



Aortic dissection is the surging of blood through a tear in the aortic intima with separation of the intima and media and creation of a false lumen (channel). The intimal tear may be a primary event or secondary to hemorrhage within the media. The dissection may occur anywhere along the aorta and extend proximally or distally into other arteries. Hypertension is an important contributor. Symptoms and signs include abrupt onset of tearing chest or back pain, and dissection may result in aortic regurgitation and compromised circulation in branch arteries. Diagnosis is by imaging tests (eg, transesophageal echocardiography, CT angiography, MRI, contrast aortography). Treatment involves strict blood pressure control and serial imaging to monitor progression of dissection. Surgical repair of the aorta and placement of a synthetic graft are needed for ascending aortic dissection and for certain descending aortic dissections. Endovascular stent grafts are an option for selected patients with descending dissections, especially when dissection involves the descending thoracic aorta.

")





Patients who are Black, male, or older, and patients with hypertension are especially at risk for aortic dissection (1, 2). Peak incidence occurs at age 50 to 65 years in the general population and at age 20 to 40 years for patients with congenital connective tissue disorders (eg, Marfan syndrome, Ehlers-Danlos syndrome).

Classification of aortic dissection
Aortic dissections are classified anatomically.
The DeBakey classification system is most widely used (3):
Type I (Majority of dissections): These dissections start in the ascending aorta and extend at least to the aortic arch and sometimes beyond.
Type II: These dissections start in and are confined to the ascending aorta (proximal to the brachiocephalic or innominate artery).
Type III: These dissections start in the descending thoracic aorta just beyond the origin of the left subclavian artery and extend distally or, less commonly, proximally. Type IIIa dissections originate distal to the left subclavian artery and are confined to the thoracic aorta. Type IIIb dissections originate distal to the left subclavian artery and extend below the diaphragm.
The Stanford system is simpler:
Type A: These dissections involve the ascending aorta.
Type B: These dissections are confined to the descending thoracic aorta (distal to the left subclavian artery).


© 2017 Elliot K. Fishman, MD.
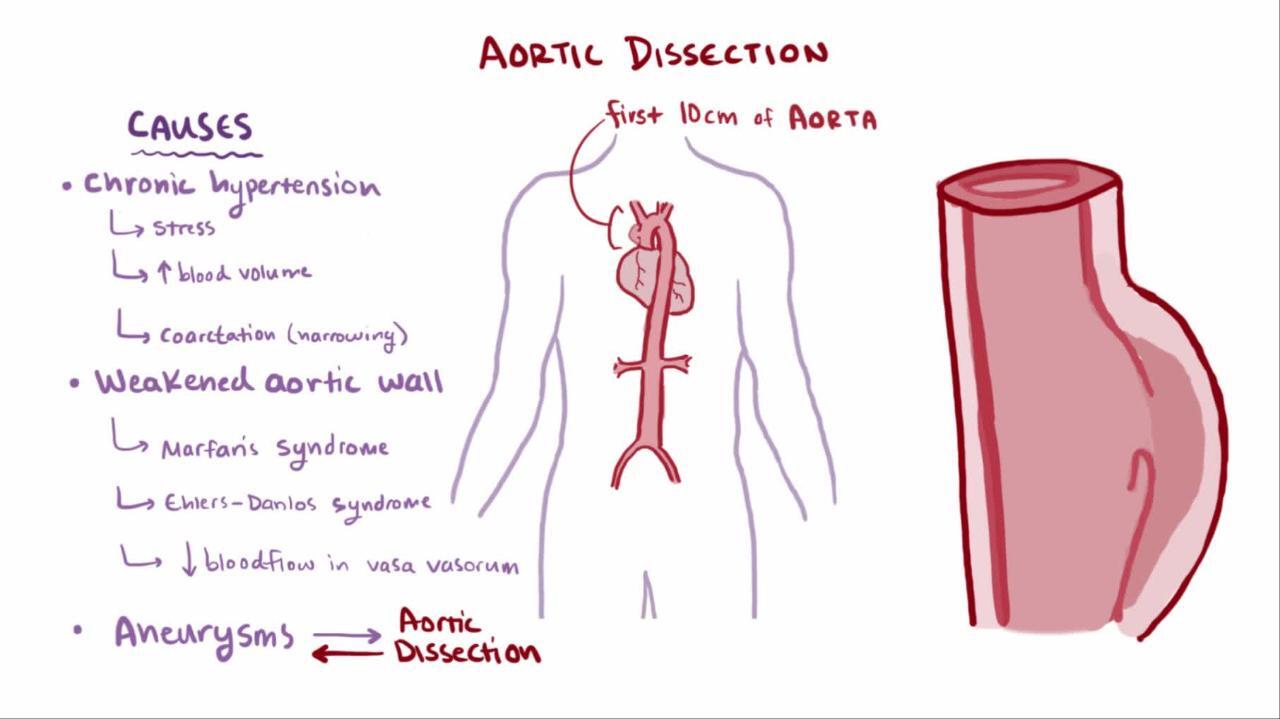
Although dissection may originate anywhere along the aorta, it occurs most commonly at areas of greatest hydraulic stress, which are the
Right lateral wall of the ascending aorta (within 5 cm of the aortic valve)
