



- Overview of Glomerular Disorders
- Overview of Nephritic Syndrome
- Alport Syndrome
- Immunoglobulin A Nephropathy
- Postinfectious Glomerulonephritis (PIGN)
- Rapidly Progressive Glomerulonephritis (RPGN)
- Thin Basement Membrane Disease
- Overview of Nephrotic Syndrome
- Congenital Nephrotic Syndromes
- Diabetic Nephropathy
- Focal Segmental Glomerulosclerosis
- HIV-Associated Nephropathy
- Membranous Nephropathy
- Minimal Change Disease
- Fibrillary and Immunotactoid Glomerulopathies
- Lupus Nephritis
- Membranoproliferative Glomerulonephritis
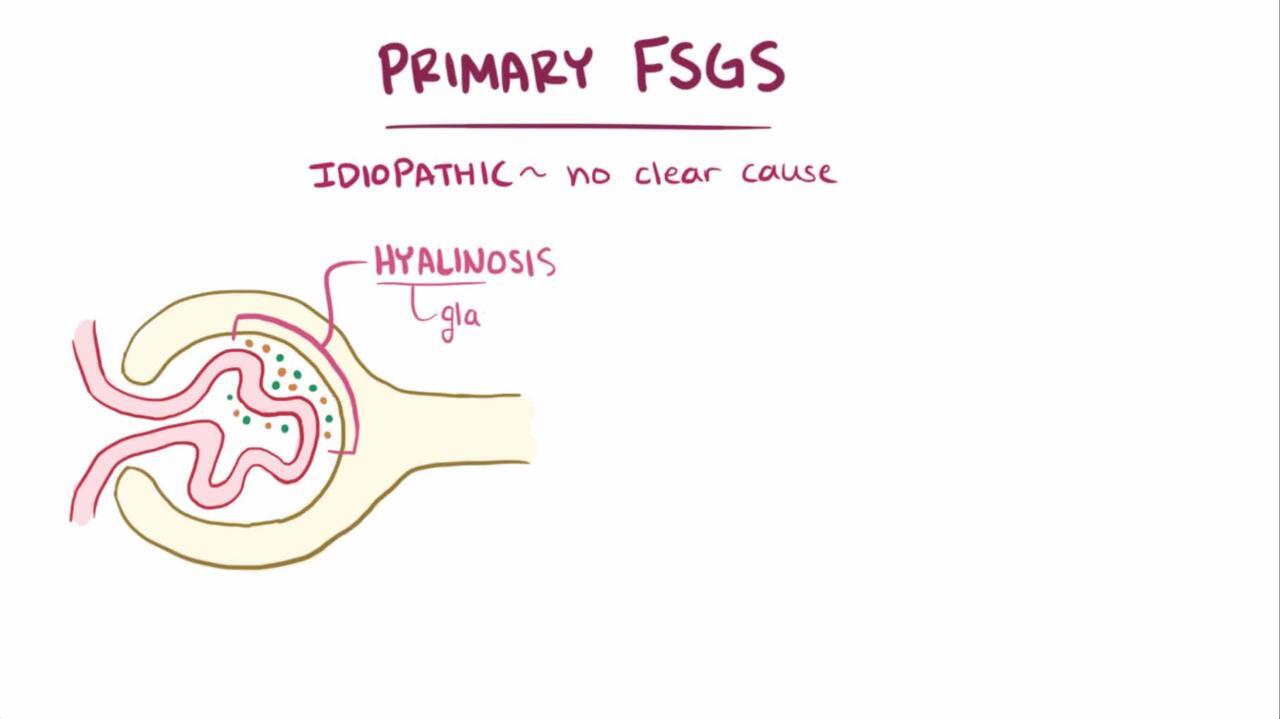
Focal segmental glomerulosclerosis is scattered (segmental) mesangial sclerosis that begins in some but not all (focal) glomeruli and eventually involves all glomeruli. It is most often idiopathic but may be secondary to use of heroin or other drugs, HIV infection, obesity, sickle cell disease, atheroembolic disease, or nephron loss (eg, in reflux nephropathy, subtotal nephrectomy, or renal dysgenesis). It manifests mainly in adolescents but also in young and middle-aged adults. Patients have insidious onset of proteinuria, mild hematuria, hypertension, and azotemia. Diagnosis is confirmed by renal biopsy. Treatment is with angiotensin inhibition and, for idiopathic disease, corticosteroids and sometimes other immunosuppressive agents.

