


- Overview of Shoulder Dislocation Reduction Techniques
- How To Reduce Anterior Shoulder Dislocations Using the Davos Technique
- How To Reduce Anterior Shoulder Dislocations Using External Rotation (Hennepin Technique)
- How To Reduce Anterior Shoulder Dislocations Using the FARES Method
- How To Reduce Anterior Shoulder Dislocations Using Scapular Manipulation
- How To Reduce Anterior Shoulder Dislocations Using the Stimson Technique
- How To Reduce Anterior Shoulder Dislocations Using Traction-Countertraction
- How To Reduce Posterior Shoulder Dislocations
- How To Reduce a Posterior Elbow Dislocation
- How To Reduce a Radial Head Subluxation (Nursemaid Elbow)
- How To Reduce a Posterior Hip Dislocation
- How To Reduce a Lateral Patellar Dislocation
- How To Reduce an Ankle Dislocation


The Stimson technique has the advantage of not requiring an assistant, but disadvantages include the increased time required, difficulty monitoring a prone patient, and the risk of the patient slipping off an elevated stretcher.
(See also Overview of Shoulder Dislocation Reduction Techniques, Overview of Dislocations, and Shoulder Dislocations.)
Indications for the Stimson Technique
Anterior dislocation of the shoulder
Reduction should be attempted soon (eg, within 30 minutes) after the diagnosis is made.
Reduction should be attempted immediately if an associated neurovascular deficit or skin tenting (due to a displaced bone fracture or, less commonly, a fracture-dislocation, with potential for skin penetration or breakdown) is present. If an orthopedic surgeon is unavailable, closed reduction can be attempted, ideally using minimal force; if reduction is unsuccessful, it may need to be performed in the operating room under general anesthesia.
Open dislocations require surgery, but closed reduction techniques and immobilization should be performed as interim treatment if the orthopedic surgeon is unavailable and a neurovascular deficit is present.
Contraindications to the Stimson Technique
Contraindications to simple closed reduction:
Greater tuberosity fracture with > 1 cm displacement
Significant Hill-Sachs deformity (≥ 20% humeral head deformity due to impaction against glenoid rim)
Surgical neck fracture (below the greater and lesser tuberosities)
Bankart fracture (anteroinferior glenoid rim) involving a bone fragment of over 20% and with glenohumeral instability
Proximal humeral fracture of 2 or more parts
These significant associated fractures require orthopedic evaluation and management, because of the risk of the procedure itself increasing displacement and injury severity.
Other reasons to consult with an orthopedic surgeon prior to reduction include:
The joint is exposed (ie, an open fracture or dislocation where bone or fracture segments penetrate the skin).
The patient is a child, in whom a physeal (growth plate) fracture is often present; however, if a neurovascular deficit is present, reduction should be performed immediately if the orthopedic surgeon is unavailable.
The dislocation is older than 7 to 10 days, due to an increased risk of damaging the axillary artery during the reduction, especially in older patients.
Contraindications to Stimson method:
Intoxicated or multi-trauma patient: Prone position (part of Stimson method) impedes care and monitoring of such patients.
Pregnant patient: Prone position causes abdominal discomfort.
Complications of the Stimson Technique
Complications are uncommon with the Stimson technique.
Equipment for the Stimson Technique
2.27- to 6.8-kg (5- to 10- lb) weights (commercial weights or bags of IV fluids) and materials (eg, stockinette, padded wrist restraint, or commercial device) to hang the weights from the patient’s wrist
A strap, sheet, or other means of restraint to keep the patient from slipping off the stretcher
Intra-articular anesthetic: 20 mL of 1% lidocaine, 20-mL syringe, 5 cm (2-inch) 20-gauge needle, antiseptic solution (eg, chlorhexidine, povidone iodine), gauze padsIntra-articular anesthetic: 20 mL of 1% lidocaine, 20-mL syringe, 5 cm (2-inch) 20-gauge needle, antiseptic solution (eg, chlorhexidine, povidone iodine), gauze pads
Shoulder immobilizer or sling and swathe
Additional Considerations for the Stimson Technique
Intra-articular anesthesia is well suited to the Stimson technique, providing excellent analgesia and requiring minimal patient monitoring.
Regional anesthesia may be used (eg, ultrasound-guided interscalene nerve block) but has the disadvantage of limiting post-reduction neurologic examination.
Procedural sedation should be avoided for the Stimson technique because the consequences of respiratory inhibition will be amplified by the patient’s prone position and because safely monitoring the patient and maintaining adequate sedation for the duration of this procedure can be difficult.
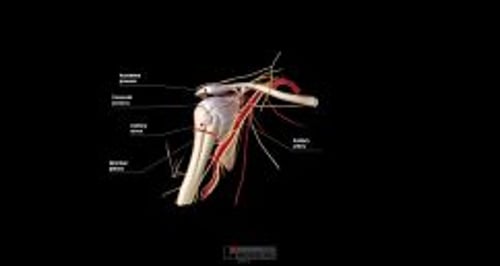
Relevant Anatomy for the Stimson Technique
In most anterior dislocations, the humeral head is trapped outside and against the anterior lip of the glenoid fossa. Reduction techniques must distract the humeral head away from the lip and then return the humeral head into the fossa.
Deficits of the axillary nerve are the most frequent nerve deficits with anterior shoulder dislocations. They often resolve within several months, sometimes soon after the shoulder reduction.
Axillary artery injury is rare with anterior shoulder dislocations and suggests possible concurrent brachial plexus injury (because the brachial plexus surrounds the artery) (1).
Positioning for the Stimson Technique
Place the patient prone on the stretcher with the affected arm hanging off the side and tie the patient’s hips to the stretcher with a restraining strap or bed sheet to prevent the patient from falling off the stretcher.
Step-by-Step Description of the Stimson Technique
Neurovascular examination
Perform a pre-procedure neurovascular examination of the affected arm, and repeat the examination after each reduction attempt. Generally, testing motor function is more reliable than testing sensation, partly because cutaneous nerve territories may overlap. Assess the following:
Distal pulses, capillary refill, cool extremity (axillary artery)
Light touch sensation of the lateral aspect of the upper arm (axillary nerve), thenar and hypothenar eminences (median and ulnar nerves), and dorsum of the 1st web space (radial nerve)
Shoulder abduction against resistance, while feeling the deltoid muscle for contraction (axillary nerve): However, if this test worsens the patient's pain, omit it until after the shoulder has been reduced.
Thumb-index finger apposition ("OK" gesture) and finger flexion against resistance (median nerve)
Finger abduction against resistance (ulnar nerve)
Wrist and finger extension against resistance (radial nerve)
Intra-articular analgesia
The needle insertion site is approximately 2 cm inferior to the lateral edge of the acromion process (into the depression created by the absence of the humeral head).
Swab the area with antiseptic solution, and allow the antiseptic solution to dry for at least 1 minute.
Optional: Place a skin wheal of local anesthetic (≤ 1 mL) at the site.
Insert the intra-articular needle perpendicular to the skin, apply back pressure on the syringe plunger, and advance the needle medially and slightly inferiorly approximately 2 cm.
If any blood is aspirated from the joint, hold the needle hub motionless, switch to an empty syringe, aspirate all of the blood, and re-attach the anesthetic syringe.
Inject 10 to 20 mL of anesthetic solution (eg, 1% lidocaine).Inject 10 to 20 mL of anesthetic solution (eg, 1% lidocaine).
Wait for analgesia to occur (up to 15 to 20 minutes) before proceeding.
Reduce the shoulder — Stimson method
With the patient prone and secured to the bed, hang the weights from the wrist. The weights should be added gradually rather than all at once, if necessary, to minimize the patient's discomfort. After up to 30 minutes, the muscle spasm usually relaxes enough to allow the humeral head to reduce.
If reduction does not occur, manually add some downward/axial traction or apply gentle external rotation to the upper arm.
If reduction does not occur, perform scapular manipulation with the weights still in place.


