



Strabismus is misalignment of the eyes, which causes deviation from the parallelism of normal gaze. Diagnosis is clinical, including observation of the corneal light reflex and use of a cover test. Treatment may include correction of visual impairment with patching and corrective lenses, alignment by corrective lenses, and surgical repair.
Topic Resources

")
Strabismus occurs in about 3% of children (1). Left untreated, approximately half of children with strabismus have some visual loss due to amblyopia (functional reduction in visual acuity of an eye caused by disuse during visual development).


General reference
1. Friedman DS, Repka MX, Katz J, et al: Prevalence of amblyopia and strabismus in white and African American children aged 6 through 71 months the Baltimore Pediatric Eye Disease Study. Ophthalmology 116(11):2128-34.e342, 2009. doi: 10.1016/j.ophtha.2009.04.034
Classification of Strabismus
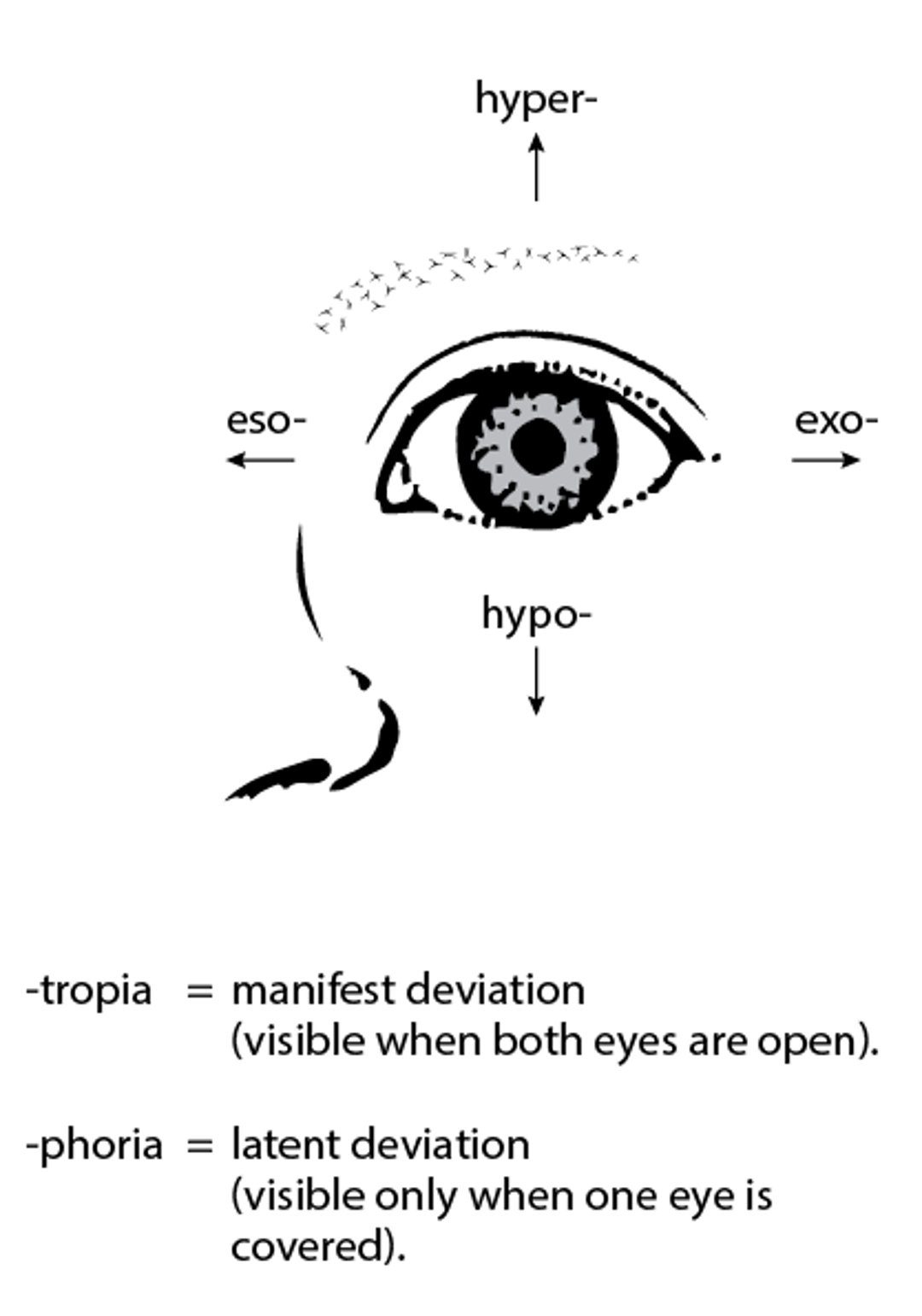
Several varieties of strabismus have been described, based on direction of deviation, specific conditions under which deviation occurs, and whether deviation is constant or intermittent. Description of these varieties requires the definition of several terms. The direction of eye deviation is described using the following prefixes:
Eso: Nasal deviation
Exo: Temporal deviation
Hyper: Upward deviation
Hypo: Downward deviation
(See figure Ocular Deviations in Strabismus.)
A tropia is a manifest deviation, detectable with both eyes open (so that vision is binocular). A tropia can be constant or intermittent and may involve one eye or both eyes.
A phoria is a latent deviation, detectable only when one eye is covered so that vision is monocular. The deviation in a phoria is latent because the brain, using the extraocular muscles, corrects the minor misalignment.
A comitant deviation has the same amplitude or degree of misalignment in all gaze directions.
An incomitant deviation varies in amplitude or degree of misalignment depending on gaze direction.
Ocular Deviations in Strabismus
Strabismus can involve both eyes; the left eye is shown here. The direction of the deviation is designated by the prefixes eso-, exo-, hyper-, and hypo-. When the deviation is visible, it is indicated by the suffixes -tropia and -phoria. |