")

")
")
")
")


Focal segmental glomerulosclerosis (FSGS) is now the most common cause of idiopathic (or primary) nephrotic syndrome among adults in the United States. It is especially common in Black men. Though usually idiopathic, FSGS can occur in association with other factors (secondary FSGS), including medications and illicit drugs (eg, heroin, lithium, interferon alfa, pamidronate, cyclosporine, or nonsteroidal anti-inflammatory drugs [causing among adults in the United States. It is especially common in Black men. Though usually idiopathic, FSGS can occur in association with other factors (secondary FSGS), including medications and illicit drugs (eg, heroin, lithium, interferon alfa, pamidronate, cyclosporine, or nonsteroidal anti-inflammatory drugs [causinganalgesic nephropathy]), atheroembolic disease affecting the kidneys, obesity, HIV infection (see HIV-associated nephropathy), and disorders causing nephron loss (eg, reflux nephropathy, subtotal nephrectomy, renal dysgenesis [eg, oligomeganephronia: renal hypoplasia with a decreased number of nephrons]). Familial cases exist.
In FSGS, the glomerular filtration barriers for size and molecular charge are defective, and proteinuria is typically nonselective, affecting high molecular-weight proteins (eg, immunoglobulins) as well as albumin. Kidneys tend to be small.In FSGS, the glomerular filtration barriers for size and molecular charge are defective, and proteinuria is typically nonselective, affecting high molecular-weight proteins (eg, immunoglobulins) as well as albumin. Kidneys tend to be small.

Symptoms and Signs of Focal Segmental Glomerulosclerosis
Patients with focal segmental glomerulosclerosis (FSGS) commonly present with heavy proteinuria, hypertension, renal dysfunction, edema, or a combination. Sometimes the only sign is asymptomatic proteinuria that is not in the nephrotic range. Microscopic hematuria is occasionally present.
Diagnosis of Focal Segmental Glomerulosclerosis
Renal biopsy, when possible, with immunostaining and electron microscopy
Focal segmental glomerulosclerosis (FSGS) is suspected in patients with nephrotic syndrome, proteinuria, or renal dysfunction with no obvious cause, particularly patients who have disorders or use illicit drugs or medications associated with FSGS.
Urinalysis is done and blood urea nitrogen (BUN), serum creatinine, and 24-hour urinary protein excretion or spot urinary protein:creatinine ratio are measured.Urinalysis is done and blood urea nitrogen (BUN), serum creatinine, and 24-hour urinary protein excretion or spot urinary protein:creatinine ratio are measured.
Diagnosis is confirmed by renal biopsy, which shows focal and segmental hyalinization of the glomeruli, often with immunostaining showing IgM and complement (C3) deposits in a nodular and coarse granular pattern. Electron microscopy reveals diffuse effacement of podocyte foot processes in idiopathic cases but may show patchy effacement in secondary cases. Global sclerosis may be visible, along with secondary atrophic glomeruli. Biopsy may be falsely negative if areas of focal abnormalities are not sampled.

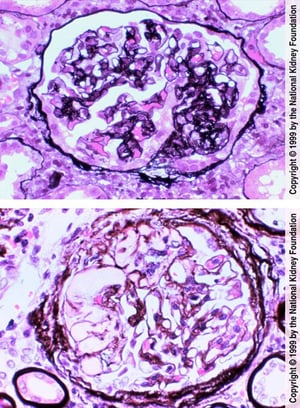
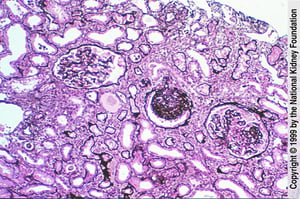
The top image shows the right side of the glomerulus. The glomerulus, which is segmentally sclerotic, is composed of obliterated capillary lumens and an increased amount of mesangial matrix. The rest of the glomerulus is normal (Jones silver stain, ×400). In the bottom image, hyalin, defined as smooth, glassy-appearing material, results from insudation (the opposite of exudation) of plasma proteins. It occurs frequently and is not diagnostic (Jones silver stain, ×400).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).