Proximal segment of the descending aorta (just beyond the origin of the left subclavian artery)
Rarely, dissection is confined to individual arteries (eg, coronary or carotid arteries), typically in pregnant or postpartum women.
General references
1. Huynh N, Thordsen S, Thomas T, et al. Clinical and pathologic findings of aortic dissection at autopsy: Review of 336 cases over nearly 6 decades. Am Heart J 2019;209:108-115. doi:10.1016/j.ahj.2018.11.006
2. Janus SE, Chami T, Mously H, et al. Proportionate and Absolute Vascular Disease Mortality by Race and Sex in the United States From 1999 to 2019. J Am Heart Assoc 2022;11(15):e025276. doi:10.1161/JAHA.121.025276
3. Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2022;146(24):e334-e482. doi:10.1161/CIR.0000000000001106
Etiology of Aortic Dissection
Aortic dissections often occur in patients with preexisting degeneration of the aortic media. Causes and risk factors include connective tissue disorders, atherosclerotic disease, systemic rheumatic diseases, and injury (see table Conditions Contributing to Aortic Dissection).
Conditions Contributing to Aortic Dissection
Category | Examples |
|---|---|
Atherosclerotic risk factors | Cocaine Smoking |
Connective tissue disorders, congenital or hereditary | Cystic medial necrosis Loeys-Dietz syndrome Familial thoracic aortic aneurysm |
Iatrogenic | Aortic catheterization Aortic valve surgery |
Systemic rheumatic diseases | |
Trauma | Deceleration injuries |
Atherosclerotic risk factors, notably hypertension, contribute in more than two-thirds of patients. After rupture of the intima, which is a primary event in some patients and secondary to hemorrhage within the media in others, blood flows into the media, creating a false channel that extends distally or, less commonly, proximally along the artery.
Pathophysiology of Aortic Dissection
The pathophysiologic sequence of aortic dissections involves
Aortic wall inflammation
Apoptosis of vascular smooth muscle cells
Degeneration of aortic media
Elastin disruption
Vessel dissection
Dissections may communicate back with the true aortic lumen through intimal rupture at a distal site, maintaining systemic blood flow.
Serious consequences of aortic dissection are common and include
Compromise of the blood supply of arteries that branch off the aorta (including coronary arteries)
Aortic valvular dilation and regurgitation
Fatal rupture of the aorta through the adventitia into the pericardium, right atrium, or left pleural space
Acute dissections and those present < 2 weeks are most likely to cause these complications. Risk decreases at ≥ 2 weeks if evidence indicates thrombosis of the false lumen and loss of communication between the true and false lumina.
