



A thoracic aortic diameter ≥ 50% larger than normal is considered an aneurysm (normal diameter varies by location). Most thoracic aortic aneurysms do not cause symptoms, although some patients have chest or back pain; other symptoms and signs are usually the result of complications (eg, dissection, compression of adjacent structures, thromboembolism, rupture). Risk of rupture is proportional to the size of the aneurysm. Diagnosis is made by CT angiography or transesophageal echocardiography (TEE). Treatment is endovascular stent grafting or surgery.
Topic Resources


(See also Overview of Aortic Aneurysms.)
Thoracic aortic aneurysms (TAAs) are abnormal dilatations of the aorta above the diaphragm. TAAs account for one-fourth of aortic aneurysms. Males and females are affected equally.
Locations of TAAs (1) include
Ascending thoracic aorta (between the aortic root and brachiocephalic, or innominate, artery): 46%
Aortic arch (including the brachiocephalic, carotid, and subclavian arteries): 21%
Descending thoracic aorta (distal to the left subclavian artery): 35%
Complications
Complications of TAAs include
Compression or erosion into adjacent structures
Leak or rupture
Thromboembolism
Aneurysms of the ascending aorta sometimes affect the aortic root, causing aortic valve regurgitation, or occlusion of the coronary arterial ostia, causing angina, myocardial infarction, or syncope.
General reference
1. Gouveia E Melo R, Silva Duarte G, Lopes A, et al. Incidence and Prevalence of Thoracic Aortic Aneurysms: A Systematic Review and Meta-analysis of Population-Based Studies. Semin Thorac Cardiovasc Surg 2022;34(1):1-16. doi:10.1053/j.semtcvs.2021.02.029
Etiology of Thoracic Aortic Aneurysms
Most thoracic aortic aneurysms result from
Risk factors for both thoracic aortic aneurysms and aortic dissections include prolonged hypertension, dyslipidemia, and smoking. Additional risk factors for TAAs include presence of aneurysms elsewhere in the body, infection, aortitis, and older age (peak incidence at age 65 to 70 years).
Congenital connective tissue disorders (eg, Marfan syndrome, Ehlers-Danlos syndrome, Loeys-Dietz syndrome) cause cystic medial necrosis, a degenerative change that leads to TAAs complicated by aortic dissection and by widening of the proximal aorta and aortic valve (annuloaortic ectasia), which causes aortic regurgitation. Marfan syndrome causes 50% of cases of annuloaortic ectasia, but cystic medial necrosis and its complications can occur in young people even if no congenital connective tissue disorder is present.
Infected (mycotic) TAAs result from hematogenous spread of systemic or local infections (eg, sepsis, pneumonia), lymphangitic spread (eg, tuberculosis), or direct extension (eg, in osteomyelitis or pericarditis). Bacterial endocarditis and tertiary syphilis are uncommon causes.
TAAs occur in some vasculitic disorders (eg, giant cell arteritis, Takayasu arteritis, granulomatosis with polyangiitis).
Blunt chest trauma can cause a pseudoaneurysm (false aneurysm) due to injury to the aortic wall resulting in a communication between the arterial lumen and overlying connective tissue and blood leaking outside the confines of the aorta; a blood-filled cavity forms outside the vessel wall and seals the leak as it thromboses).
Symptoms and Signs of Thoracic Aortic Aneurysms
Most thoracic aortic aneurysms are asymptomatic until complications (eg, thromboembolism, rupture, aortic regurgitation, dissection) develop. However, compression of adjacent structures can cause back pain (due to compression of vertebra), cough or wheezing (due to compression of the tracheobronchial tree), dysphagia (due to esophageal compression), hoarseness (due to left recurrent laryngeal or vagus nerve compression), chest pain (due to coronary artery compression), and superior vena cava syndrome (due to compression of the central veins or superior vena cava).
Erosion of aneurysms into the lungs causes hemoptysis or pneumonitis; erosion into the esophagus (aortoesophageal fistula) causes massive hematemesis.
Dissection manifests with tearing chest pain, often radiating to the back between the shoulder blades.
Thromboembolism may cause stroke, abdominal pain (due to mesenteric ischemia), or extremity pain.