Etiology of Strabismus
Most strabismus is caused by
Refractive error
Muscle imbalance
Rare causes include retinoblastoma or other serious ocular defects and neurologic disease.
Strabismus may be infantile or acquired. The term infantile rather than congenital is preferred because the presence of true strabismus at birth is uncommon, and the term infantile permits inclusion of varieties that develop within the first 6 months of life. The term acquired includes varieties that develop after 6 months of life.
Risk factors for infantile strabismus include family history (first- or second-degree relative), genetic disorders (Down syndrome and craniofacial syndromes), prenatal drug exposure (including alcohol), prenatal medication exposure, prematurity or low birth weight, congenital eye defects, and cerebral palsy.
Acquired strabismus can develop acutely or gradually. Causes of acquired strabismus include refractive error (high hyperopia), tumors (eg, retinoblastoma), head trauma, neurologic conditions (eg, increased intracranial pressure; cerebral palsy; spina bifida; palsy of the 3rd cranial nerve, 4th cranial nerve, or 6th cranial nerve), viral infections (eg, encephalitis, meningitis), and acquired eye defects. Specific causes vary depending on the type of deviation.
Esotropia is commonly infantile. Infantile esotropia is considered idiopathic, although an anomaly of fusion is the suspected cause. Accommodative esotropia, a common variety of acquired esotropia, develops between 2 years and 4 years of age and is associated with hyperopia. Sensory esotropia occurs when severe visual loss (due to conditions such as cataracts, optic nerve anomalies, or tumors) interferes with the brain’s effort to maintain ocular alignment.