Variants of dissection are thought to be precursors of classic aortic dissection. Variants of aortic dissection include
Separation of the intima and media by intramural hematoma without a clear intimal tear or flap
Intimal tear and bulge without a hematoma or false lumen
Dissection or hematoma caused by ulceration of atherosclerotic plaque

Symptoms and Signs of Aortic Dissection
Typically in aortic dissection, excruciating precordial or interscapular pain, often described as tearing or ripping, occurs abruptly (1). The pain frequently migrates from the original location as the dissection extends along the aorta. Up to 20% of patients present with syncope due to severe pain, aortic baroreceptor activation, extracranial cerebral artery obstruction, or cardiac tamponade. Hypotension and tachycardia could indicate active bleeding.
Occasionally, patients present with symptoms of malperfusion (ischemia due to the obstruction resulting from dissection), such as stroke, myocardial infarction, intestinal infarction, renal insufficiency, paraparesis, or paraplegia, due to interruption of the blood supply to a particular vascular bed, including the spinal cord, brain, heart, kidneys, intestine, or extremities. The interruption in blood supply is most often due to acute distal arterial obstruction by the false lumen.
Approximately 20 to 30% of patients have partial or complete deficits of major arterial pulses, which may wax and wane (1). Limb blood pressures may differ, sometimes by > 30 mm Hg; this finding suggests a poor prognosis.
A murmur of aortic regurgitation is often heard in patients with proximal dissection. Peripheral signs of aortic regurgitation may be present. Rarely, heart failure results from severe acute aortic regurgitation. Cardiac tamponade may cause pulsus paradoxus and jugular venous distention.