Ruptured TAA that is not immediately fatal manifests with severe chest or back pain and hypotension or shock. Exsanguination due to rupture most commonly occurs into the pleural or pericardial space.
Additional signs include Horner syndrome (miosis, ptosis, anhidrosis) due to compression of sympathetic ganglia, palpable downward pull of the trachea with each cardiac contraction (tracheal tug), and tracheal deviation. Visible or palpable chest wall pulsations, occasionally more prominent than the left ventricular apical impulse, are unusual but may occur.
Syphilitic aneurysms of the aortic root classically lead to aortic regurgitation and inflammatory stenosis of the coronary artery ostia, which may manifest as chest pain due to myocardial ischemia. Syphilitic aneurysms do not dissect.
Diagnosis of Thoracic Aortic Aneurysms
Incidental radiograph finding
Confirmation by CT angiography (CTA), magnetic resonance angiography (MRA), or transesophageal echocardiography (TEE)
Thoracic aortic aneurysms are usually first suspected when a chest radiograph incidentally shows a widened mediastinum or enlargement of the aortic knob. However, chest radiography has poor sensitivity for TAA and is not a reliable diagnostic tool (eg, in patients with chest pain and suspected aortic aneurysm). Chest radiograph abnormalities or symptoms and signs suggesting an aneurysm should be followed up with a cross-sectional imaging test; choice among these tests is based on availability and local experience (1).

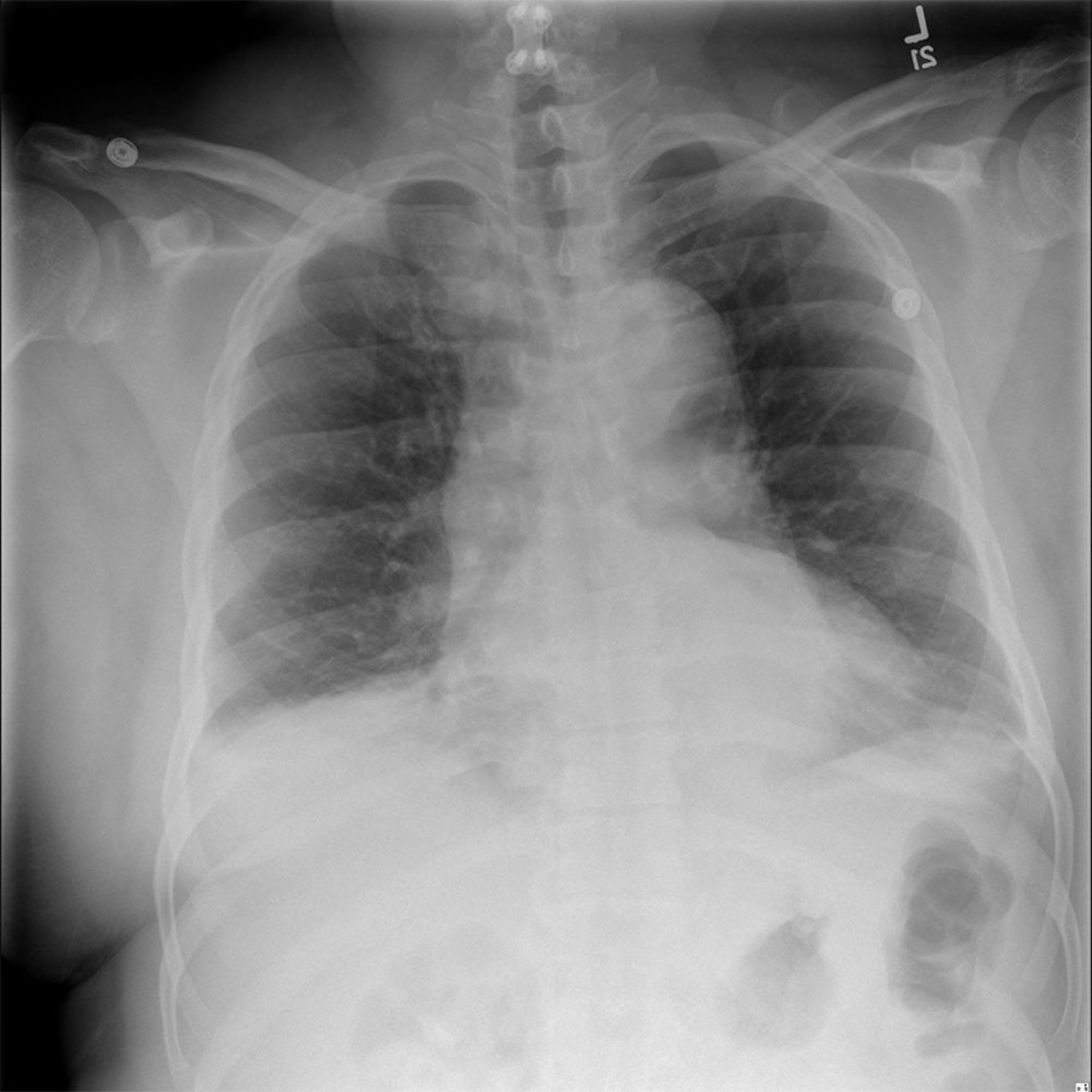
© 2017 Elliot K. Fishman, MD.