Esotropia can be paralytic, so designated because the cause is a 6th (abducens) cranial nerve palsy, but it is an uncommon cause. Esotropia can also be a component of a syndrome. Duane syndrome (congenital absence of the abducens nucleus with anomalous innervation of the lateral rectus extraocular muscle by the 3rd cranial nerve) and Möbius syndrome (anomalies of multiple cranial nerves) are specific examples.
Exotropia is most often intermittent and idiopathic. Less often, exotropia is constant and paralytic, as with infantile exotropia or 3rd (oculomotor) cranial nerve palsy.
Hypertropia can be paralytic, caused by 4th (trochlear) cranial nerve palsy that occurs congenitally or after head trauma or, less commonly, as a result of 3rd cranial nerve palsy.
Hypotropia can be restrictive, caused by mechanical restriction of full movement of the globe rather than neurologic interference with eye movement. For example, restrictive hypotropia can result from a blowout fracture of the orbit floor or walls. Less commonly, restrictive hypotropia can be caused by Graves ophthalmopathy (thyroid eye disease). Third cranial nerve palsy and Brown syndrome (congenital or acquired tightness and restriction of the superior oblique muscle tendon) are other uncommon causes.
Symptoms and Signs of Strabismus
Unless severe, phorias rarely cause symptoms of strabismus. If symptomatic, phorias typically cause asthenopia (eye strain).
Tropias sometimes result in symptoms. For example, torticollis may develop to compensate for the brain’s difficulty in fusing images from misaligned eyes and to reduce diplopia. Some children with tropias have normal and equal visual acuity; however, amblyopia frequently develops with tropias and is due to cortical suppression of the image in the deviating eye to avoid confusion and diplopia.
Diagnosis of Strabismus
Physical and neurologic examinations at well-child checkups
Tests (eg, corneal light reflex, alternate cover, cover-uncover)
Prisms
Strabismus can be detected during well-child checkups through the history and eye examination. Evaluation should include questions about family history of amblyopia or strabismus and, if family or caregivers have noticed deviation of gaze, questions about when the deviation began, when or how often it is present, and whether there is a preference for using one eye for fixation. Physical examination should include an assessment of visual acuity, pupil reactivity, and the extent of extraocular movements. Slit-lamp examination is done to detect signs of cataract, and funduscopic examination is done to detect signs of structural defects or pathology of disorders such as retinoblastoma. Neurologic examination, particularly of the cranial nerves, is important.
The corneal light reflex test is a good screening test, but it is not very sensitive for detecting small deviations. The child looks at a light and the light reflection (reflex) from the pupil is observed; normally, the reflex appears symmetric (ie, in the same location on each pupil). The light reflex for an exotropic eye is nasal to the pupillary center, whereas the reflex for an esotropic eye is temporal to the pupillary center. Vision screening devices such as photoscreeners may be used by trained lay personnel to identify children at risk.
When doing the cover test, the child is asked to fixate on an object. One eye is then covered while the other is observed for movement. No movement should be detected if the eyes are properly aligned, but manifest strabismus is present if the uncovered eye shifts to establish fixation once the other eye, which had fixed on the object, is covered. The test is then repeated on the other eye.
In a variation of the cover test, called the alternate uncover test, the child is asked to fixate on an object while the examiner alternately covers one eye and then the other, back and forth. An eye with a latent strabismus shifts position when it is uncovered. In exotropia, the eye that was covered turns in to fixate when the cover is removed; in esotropia, it turns out to fixate when the cover is removed. Deviations can be quantified by using prisms positioned such that the deviating eye does not need to move to fixate. The power of the prism is used to quantify the deviation and provide a measurement of the magnitude of misalignment of the visual axes. The unit of measurement used by ophthalmologists is the prism diopter. One prism diopter is a deviation of the visual axes of 1 cm at 1 m.
Strabismus should be distinguished from pseudostrabismus, which is the appearance of esotropia in a child with good visual acuity in both eyes but a wide nasal bridge or broad epicanthal folds that obscure much of the white sclera nasally when looking laterally. The light reflex and cover tests are normal in a child with pseudostrabismus.
Neuroimaging may be necessary to identify the cause of acquired cranial nerve palsies. In addition, genetics evaluation may be beneficial for certain ocular malformations.
Treatment of Strabismus
Patching or atropine drops for attendant amblyopiaPatching or atropine drops for attendant amblyopia
Contact lenses or eyeglasses (for refractive error)
Eye exercises (for convergence insufficiency only)
Surgical alignment of the eyes
Treatment of strabismus is first aimed at equalizing vision (ie, correcting amblyopia) and then, once vision is optimized, at aligning the eyes.
Treatment of children with amblyopia requires measures to encourage use of the amblyopic eye, such as patching the better eye or administering atropine drops into the better eye to provide a visual advantage to the amblyopic eye; improved vision offers a better prognosis for development of binocular vision and for stability if surgery is done to treat the strabismus. Patching is not, however, a treatment for strabismus. requires measures to encourage use of the amblyopic eye, such as patching the better eye or administering atropine drops into the better eye to provide a visual advantage to the amblyopic eye; improved vision offers a better prognosis for development of binocular vision and for stability if surgery is done to treat the strabismus. Patching is not, however, a treatment for strabismus.
Eyeglasses or contact lenses are sometimes used if the amount of refractive error is significant enough to interfere with fusion, especially in children with accommodative esotropia.
Orthoptic eye exercises can help correct intermittent exotropia with convergence insufficiency.
Surgical repair is generally done when nonsurgical methods are unsuccessful in aligning the eyes satisfactorily. Surgical repair consists of loosening (recession) and tightening (resection) procedures, most often involving the horizontal rectus muscles, and is most often done bilaterally. Surgical repair is typically done in an outpatient setting. Rates for successful realignment can exceed 80% (1); about 20% need another surgical procedure. The most common complications are overcorrection or undercorrection and recurrence of strabismus later in life. Rare complications include infection, excessive bleeding, and vision loss.
Treatment reference
1. Ekdawi NS, Nusz KJ, Diehl NN, Mohney BG: Postoperative outcomes in children with intermittent exotropia from a population-based cohort. J AAPOS 13(1):4–7, 2009. doi: 10.1016/j.jaapos.2008.06.001
Prognosis for Strabismus
Strabismus should not be ignored on the assumption that it will be outgrown. Permanent vision loss can occur if strabismus and its attendant amblyopia are not treated promptly; children treated later respond somewhat, but once the visual system has matured (typically by age 8), response is minimal. As a result, all children should have periodic formal vision screenings during the preschool years.
Key Points
Strabismus is misalignment of the eyes; it occurs in about 3% of children and causes some vision loss (amblyopia) in about half of them.
Most cases are caused by refractive error or muscle weakness but occassionally a serious disorder is involved (eg, retinoblastoma, cranial nerve palsy).
Permanent vision loss can occur if strabismus and its attendant amblyopia are not treated promptly; the visual system often does not respond to treatment after age 8 years.
Physical examination can detect most strabismus.
Treatment depends on cause, but surgery of the extraocular muscles is sometimes necessary.







