day for 2 days, followed by 300 mg once a day |
Sulfa-allergic patients | Clindamycin 600 mg orally every 8 hoursClindamycin 600 mg orally every 8 hours Linezolid 600 mg orally every 12 hoursLinezolid 600 mg orally every 12 hours Tedizolid 200 mg orally every 24 hoursTedizolid 200 mg orally every 24 hours Doxycycline 100 mg orally every 12 hours Doxycycline 100 mg orally every 12 hours Delafloxacin 450 mg orally every 12 hoursDelafloxacin 450 mg orally every 12 hours Omadacycline 450 mg orally once a day for 2 days, followed by 300 mg once a dayOmadacycline 450 mg orally once a day for 2 days, followed by 300 mg once a day |
Serious infections unlikely to be due to MRSA | Nafcillin or oxacillin 1–2 g IV every 4–6 hoursNafcillin or oxacillin 1–2 g IV every 4–6 hours Cefazolin 1–2 g IV every 8 hoursCefazolin 1–2 g IV every 8 hours |
Penicillin-allergic patients | Clindamycin 600 mg IV every 8 hoursClindamycin 600 mg IV every 8 hours Vancomycin 15 mg/kg every 12 hoursVancomycin 15 mg/kg every 12 hours |
Serious infection highly likely to be due to MRSA | Vancomycin 15 mg/kg IV every 12 hoursVancomycin 15 mg/kg IV every 12 hours Linezolid 600 mg IV every 12 hours, tedizolid 200 mg IV every 24 hoursLinezolid 600 mg IV every 12 hours, tedizolid 200 mg IV every 24 hours Daptomycin 4–10 mg/kg every 24 hours, depending on site of infection (not for pulmonary infections)Daptomycin 4–10 mg/kg every 24 hours, depending on site of infection (not for pulmonary infections) Ceftobiprole 500 mg IV every 8 hours (not available in the United States) Ceftobiprole 500 mg IV every 8 hours (not available in the United States) Ceftaroline 600 mg IV every 12 hoursCeftaroline 600 mg IV every 12 hours Delafloxacin 300 mg IV every 12 hoursDelafloxacin 300 mg IV every 12 hours Omadacycline 200 mg IV once, followed by 100 mg IV every 24 hours Omadacycline 200 mg IV once, followed by 100 mg IV every 24 hours |
Documented MRSA | By reported sensitivities |
Vancomycin-resistant staphylococci*Vancomycin-resistant staphylococci* | Linezolid 600 mg IV every 12 hoursLinezolid 600 mg IV every 12 hours Quinupristin/dalfopristin 7.5 mg/kg every 8 hours Daptomycin 4–8 mg/kg every 24 hoursDaptomycin 4–8 mg/kg every 24 hours Oritavancin 1200 mg IV once Oritavancin 1200 mg IV once Ceftobiprole 500 mg IV every 8 hours (not available in the United States) Ceftobiprole 500 mg IV every 8 hours (not available in the United States) Ceftaroline 600 mg IV every 12 hoursCeftaroline 600 mg IV every 12 hours |
* No clinical data are available, but listed antibiotics appear to be active in vitro. | |
MRSA = methicillin-resistant Staphylococcus aureus. | |
Prevention of Staphylococcal Infections
Aseptic precautions (eg, thoroughly washing hands between patient examinations, sterilizing shared equipment) help decrease spread in health care institutions.
Strict isolation procedures should be used for patients harboring resistant microbes until their infections have been cured. An asymptomatic nasal carrier of S. aureus does not need to be isolated unless the strain is MRSA or is the suspected source of an outbreak. The Centers for Disease Control and Prevention recommends placing patients who are colonized or infected with MRSA in private rooms and on contact precautions in inpatient acute care settings and using strict isolation procedures (see Strategies to Prevent Hospital-onset Staphylococcus aureus Bloodstream Infections in Acute Care Facilities.)
Multidisciplinary guidelines for antibiotic prophylaxis before certain types of surgery suggest that most patients can be given a single parenteral dose of an antibiotic given shortly before surgery. Cefazolin is used for most procedures. However, in patients with MRSA colonization documented by culture or polymerase chain reaction (PCR) testing, vancomycin should be added (suggest that most patients can be given a single parenteral dose of an antibiotic given shortly before surgery. Cefazolin is used for most procedures. However, in patients with MRSA colonization documented by culture or polymerase chain reaction (PCR) testing, vancomycin should be added (2).
Staphylococcal food poisoning can be prevented by appropriate food preparation. Patients with staphylococcal skin infections should not handle food, and food should be consumed immediately or refrigerated and not kept at room temperature.
Decolonization of MRSA carriers
The S. aureus organism recurs in up to 50% of carriers and frequently becomes resistant. For certain MRSA carriers (eg, preorthopedic, vascular, and cardiovascular surgical patients), some experts recommend nasal decolonization with mupirocin ointment 2 times a day for 5 to 10 days and topical body decolonization regimens with a skin antiseptic solution (eg, organism recurs in up to 50% of carriers and frequently becomes resistant. For certain MRSA carriers (eg, preorthopedic, vascular, and cardiovascular surgical patients), some experts recommend nasal decolonization with mupirocin ointment 2 times a day for 5 to 10 days and topical body decolonization regimens with a skin antiseptic solution (eg,chlorhexidine) or dilute bleach baths (about 5 mL/L) for 5 to 14 days.
Topical nasal mupirocin has been proved somewhat effective for reducing MRSA infection in hospitalized patients (eg, patients in intensive care units, those undergoing major surgeries). Although mupirocin resistance is emerging, a large study showed a 30% reduction in postdischarge MRSA infection risk over 1 year for patients who were colonized with MRSA and treated with decolonization for 5 days 2 times a month for 6 months. Each 5-day decolonization regimen included 2% nasal mupirocin once a day, a 4% chlorhexidine bath or shower once a day, and 0.12% chlorhexidine mouthwash 2 times a day (resistance is emerging, a large study showed a 30% reduction in postdischarge MRSA infection risk over 1 year for patients who were colonized with MRSA and treated with decolonization for 5 days 2 times a month for 6 months. Each 5-day decolonization regimen included 2% nasal mupirocin once a day, a 4% chlorhexidine bath or shower once a day, and 0.12% chlorhexidine mouthwash 2 times a day (1).
Prevention references
1. Huang SS, Singh R, McKinnell JA, et al: Decolonization to reduce postdischarge infection risk among MRSA carriers. N Engl J Med 380:638–650, 2019. doi: 10.1056/NEJMoa1716771
2. Bratzler DW, Dellinger EP, Olsen KM, et al: Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surg Infect (Larchmt) 14(1):73–156, 2013. doi: 10.1089/sur.2013.9999
Key Points
Staphylococcus aureus is the most dangerous staphylococcal species.
Most staphylococcal diseases involve direct tissue invasion and cause skin and soft-tissue infections, IV catheter infections, pneumonia, endocarditis, and osteomyelitis.
Some strains produce a toxin that can cause toxic shock syndrome, scalded skin syndrome, or food poisoning.
Methicillin-resistant strains are common, and vancomycin resistance is appearing in the United States.Methicillin-resistant strains are common, and vancomycin resistance is appearing in the United States.
Antibiotic choice depends on source and location of infection and community or institutional resistance patterns.