© 2017 Elliot K. Fishman, MD.
If rupture is suspected, TEE (for ascending dissection) or CTA, depending on availability, should be done immediately. Chest CTA can delineate aneurysm size and proximal or distal extent, detect leakage, and identify coincidental pathology. MRA may provide similar detail. Transthoracic echocardiography (TTE) can delineate aneurysm size and extent and detect leakage of aneurysms of the ascending but not descending aorta. TEE cannot show the entire thoracic aorta, but it can be extremely useful in detecting the entry point in aortic dissection.
Contrast angiography provides the best image of the arterial lumen, but it is not the preferred imaging study. It gives no information on extraluminal structures (ie, as an alternative diagnosis), it is invasive, and it has a significant risk of renal and extremity atheroembolism and contrast nephropathy.
Aortic root dilation or unexplained ascending aorta aneurysms warrant serologic testing for syphilis. If a mycotic aneurysm is suspected, bacterial and fungal blood cultures are done.
Diagnosis reference
1. Isselbacher EM, Preventza O, Hamilton Black J 3rd, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2022;146(24):e334-e482. doi:10.1161/CIR.0000000000001106
Treatment of Thoracic Aortic Aneurysms
Control of hypertension and other comorbidities
Endovascular stent grafting or open surgical repair
Immediate control of hypertension is essential.
Medical management with optimal control of hypertension, dyslipidemia, diabetes, and respiratory disease is the appropriate treatment until surgery is indicated. Treatment is endovascular stent grafting when anatomically possible and open surgical repair for more complex aneurysms.
Ruptured TAAs, if untreated, are universally fatal. They require immediate intervention, as do leaking aneurysms and those that cause acute dissection or acute valvular regurgitation.
Transcatheter-placed endovascular stent grafts (endografts) for descending TAAs and thoracoabdominal aortic aneurysms (TAAAs) are a less invasive alternative to open surgery.
Surgery involves a median sternotomy (for ascending and aortic arch aneurysms) or left thoracotomy or thoracoretroperitoneal exposure (for descending and TAAs) and replacement with a synthetic graft. With emergency open surgery, the mortality rate at 1 month is approximately 30 to 50% (1). Patients who survive have a high incidence of serious complications (eg, renal failure, respiratory failure, severe neurologic damage).
Elective surgery is indicated for aneurysms that are
Large
Rapidly enlarging (> 0.5 cm/year)
Causing bronchial compression
Causing aortobronchial or aortoesophageal fistulas
Symptomatic
Traumatic
Mycotic
Aneurysms of the ascending aorta are generally considered large if the diameter is > 5.5 cm or twice the native size of the ascending aorta or if the aortic size index (aortic diameter in relation to body surface area) is ≥ 2.75 cm/m2. In the descending aorta, aneurysms are generally considered large if they are > 6 cm. In patients with Marfan syndrome, large aneurysms are those that are ≥ 4.5 to 5 cm in any location.
Treatment of mycotic aneurysms is aggressive antimicrobial therapy directed at the specific pathogen. Generally, these aneurysms must also be surgically repaired.
