




")





In patients with diabetes mellitus, years of poorly controlled hyperglycemia lead to multiple, primarily vascular, complications that affect small vessels (microvascular), large vessels (macrovascular), or both.
The mechanisms by which vascular disease develops include
Glycosylation of serum and tissue proteins with formation of advanced glycation end products
Superoxide production
Activation of protein kinase C, a signaling molecule that increases vascular permeability and causes endothelial dysfunction
Accelerated hexosamine biosynthetic and polyol pathways leading to sorbitol accumulation within tissues
Hypertension and dyslipidemias that commonly accompany diabetes mellitus
Arterial microthromboses
Proinflammatory and prothrombotic effects of hyperglycemia and hyperinsulinemia that impair vascular autoregulation
Microvascular disease underlies 3 common and devastating manifestations of diabetes mellitus:
Microvascular disease may also impair skin healing, so that even minor breaks in skin integrity can develop into deeper ulcers and easily become infected, particularly in the lower extremities. Intensive control of plasma glucose can prevent or delay many of these complications but may not reverse them once established.
Macrovascular disease involves atherosclerosis of large vessels, which can lead to
Immune dysfunction is another major complication and develops from the direct effects of hyperglycemia on cellular immunity. Patients with diabetes mellitus are particularly susceptible to bacterial and fungal infections.