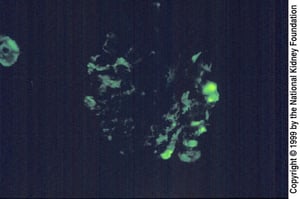
Immunofluorescence staining with anti-IgM demonstrates IgM in mesangium or in areas of hyalinosis (smooth, globular staining on right). IgM is thought to become trapped in areas of expanded mesangium and sclerosis (×200).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
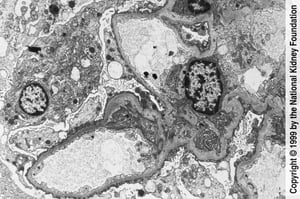
Extensive blunting and effacement of foot processes can be seen on transmission electron microscopy (×3000).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
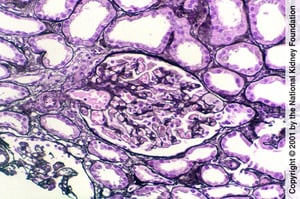
The central glomerulus in this biopsy specimen demonstrates global sclerosis. The finding is nonspecific and may develop in response to injury or aging (Jones silver stain, ×100).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
A tip lesion is segmental sclerosis localized to the glomerular pole where the tubule originates. It may be a marker of improved prognosis (Jones silver stain, ×200).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
The top image shows the right side of the glomerulus. The glomerulus, which is segmentally sclerotic, is composed of obliterated capillary lumens and an increased amount of mesangial matrix. The rest of the glomerulus is normal (Jones silver stain, ×400). In the bottom image, hyalin, defined as smooth, glassy-appearing material, results from insudation (the opposite of exudation) of plasma proteins. It occurs frequently and is not diagnostic (Jones silver stain, ×400).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Immunofluorescence staining with anti-IgM demonstrates IgM in mesangium or in areas of hyalinosis (smooth, globular staining on right). IgM is thought to become trapped in areas of expanded mesangium and sclerosis (×200).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Extensive blunting and effacement of foot processes can be seen on transmission electron microscopy (×3000).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
The central glomerulus in this biopsy specimen demonstrates global sclerosis. The finding is nonspecific and may develop in response to injury or aging (Jones silver stain, ×100).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
A tip lesion is segmental sclerosis localized to the glomerular pole where the tubule originates. It may be a marker of improved prognosis (Jones silver stain, ×200).
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
Treatment of Focal Segmental Glomerulosclerosis
Angiotensin inhibition
Corticosteroids and sometimes other immunosuppressive agents for idiopathic FSGS
Kidney transplantation for patients with end-stage kidney disease
Treatment often is not effective. Patients with FSGS should be treated with angiotensin inhibition (with an angiotensin-converting enzyme [ACE] inhibitor or an angiotensin II receptor blocker [ARB]) unless contraindicated by Treatment often is not effective. Patients with FSGS should be treated with angiotensin inhibition (with an angiotensin-converting enzyme [ACE] inhibitor or an angiotensin II receptor blocker [ARB]) unless contraindicated byangioedema or hyperkalemia. Patients with nephrotic syndrome should be treated with a statin.
In idiopathic FSGS, a trial of immunosuppressive therapy is indicated if proteinuria reaches the nephrotic range or if renal function worsens, especially if kidney biopsy reveals a tip lesion. In contrast, patients with secondary FSGS, collapsing FSGS, or advanced tubulointerstitial fibrosis on renal biopsy are generally not treated with immunosuppression because they tend to not respond; instead, the primary disorder is treated.
Immunosuppressive therapy
High-dose corticosteroids (eg, prednisone 1 mg/kg orally once a day or 2 mg/kg every other day) are recommended for at least 2 months, although some experts recommend use for up to 9 months. Response rates of 30 to 50% have been reported with prolonged therapy and vary by the histologic classification of FSGS. After a 2-week remission of proteinuria, the corticosteroid is slowly tapered over High-dose corticosteroids (eg, prednisone 1 mg/kg orally once a day or 2 mg/kg every other day) are recommended for at least 2 months, although some experts recommend use for up to 9 months. Response rates of 30 to 50% have been reported with prolonged therapy and vary by the histologic classification of FSGS. After a 2-week remission of proteinuria, the corticosteroid is slowly tapered over≥ 2 months. Secondary and familial cases, collapsing FSGS, and advanced tubulointerstitial fibrosis are more likely to be corticosteroid-resistant.
If only slight improvement or relapse occurs with corticosteroid therapy, remission may be induced with a calcineurin inhibitor (eg, cyclosporine or tacrolimus) for at least 6 months. Although calcineurin inhibitors have been studied more than tacrolimus for FSGS, some clinicians prefer tacrolimus because it is commonly used for other glomerular diseases and there is a lower risk of cosmetic side effects (eg, hirsutism, gingival hyperplasia). In selected cases, mycophenolate mofetil may be used as an alternative. If only slight improvement or relapse occurs with corticosteroid therapy, remission may be induced with a calcineurin inhibitor (eg, cyclosporine or tacrolimus) for at least 6 months. Although calcineurin inhibitors have been studied more than tacrolimus for FSGS, some clinicians prefer tacrolimus because it is commonly used for other glomerular diseases and there is a lower risk of cosmetic side effects (eg, hirsutism, gingival hyperplasia). In selected cases, mycophenolate mofetil may be used as an alternative.
In patients with contraindications to high-dose corticosteroids (eg, diabetes, osteoporosis), a calcineurin inhibitor can be given along with a lower dose of corticosteroids (eg, prednisone 0.15 mg/kg orally once a day). In patients with contraindications to high-dose corticosteroids (eg, diabetes, osteoporosis), a calcineurin inhibitor can be given along with a lower dose of corticosteroids (eg, prednisone 0.15 mg/kg orally once a day).
An alternative is plasma exchange in combination with immunosuppression.