Although open surgical repair of an intact TAA improves outcome, mortality rate may still exceed 7% at 30 days (2). The mortality rate is lower with endovascular stent grafts, although life-long surveillance is still required (3). Risk of death increases greatly if aneurysms are complicated (eg, located in the aortic arch or thoracoabdominal aorta) or if patients are older or have coronary artery disease, symptoms, or preexisting renal insufficiency. Perioperative complications (eg, stroke, spinal injury, acute renal failure) occur in about 10 to 20% (4).
Asymptomatic aneurysms that do not meet criteria for elective surgical or endovascular repair are treated with aggressive blood pressure control using a beta-blocker and other antihypertensives if necessary. Smoking cessation is essential. Dyslipidemia, diabetes, and respiratory diseases should all be treated.
Patients require frequent follow-ups to check for symptoms and serial CT or ultrasound every 6 to 12 months. Imaging frequency depends on aneurysm size.
Treatment references
1. Latz CA, Boitano L, Schwartz S, et al. Contemporary mortality after emergent open repair of complex abdominal aortic aneurysms. J Vasc Surg 2021;73(1):39-47.e1. doi:10.1016/j.jvs.2020.03.059
2. Goodney PP, Travis L, Lucas FL, et al. Survival after open versus endovascular thoracic aortic aneurysm repair in an observational study of the Medicare population. Circulation 2011;124(24):2661-2669. doi:10.1161/CIRCULATIONAHA.111.033944
3. Desai ND, Burtch K, Moser W, et al. Long-term comparison of thoracic endovascular aortic repair (TEVAR) to open surgery for the treatment of thoracic aortic aneurysms. J Thorac Cardiovasc Surg 2012;144(3):604-611. doi:10.1016/j.jtcvs.2012.05.049
4. Tanaka A, Leonard SD, Sandhu HK, et al. Open Descending and Thoracoabdominal Aortic Repairs in Patients Younger Than 50 Years Old. Ann Thorac Surg 2019;108(3):693-699. doi:10.1016/j.athoracsur.2019.03.058
Prognosis for Thoracic Aortic Aneurysms
Thoracic abdominal aneurysms enlarge an average of 3 to 5 mm/year. Risk factors for rapid enlargement include larger size of aneurysm, location in the descending aorta, and presence of mural thrombi.
The risk of rupture appears to rise abruptly as TAAs reach 6 cm in diameter. Median diameter at aneurysm rupture is approximately 6 cm for ascending aneurysms and 7 cm for descending aneurysms (1, 2); smaller aneurysms also may rupture, especially in patients with connective tissue disorders or saccular aneurysms.
Survival rate of patients with untreated large TAAs is 25% at 2 years. TAA rupture has a mortality of 97% (3).
Prognosis references
1. Coady MA, Rizzo JA, Hammond GL, Kopf GS, Elefteriades JA. Surgical intervention criteria for thoracic aortic aneurysms: a study of growth rates and complications. Ann Thorac Surg 1999;67(6):1922-1958. doi:10.1016/s0003-4975(99)00431-2
2. Davies RR, Goldstein LJ, Coady MA, et al. Yearly rupture or dissection rates for thoracic aortic aneurysms: simple prediction based on size. Ann Thorac Surg 2002;73(1):17-28. doi:10.1016/s0003-4975(01)03236-2
3. Zvara DA. Thoracoabdominal aneurysm surgery and the risk of paraplegia: contemporary practice and future directions. J Extra Corpor Technol 2002;34(1):11-17.
Key Points
Thoracic aortic aneurysm (TAA) is a ≥ 50% increase in diameter of the thoracic aorta.
TAAs may dissect, compress, or erode into adjacent structures, cause thromboembolism, leak, or rupture.
Median diameter at aneurysm rupture is 6 cm for ascending aneurysms and 7 cm for descending aneurysms.
Diagnosis is often first suspected based on an incidental radiograph or CT finding, and confirmed using CT angiography, magnetic resonance angiography, or transthoracic echocardiography.
Treat small, asymptomatic TAAs with aggressive management of blood pressure and dyslipidemia and smoking cessation.
Treat larger or symptomatic TAAs with endovascular stent grafting when anatomically possible and open surgical repair for more complex aneurysms.