Diabetic Retinopathy
Diabetic retinopathy is a common cause of adult blindness in the United States. It is characterized initially by retinal capillary microaneurysms (background retinopathy) and later by neovascularization (proliferative retinopathy) and macular edema. There are no early symptoms, but focal blurring, vitreous or retinal detachment, and partial or total vision loss can eventually develop; rate of progression is highly variable.
Screening and diagnosis are by retinal examination performed by an ophthalmologist, which should be done regularly (usually annually) in both type 1 and type 2 diabetes. Early detection and treatment are critical to preventing vision loss. Treatment for all patients includes intensive glycemic and blood pressure control. Panretinal laser photocoagulation is used for proliferative diabetic retinopathy and sometimes severe nonproliferative diabetic retinopathy. Vascular endothelial growth factor (VEGF) inhibitors such as aflibercept, bevacizumab, and ranibizumab are used for macular edema and can also be used for proliferative retinopathy, but this treatment requires frequent regular visits. Screening and diagnosis are by retinal examination performed by an ophthalmologist, which should be done regularly (usually annually) in both type 1 and type 2 diabetes. Early detection and treatment are critical to preventing vision loss. Treatment for all patients includes intensive glycemic and blood pressure control. Panretinal laser photocoagulation is used for proliferative diabetic retinopathy and sometimes severe nonproliferative diabetic retinopathy. Vascular endothelial growth factor (VEGF) inhibitors such as aflibercept, bevacizumab, and ranibizumab are used for macular edema and can also be used for proliferative retinopathy, but this treatment requires frequent regular visits.
Diabetic Nephropathy
Diabetic nephropathy is a leading cause of chronic kidney disease in the United States. It is characterized by thickening of the glomerular basement membrane, mesangial expansion, and glomerular sclerosis. These changes cause glomerular hypertension and progressive decline in glomerular filtration rate (GFR). Systemic hypertension may accelerate progression. The disease is usually asymptomatic until nephrotic syndrome or kidney failure develops.
Diagnosis is by detection of urinary albumin or decline in GFR. Once diabetes is diagnosed (and annually thereafter), urinary albumin level should be monitored so that nephropathy can be detected early. Monitoring can be done by measuring the albumin:creatinine ratio on a spot urine specimen or total urinary albumin in a 24-hour collection. A ratio ≥ 30 mg/g ( ≥ 3.4 mg/mmol) or an albumin excretion of 30 to 299 mg/day signifies moderately increased albuminuria (previously called microalbuminuria) and early diabetic nephropathy. An albumin excretion ≥ 300 mg/day is considered severely increased albuminuria (previously called macroalbuminuria), or overt proteinuria, and signifies more advanced diabetic nephropathy. Typically a urine dipstick is positive only if the protein excretion exceeds 300 to 500 mg/day.
Treatment is rigorous glycemic control combined with blood pressure control. An angiotensin-converting enzyme (ACE) inhibitor or an angiotensin II receptor blocker (ARB) should be used at the earliest sign of albuminuria (albumin:creatinine ratio ≥ 30 mg/g [ ≥ 3.4.mg/mmol]), to prevent progression of kidney disease because these medications lower intraglomerular blood pressure and thus have renoprotective effects. However, these medications have not been shown to be beneficial for primary prevention (ie, in patients who do not have albuminuria) (1, 2, 3).
Sodium-glucose cotransporter- 2 (SGLT-2) inhibitors also delay progression of renal disease and should be prescribed in patients with diabetic nephropathy who have an estimated glomerular filtration rate (eGRF) ≥20 mL/minute and a urine albumin:creatinine ratio ≥ 200 mg/g.
Fineronone, a nonsteroidal mineralocorticoid receptor antagonist, has also been shown to decrease the risk of progression of diabetic kidney disease and cardiovascular events and can be used in addition to, or instead of, an ACE inhibitor or ARB (4).
Diabetic nephropathy references
1. Bilous R, Chaturvedi N, Sjølie AK, et al. Effect of candesartan on microalbuminuria and albumin excretion rate in diabetes: three randomized trials. Ann Intern Med 2009;151(1):11-W4. doi:10.7326/0003-4819-151-1-200907070-00120
2. Randomised placebo-controlled trial of lisinopril in normotensive patients with insulin-dependent diabetes and normoalbuminuria or microalbuminuria. The EUCLID Study Group. Lancet 1997;349(9068):1787-1792.
3. Mauer M, Zinman B, Gardiner R, et al. Renal and retinal effects of enalapril and losartan in type 1 diabetes. N Engl J Med 2009;361(1):40-51. doi:10.1056/NEJMoa0808400
4. Veneti S, Tziomalos K. The Role of Finerenone in the Management of Diabetic Nephropathy. Diabetes Ther 2021;12(7):1791-1797. doi:10.1007/s13300-021-01085-z
Diabetic Neuropathy
Diabetic neuropathy is the result of nerve ischemia due to microvascular disease, direct effects of hyperglycemia on neurons, and intracellular metabolic changes that impair nerve function. There are multiple types, including
Symmetric polyneuropathy (with small- and large-fiber variants)
Cranial neuropathy
Symmetric polyneuropathy is most common and affects the distal feet and hands (stocking-glove distribution); it manifests as paresthesias, dysesthesias, or a painless loss of sense of touch, vibration, proprioception, or temperature. In the lower extremities, these symptoms can lead to blunted perception of foot trauma due to ill-fitting shoes and abnormal weight bearing, which can in turn lead to foot ulceration and infection or to fractures, subluxation, and dislocation or destruction of normal foot architecture (Charcot arthropathy). Small-fiber neuropathy is characterized by pain, numbness, and loss of temperature sensation with preserved vibration and position sense. Patients are prone to foot ulceration and neuropathic joint degeneration and have a high incidence of autonomic neuropathy. Predominant large-fiber neuropathy is characterized by muscle weakness, loss of vibration and position sense, and lack of deep tendon reflexes. Atrophy of intrinsic muscles of the feet and foot drop can occur.
Autonomic neuropathy can cause orthostatic hypotension, exercise intolerance, resting tachycardia, dysphagia, nausea and vomiting (due to gastroparesis), constipation and/or diarrhea (including dumping syndrome), fecal incontinence, urinary retention and/or incontinence, erectile dysfunction and retrograde ejaculation, and decreased vaginal lubrication.
Radiculopathies most often affect the proximal lumbar (L2 through L4) nerve roots, causing pain, weakness, and atrophy of the lower extremities (diabetic amyotrophy), or the proximal thoracic (T4 through T12) nerve roots, causing abdominal pain (thoracic polyradiculopathy).
Cranial neuropathies cause diplopia, ptosis, and anisocoria when they affect the 3rd cranial nerve or motor palsies when they affect the 4th or 6th cranial nerve.
Mononeuropathies cause finger weakness and numbness (median nerve) or foot drop (peroneal nerve). Patients with diabetes are also prone to nerve compression disorders, such as carpal tunnel syndrome. Mononeuropathies can occur in several places simultaneously (mononeuritis multiplex). All tend to affect older patients predominantly and usually abate spontaneously over months; however, nerve compression disorders do not.
Diagnosis of symmetric polyneuropathy is by detection of sensory deficits and diminished ankle reflexes. Loss of ability to detect the light touch of a nylon monofilament identifies patients at highest risk of foot ulceration (see figure Diabetic Foot Screening). Alternatively, a 128-Hz tuning fork can be used to assess vibratory sense on the dorsum of the first toe.
Electromyography and nerve conduction studies may be needed to evaluate all forms of neuropathy and are sometimes used to exclude other causes of neuropathic symptoms, such as radiculopathy not caused by diabetes and carpal tunnel syndrome.
Management of neuropathy involves a multidimensional approach including glycemic control, regular foot care, and management of pain. Strict glycemic control may lessen neuropathy. Treatments to relieve symptoms include topical capsaicin cream, tricyclic antidepressants (eg, amitriptyline), serotonin-Management of neuropathy involves a multidimensional approach including glycemic control, regular foot care, and management of pain. Strict glycemic control may lessen neuropathy. Treatments to relieve symptoms include topical capsaicin cream, tricyclic antidepressants (eg, amitriptyline), serotonin-norepinephrine reuptake inhibitors (eg, duloxetine), and antiseizure medications (eg, pregabalin, gabapentin). Patients with sensory loss should examine their feet daily to detect minor foot trauma and prevent it from progressing to limb-threatening infection.reuptake inhibitors (eg, duloxetine), and antiseizure medications (eg, pregabalin, gabapentin). Patients with sensory loss should examine their feet daily to detect minor foot trauma and prevent it from progressing to limb-threatening infection.
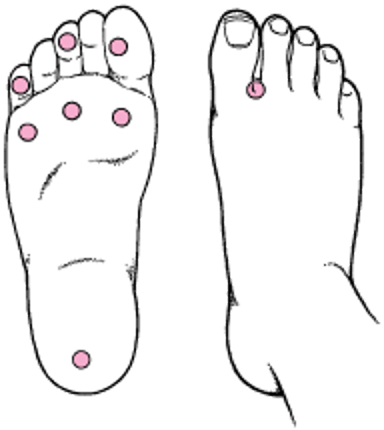
Diabetic Foot Screening
A 10-g monofilament esthesiometer is touched to specific sites on each foot and is pushed until it bends. This test provides a constant, reproducible pressure stimulus (usually a 10-g force), which can be used to monitor change in sensation over time. Both feet are tested, and presence (+) or absence (−) of sensation at each site is recorded. |