Leakage of blood or inflammatory serous fluid into the left pleural space may lead to signs of pleural effusion.
Occlusion of a limb artery may cause signs of peripheral ischemia or neuropathy.
Renal artery occlusion may cause oliguria or anuria.
Pearls & Pitfalls
|
Symptoms and signs reference
1. Pape LA, Awais M, Woznicki EM, et al. Presentation, Diagnosis, and Outcomes of Acute Aortic Dissection: 17-Year Trends From the International Registry of Acute Aortic Dissection. J Am Coll Cardiol 2015;66(4):350-358. doi:10.1016/j.jacc.2015.05.029
Diagnosis of Aortic Dissection
Transesophageal echocardiography (TEE), CT angiography (CTA), or magnetic resonance angiography (MRA)
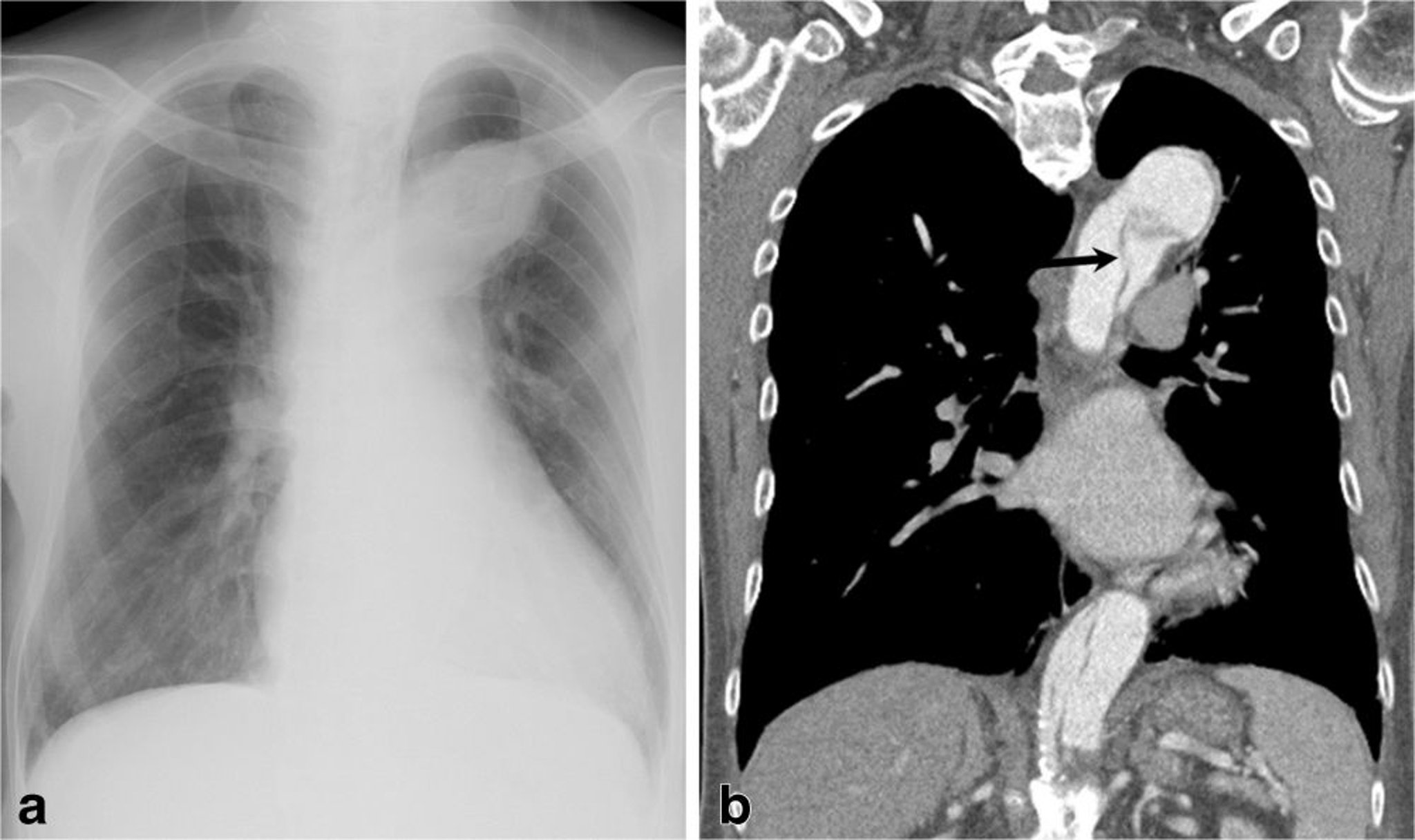
Aortic dissection must be considered in any patient with chest pain, thoracic back pain, unexplained syncope, unexplained abdominal pain, stroke, or acute-onset heart failure, especially when pulses or blood pressures in the limbs are unequal. Such patients require a chest radiograph; the mediastinal shadow is often widened, usually with a localized bulge signifying the site of origin. Left pleural effusion is common.
Patients presenting with acute chest pain, electrocardiography (ECG) changes of acute inferior myocardial infarction, and a previously undocumented murmur of aortic regurgitation (AR) are of particular concern for a type I aortic dissection into the right coronary artery (causing inferior myocardial infarction), and the aortic valve (causing AR).

© Springer Science+Business Media

© 2017 Elliot K. Fishman, MD.
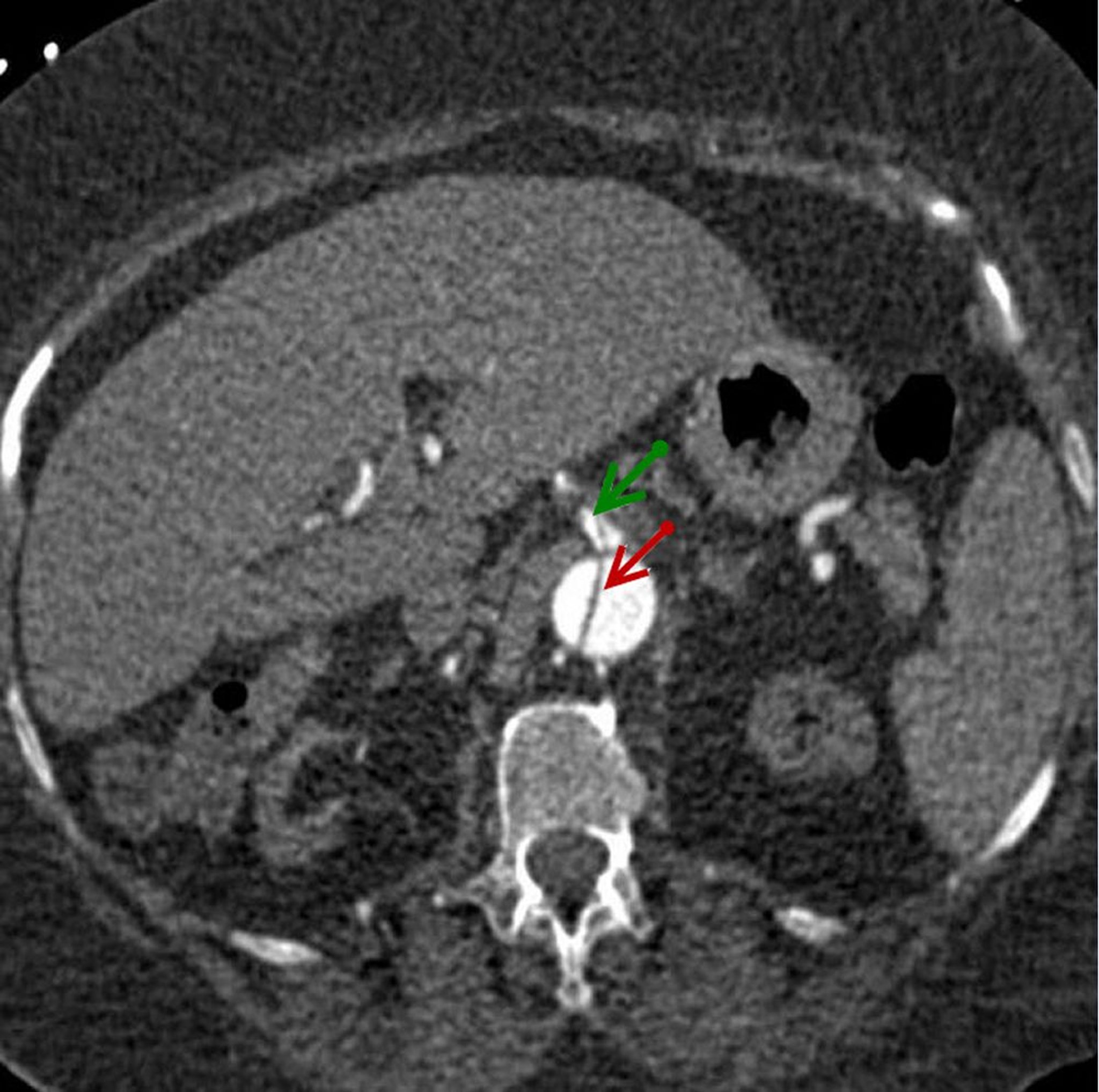