Aftercare for the Stimson Technique
Successful reduction is preliminarily confirmed by restoration of a normal round shoulder contour, by decreased pain, and by the patient's renewed ability to reach across the chest and place the palm of the hand upon the opposite shoulder.
Immobilize the shoulder with a sling and swathe or with a shoulder immobilizer.
Because the joint can spontaneously dislocate after successful reduction, do not delay immobilizing the joint.
Perform a post-procedure neurovascular examination. A neurovascular deficit warrants immediate orthopedic evaluation.
Perform post-procedure radiographs to confirm proper reduction and identify any coexisting fractures.
Arrange orthopedic follow-up.
Warnings and Common Errors for the Stimson Technique
Ensure that the patient is secured to the stretcher to prevent falling off the stretcher.
Apparent shoulder dislocation in a child is often a fracture involving the growth plate, which tends to fracture before the joint is disrupted.
Tips and Tricks for the Stimson Technique
In patients who return with increased pain within 48 hours after a reduction, hemarthrosis is likely (unless the shoulder has again dislocated). Aspirate the blood from the joint space (see How to Do Arthrocentesis of the Shoulder).
Reference
1. Perlmutter GS, Apruzzese W. Axillary nerve injuries in contact sports: recommendations for treatment and rehabilitation. Sports Med. 1998;26(5):351-361. doi:10.2165/00007256-199826050-00005
Drugs Mentioned In This Article