Macrovascular Disease
Large-vessel atherosclerosis is a result of the hyperinsulinemia, dyslipidemia, and hyperglycemia characteristic of diabetes mellitus. Manifestations are
Diagnosis is made by history and physical examination. Treatment is rigorous control of atherosclerotic risk factors, including normalization of plasma glucose, lipids, and blood pressure, combined with smoking cessation, daily intake of aspirin (if indicated), and statins. A multifactorial approach that includes management of glycemic control, hypertension, and dyslipidemia may be effective in reducing the rate of cardiovascular events. In contrast with microvascular disease, intensive control of plasma glucose alone has been shown to reduce risk in type 1 diabetes but not in type 2 (1, 2, 3). Certain diabetes medications decrease the risk of major adverse cardiovascular events, including metformin and some SGLT2 inhibitors and ). Certain diabetes medications decrease the risk of major adverse cardiovascular events, including metformin and some SGLT2 inhibitors andglucagon-like peptide-1 (GLP-1) receptor agonists.
Macrovascular disease references
1. ACCORD Study Group; ACCORD Eye Study Group, Chew EY, et al. Effects of medical therapies on retinopathy progression in type 2 diabetes [published correction appears in N Engl J Med 2011 Jan 13;364(2):190] [published correction appears in N Engl J Med 2012 Dec 20;367(25):2458]. N Engl J Med 2010;363(3):233-244. doi:10.1056/NEJMoa1001288
2. Nathan DM, Cleary PA, Backlund JY, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 2005;353(25):2643-2653. doi:10.1056/NEJMoa052187
3. Zoungas S, Chalmers J, Neal B, et al. Follow-up of blood-pressure lowering and glucose control in type 2 diabetes. N Engl J Med 2014;371(15):1392-1406. doi:10.1056/NEJMoa1407963
Cardiomyopathy
Diabetic cardiomyopathy is thought to result from many factors, including epicardial atherosclerosis, hypertension and left ventricular hypertrophy, microvascular disease, endothelial and autonomic dysfunction, obesity, and metabolic disturbances. Patients develop heart failure due to impairment in left ventricular systolic and diastolic function and are more likely to develop heart failure after myocardial infarction.
Infection
Patients with poorly controlled diabetes mellitus are prone to bacterial and fungal infections because of adverse effects of hyperglycemia on the function of granulocytes and T cells. In addition to an overall increase in risk for infectious diseases, individuals with diabetes have an increased susceptibility to mucocutaneous fungal infections (eg, oral and vaginal candidiasis) and bacterial foot infections (including osteomyelitis), which are typically exacerbated by lower extremity vascular insufficiency and diabetic neuropathy. Hyperglycemia is a well-established risk factor for surgical site infections.
People with diabetes have a higher risk for severe illness or death from COVID-19; either type 1 diabetes or type 2 diabetes is an independent risk factor for COVID-related death (1). In people with diabetes infected with SARS-CoV-2, higher blood glucose levels have been associated with poorer outcomes, including higher mortality. Several studies have reported an increased risk of new-onset type 1 diabetes associated with COVID-19 (2); however, other studies have suggested this effect may be due to a delay in diagnosis due to pandemic lockdowns.
Infection references
1. Hartmann-Boyce J, Rees K, Perring JC, et al. Risks of and From SARS-CoV-2 Infection and COVID-19 in People With Diabetes: A Systematic Review of Reviews [published correction appears in Diabetes Care 2022 Jun 2;45(6):1489]. Diabetes Care 2021;44(12):2790-2811. doi:10.2337/dc21-0930
2. D'Souza D, Empringham J, Pechlivanoglou P, Uleryk EM, Cohen E, Shulman R. Incidence of Diabetes in Children and Adolescents During the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. JAMA Netw Open 2023;6(6):e2321281. doi:10.1001/jamanetworkopen.2023.21281
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD)
Metabolic associated steatotic liver disease (MASLD, formerly nonalcoholic fatty liver disease [NAFLD]), is increasingly common and represents an important comorbidity of type 2 diabetes. Some studies have found that over half of patients with type 2 diabetes have MASLD (1). MASLD can also occur in patients with metabolic syndrome, obesity, and dyslipidemia in the absence of diabetes mellitus.
Diagnosis of MASLD requires evidence of hepatic steatosis by imaging or histology, and a lack of other causes of fat accumulation (such as alcohol consumption or medications that cause fat accumulation) (2). MASLD occurs when there is ≥ 5% hepatic steatosis but no evidence of hepatocellular injury. In contrast, metabolic dysfunction-associated steatohepatitis (MASH), formerly nonalcoholic steatohepatitis (NASH), requires both hepatic steatosis (≥ 5%) and inflammation with hepatocyte injury. Fibrosis may also occur in MASH and can lead to cirrhosis. The pathogenesis of MASLD is not well understood but is clearly related to insulin resistance, leading to accumulation of triglycerides in the liver.
Individuals with type 2 diabetes can be screened for fibrosis by calculating the fibrosis 4 index for liver fibrosis (FIB-4 index) from age, aminotransferase levels, and platelet count. Further testing to look for fibrosis, with transient elastography or fibrosis blood markers can be performed if the FIB-4 score shows indeterminate or high risk of fibrosis.