If the chest radiograph suggests dissection, TEE, CTA, or MRA is done immediately after the patient is stabilized. Findings of an intimal flap and double lumina confirm dissection.
Multiplanar TEE is 97 to 99% sensitive and, with M-mode echocardiography, is nearly 100% specific. It can be done at the bedside in < 20 minutes and does not require contrast agents. However, CTA is typically the first-line imaging modality because it is often available more rapidly and widely than TEE. CTA sensitivity has been reported in the range of 90 to 100%, and specificity of CTA is 87 to 100% (1).
MRA has nearly 100% sensitivity and specificity for aortic dissection. But it is time-consuming and ill-suited for emergencies. MRA is best used when dissection is suspected in patients who are stable and have subacute or chronic chest pain.
Contrast aortography is an option if surgery is being considered. In addition to identifying the origin and extent of dissection, severity of aortic regurgitation, and extent of involvement of the aorta’s major branches, aortography helps determine whether simultaneous coronary artery bypass surgery is needed.
Echocardiography should be done to check for aortic regurgitation and thus determine whether the aortic valve should be repaired or replaced concomitantly.
Electrocardiography (ECG) is nearly universally done. However, findings range from normal to markedly abnormal (in acute coronary artery occlusion or aortic regurgitation), so the test is not diagnostically helpful for dissection itself.
Serum creatine kinase-MB and troponin levels may help distinguish aortic dissection from myocardial infarction, except when dissection causes myocardial infarction.