Prognosis for Focal Segmental Glomerulosclerosis
Prognosis is poor. Spontaneous remissions occur in < 10% of patients. Renal failure occurs in > 50% of patients within 10 years; in 20%, end-stage kidney disease occurs within 2 years despite treatment and is more likely if patients have significant tubulointerstitial fibrosis. The disorder is more rapidly progressive in adults than in children.
The presence of segmental sclerosis consistently at the glomerular pole where the tubule originates (tip lesion) may portend a more favorable response to corticosteroid therapy. Another variant, in which the capillary walls are wrinkled or collapsed (collapsing FSGS, which is typical in association with IV drug abuse or HIV infection), suggests more severe disease and rapid progression to renal failure. Pregnancy may exacerbate FSGS.
FSGS may recur after kidney transplantation; proteinuria sometimes returns within hours of transplantation. Of patients whose transplant was for end-stage kidney disease caused by FSGS, about 8 to 30% lose their graft due to recurrent FSGS; risk is highest in young children, patients who are not Black, patients who develop renal failure < 3 years after disease onset, patients with mesangial proliferation, and patients with repeat transplants when the diagnosis before the first transplant was primary FSGS. Familial forms of FSGS rarely recur after transplantation.

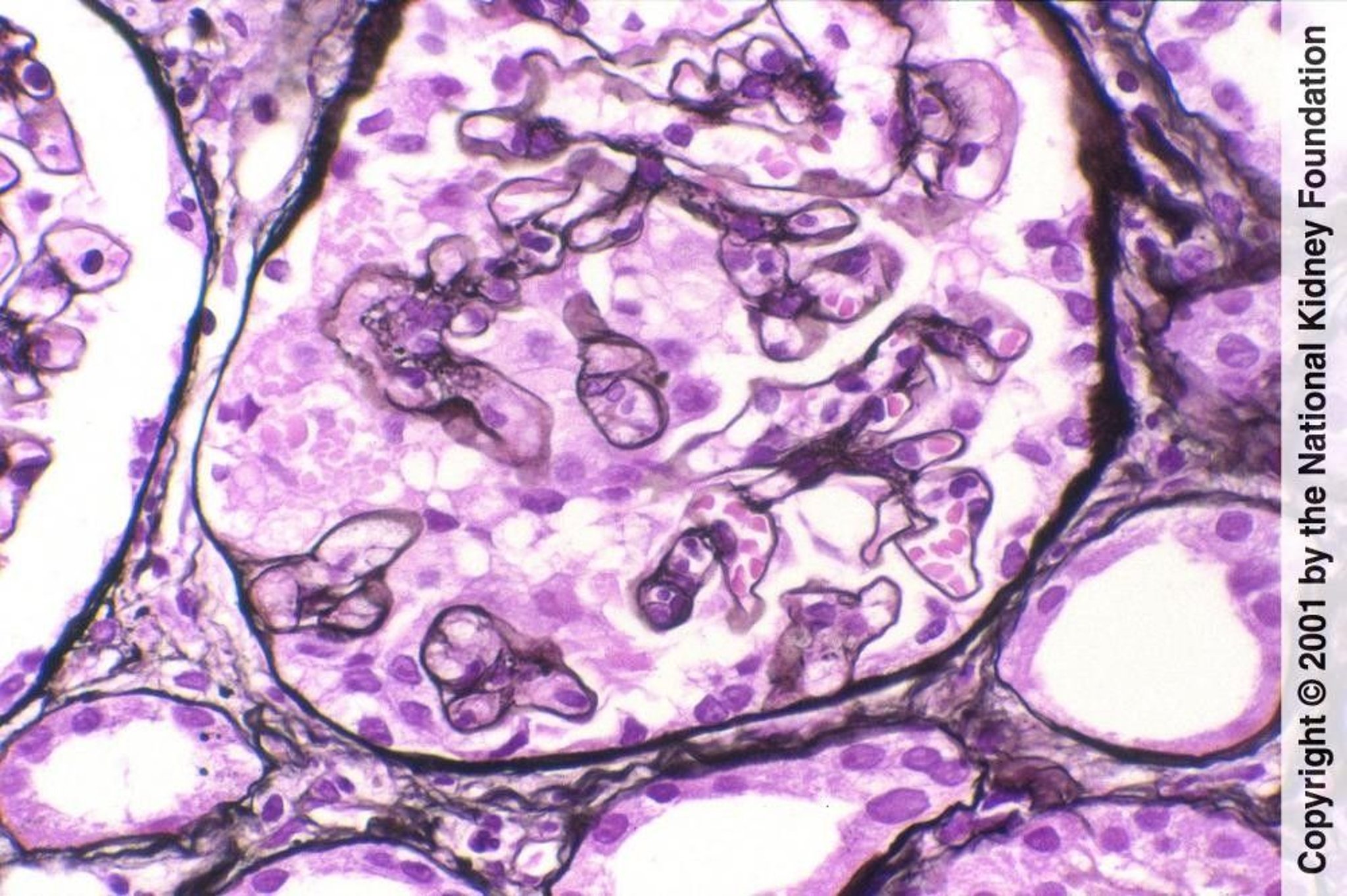
Image provided by Agnes Fogo, MD, and the American Journal of Kidney Diseases' Atlas of Renal Pathology (see www.ajkd.org).
People who use heroin and develop nephrotic syndrome due to FSGS can experience complete remission if they cease taking heroin early in the disease.
Key Points
Suspect focal segmental glomerulosclerosis if patients have nephrotic syndrome, proteinuria, or renal dysfunction with no obvious cause, particularly patients who have disorders or use illicit drugs or medications associated with FSGS.
When possible, confirm FSGS by renal biopsy with immunostaining and electron microscopy.
Consider treatment with corticosteroids and possibly a calcineurin inhibitor (eg, cyclosporine or tacrolimus) or alternatively, mycophenolate mofetil, if FSGS is idiopathic and proteinuria reaches the nephrotic range or renal function worsens.Consider treatment with corticosteroids and possibly a calcineurin inhibitor (eg, cyclosporine or tacrolimus) or alternatively, mycophenolate mofetil, if FSGS is idiopathic and proteinuria reaches the nephrotic range or renal function worsens.