The mainstays of treatment are diet, exercise, and weight loss. In patients with diabetes and evidence of MASH, use of pioglitazone or a GLP-1 receptor agonist such as liraglutide or semaglutide has been shown to slow progression of fibrosis (The mainstays of treatment are diet, exercise, and weight loss. In patients with diabetes and evidence of MASH, use of pioglitazone or a GLP-1 receptor agonist such as liraglutide or semaglutide has been shown to slow progression of fibrosis (3, 4, 5, 6, 7). Other medications known to induce weight loss in diabetes (eg, the dual glucose-dependent insulinotropic polypeptide [GIP] and GLP-1 inhibitor tirzepatide, SGLT-2 inhibitors) can be used. ). Other medications known to induce weight loss in diabetes (eg, the dual glucose-dependent insulinotropic polypeptide [GIP] and GLP-1 inhibitor tirzepatide, SGLT-2 inhibitors) can be used.
MASLD references
1. Lee YH, Cho Y, Lee BW, et al. Nonalcoholic Fatty Liver Disease in Diabetes. Part I: Epidemiology and Diagnosis [published correction appears in Diabetes Metab J 2019 Oct;43(5):731]. Diabetes Metab J 2019;43(1):31-45. doi:10.4093/dmj.2019.0011
2. Cusi K, Isaacs S, Barb D, et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Primary Care and Endocrinology Clinical Settings: Co-Sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr Pract 2022;28(5):528-562. doi:10.1016/j.eprac.2022.03.010
3. Armstrong MJ, Gaunt P, Aithal GP, et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet 2016;387(10019):679-690. doi:10.1016/S0140-6736(15)00803-X
4. Belfort R, Harrison SA, Brown K, et al. A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N Engl J Med 2006;355(22):2297-2307. doi:10.1056/NEJMoa060326
5. Cusi K, Orsak B, Bril F, et al. Long-Term Pioglitazone Treatment for Patients With Nonalcoholic Steatohepatitis and Prediabetes or Type 2 Diabetes Mellitus: A Randomized Trial. Ann Intern Med 2016;165(5):305-315. doi:10.7326/M15-1774
6. Newsome PN, Buchholtz K, Cusi K, et al. A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis. N Engl J Med 2021;384(12):1113-1124. doi:10.1056/NEJMoa2028395
7. Patel Chavez C, Cusi K, Kadiyala S. The Emerging Role of Glucagon-like Peptide-1 Receptor Agonists for the Management of NAFLD. J Clin Endocrinol Metab 2022;107(1):29-38. doi:10.1210/clinem/dgab578
Other Complications of Diabetes Mellitus
Diabetic foot complications (skin changes, ulceration, infection, gangrene) are common and are attributable to vascular disease, neuropathy, and relative immunosuppression. These complications can lead to lower extremity amputations.
Certain musculoskeletal disorders are more common in patients with diabetes, including muscle infarction, carpal tunnel syndrome, Dupuytren contracture, adhesive capsulitis, and sclerodactyly.
Patients with diabetes may also develop
Ophthalmologic disease unrelated to diabetic retinopathy (eg, cataracts, glaucoma, corneal abrasions, optic neuropathy)
Hepatobiliary diseases (eg, cirrhosis, gallstones)
Dermatologic disease (eg, tinea infections, lower-extremity ulcers, diabetic dermopathy, necrobiosis lipoidica diabeticorum, diabetic systemic sclerosis, vitiligo, granuloma annulare, acanthosis nigricans [a sign of insulin resistance])