Routine laboratory tests may detect slight leukocytosis and anemia if blood has leaked from the aorta. Increased lactate dehydrogenase may be a nonspecific sign of celiac or mesenteric arterial trunk involvement.
A cardiothoracic surgeon should be consulted early during the diagnostic evaluation.
Diagnosis reference
1. Expert Panel on Cardiac Imaging, Kicska GA, Hurwitz Koweek LM, et al. ACR Appropriateness Criteria® Suspected Acute Aortic Syndrome. J Am Coll Radiol 2021;18(11S):S474-S481. doi:10.1016/j.jacr.2021.09.004
Treatment of Aortic Dissection
Beta-blockers and other medications to control blood pressure
Usually endovascular repair or open surgical repair
Patients who do not immediately die of aortic dissection should be admitted to an intensive care unit with intra-arterial blood pressure monitoring and an indwelling urethral catheter to monitor urine output. Blood should be typed and cross-matched for 4 to 6 units of packed red blood cells when surgery is likely. Patients who are hemodynamically unstable should be intubated.
Medical management
Medications to decrease arterial pressure, arterial shear stress, ventricular contractility, and pain are started immediately to maintain systolic blood pressure at ≤ 120 mm Hg (or the lowest level compatible with adequate cerebral, coronary, and renal perfusion) and to maintain a target heart rate of 60 to 80 beats per minute.
A beta-blocker is usually the first-line medication for heart rate and blood pressure control. Options include
Metoprolol tartrate IV Metoprolol tartrate IV
Esmolol IV Esmolol IV
Labetalol (an alpha- and beta-adrenergic blocker) IV Labetalol (an alpha- and beta-adrenergic blocker) IV
Alternatively, nondihydropyridine calcium channel blockers (eg, verapamil, diltiazem) can be used to control blood pressure and heart rate in patients who do not tolerate beta-blockers.Alternatively, nondihydropyridine calcium channel blockers (eg, verapamil, diltiazem) can be used to control blood pressure and heart rate in patients who do not tolerate beta-blockers.
If systolic blood pressure remains > 110 mm Hg despite use of beta-blockers or nondihydropyridine calcium channel blockers, nitroprusside can be given in a constant IV infusion, titrated as necessary to control blood pressure. 110 mm Hg despite use of beta-blockers or nondihydropyridine calcium channel blockers, nitroprusside can be given in a constant IV infusion, titrated as necessary to control blood pressure.Nitroprusside should not be given without a beta-blocker or nondihydropyridine calcium channel blocker because reflex sympathetic activation in response to vasodilation can increase ventricular inotropy and aortic shear stress, worsening the dissection.
Pearls & Pitfalls
|
Surgical repair
For a dissection of the descending aorta, a trial of medical therapy alone is appropriate for an uncomplicated, stable dissection confined to the descending aorta (type B). Endovascular repair is warranted in patients with complications (malperfusion, meaning ischemia due to obstruction secondary to the dissection; persistent hypertension and pain; rapidly enlarging aortic diameter; extension of the dissection; and rupture). Surgery is also best for acute distal dissections in patients with Marfan syndrome.
For ascending aorta dissections, surgery is virtually always indicated due to the risk of life-threatening complications. Surgery usually involves open repair and replacement, although endovascular therapy can be used in certain circumstances when patients are not candidates for open repair.
The extent of repair depends upon the reason for repair and the anatomic nature of the dissection.
The goal of surgery is to obliterate entry into the false channel and reconstitute the aorta with a synthetic graft. If present, severe aortic regurgitation must be treated by resuspending the aortic leaflets or replacing the valve. Surgical outcomes are best with early, aggressive intervention. Mortality rates are approximately 20% (1). Predictors of poor outcome include
Hypotension
Renal failure
Age > 70 years
Abrupt onset of chest pain
Pulse deficit
ST-segment elevation on ECG
Stent grafts that seal entry to the false lumen and improve patency of the true lumen, balloon fenestration (in which an opening is made in the dissection flap that separates the true and false lumina), or both may be less invasive alternatives for patients with type B dissection if peripheral ischemic complications develop. Some endovascular devices (Gore Ascending Stent Graft) are available for compassionate use in patients with type A dissections who have contraindications to open surgical repair.
Complications of surgery include death, stroke (due to emboli), paraplegia (due to spinal cord ischemia), acute renal failure (especially if dissection includes renal arteries) and endoleak (leakage of blood back into the aneurysmal sac).
The most important late sequellae include redissection, formation of localized aneurysms in the weakened aorta, and progressive aortic regurgitation. These complications may require surgical or endovascular repair.
Long-term management
All patients, including those treated by surgery or endovascular methods, are given long-term antihypertensive therapy, usually including beta-blockers, nondihydropyridine calcium channel blockers, and angiotensin-converting enzyme (ACE) inhibitors. Almost any combination of antihypertensives is acceptable; exceptions are those that act mainly by vasodilation (eg, hydralazine, minoxidil) and beta-blockers that have intrinsic sympathomimetic action (eg, acebutolol, pindolol). Avoidance of strenuous physical activity is often recommended. , usually including beta-blockers, nondihydropyridine calcium channel blockers, and angiotensin-converting enzyme (ACE) inhibitors. Almost any combination of antihypertensives is acceptable; exceptions are those that act mainly by vasodilation (eg, hydralazine, minoxidil) and beta-blockers that have intrinsic sympathomimetic action (eg, acebutolol, pindolol). Avoidance of strenuous physical activity is often recommended.
CT may be done before discharge and repeated at 6 months and 1 year, and then every 1 to 2 years.
After repair of a dissection, the aorta should be monitored for the rest of the patient's life. The weakened aorta may develop aneurysmal degeneration above or below the surgical repair or re-dissect. For these reasons, continued surveillance is indicated.
Treatment reference
1. Pape LA, Awais M, Woznicki EM, et al. Presentation, Diagnosis, and Outcomes of Acute Aortic Dissection: 17-Year Trends From the International Registry of Acute Aortic Dissection. J Am Coll Cardiol 2015;66(4):350-358. doi:10.1016/j.jacc.2015.05.029
Prognosis for Aortic Dissection
About 20% of patients with aortic dissection die before reaching the hospital. Without treatment, mortality rate is approximately 1 to 2% per hour after symptom onset. Without surgery, mortality is > 50% at 1 month (1).
Hospital mortality rate for treated patients is about 20% for type A dissection and 10% for type B dissection (2). One of the largest international registry databases reported survival rates of > 90 percent for type A dissections treated surgically at 1 and 3 years postdischarge. However, the 3-year survival rate of patients with type B dissection was 78% for those treated with medical management alone.
Prognosis references
1. Tsai TT, Nienaber CA, Eagle KA. Acute aortic syndromes. Circulation 2005;112(24):3802-3813. doi:10.1161/CIRCULATIONAHA.105.534198
2. Evangelista A, Isselbacher EM, Bossone E, et al. Insights From the International Registry of Acute Aortic Dissection: A 20-Year Experience of Collaborative Clinical Research. Circulation 2018;137(17):1846-1860. doi:10.1161/CIRCULATIONAHA.117.031264
Key Points
Aortic dissection may originate anywhere along the aorta but is most common at the proximal ascending aorta (within 5 cm of the aortic valve) or the descending thoracic aorta just beyond the origin of the left subclavian artery.
Dissection can present in patients with preexisting degeneration of the aortic media (eg, caused by connective tissue disorders, injury) but hypertension is commonly also involved.
Patients typically have excruciating, tearing precordial or interscapular pain.
Other manifestations depend on whether the aortic root and/or branches of the aorta are affected, and the presence and location of any rupture; heart failure, organ ischemia, and hemorrhagic shock may occur.
Diagnose using transesophageal echocardiography (TEE), computed tomography angiography (CTA), or magnetic resonance angiography (MRA).
Immediately give beta-blockers and other medications as needed to control blood pressure and heart rate.
Medical therapy alone is appropriate for uncomplicated, stable dissection confined to the descending aorta; other cases require surgery.