A patient with diabetes often develops microvascular disease, which may impair skin healing, so that even minor breaks in skin integrity can develop into deeper ulcers and easily become infected, particularly in the lower extremities.
© Springer Science+Business Media


Necrobiosis lipoidica is characteristic but not diagnostic of diabetes. Lesions most often appear on the legs and begin as erythematous papules that develop into atrophic, waxy, and yellow or brown lesions.
Photo provided by Thomas Habif, MD.


Acanthosis nigricans is skin thickening and pigmentation most typically developing in the axillae and nape of the neck (top); in people with dark skin, the skin may have a leathery appearance (bottom). It is most often a skin manifestation of impaired glucose tolerance, but it may reflect internal cancer, especially if onset is rapid and distribution is widespread.
Photos provided by Thomas Habif, MD.

This image shows erythematous bumps arranged in a ring or circular pattern on the torso of a patient with diabetes.
SCIENCE PHOTO LIBRARY
A patient with diabetes often develops microvascular disease, which may impair skin healing, so that even minor breaks in skin integrity can develop into deeper ulcers and easily become infected, particularly in the lower extremities.
© Springer Science+Business Media
Necrobiosis lipoidica is characteristic but not diagnostic of diabetes. Lesions most often appear on the legs and begin as erythematous papules that develop into atrophic, waxy, and yellow or brown lesions.
Photo provided by Thomas Habif, MD.
Acanthosis nigricans is skin thickening and pigmentation most typically developing in the axillae and nape of the neck (top); in people with dark skin, the skin may have a leathery appearance (bottom). It is most often a skin manifestation of impaired glucose tolerance, but it may reflect internal cancer, especially if onset is rapid and distribution is widespread.
Photos provided by Thomas Habif, MD.
This image shows erythematous bumps arranged in a ring or circular pattern on the torso of a patient with diabetes.
SCIENCE PHOTO LIBRARY
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Diabetes Association: Standards of Medical Care in DiabetesDiabetes Care 46 (Supplement 1): 1-291, 2023.
Davies MJ, Aroda VR, Collins BS, et al. Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2022;45(11):2753-2786. doi:10.2337/dci22-0034
Endocrine Society: Clinical Practice Guidelines: provides guidelines on evaluation and management of patients with diabetes as well as links to other information for clinicians
Holt RIG, DeVries JH, Hess-Fischl A, et al: The management of type 1 diabetes in adults. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 64(12):2609–2652, 2021. doi: 10.1007/s00125-021-05568-3
Powers MA, Bardsley JK, Cypress M, et al. Diabetes Self-management Education and Support in Adults With Type 2 Diabetes: A Consensus Report of the American Diabetes Association, the Association of Diabetes Care & Education Specialists, the Academy of Nutrition and Dietetics, the American Academy of Family Physicians, the American Academy of PAs, the American Association of Nurse Practitioners, and the American Pharmacists Association. Diabetes Care 2020;43(7):1636-1649. doi:10.2337/dci20-0023







